Transcription
TRAUMA-INFORMEDORGANIZATIONAL CHANGEMANUALsocialwork.buffalo.edu/itticJanuary 2019
THE INSTITUTE ON TRAUMA AND TRAUMA-INFORMED CARE (ITTIC)The Institute on Trauma and Trauma-Informed Care (ITTIC) is a part of the Buffalo Center of Social Researchand University at Buffalo School of Social Work. ITTIC is dedicated to providing the public with knowledge abouttrauma, adversity and its impact, and promoting the implementation of Trauma-Informed Care across variousdisciplines and service settings. Recognizing the centrality of trauma is the key to accomplishing ITTIC’s overallmission of establishing a multidisciplinary trauma-informed system of care, thus ensuring that service systemsare not re-traumatizing the individuals within them.ITTIC was started at the University at Buffalo in 2012 by Research Professor Thomas Nochajski, PhD, and ClinicalProfessor Susan A. Green, LCSW, out of the need for additional trauma-related services, training and supportwithin the community. Since its inception, ITTIC has provided education, training, consultation/coaching andevaluation within adult mental health, criminal justice, developmental disabilities, education and health caresystems.DISCLAIMERThis manual is a product of our many years of research and experience in academic and clinical settings. While our work hasshown us the positive impact trauma-informed approaches can have in all organizations, we understand that it does not replacethe need for individualized care and treatment decisions. Rather, it is intended to work in tandem with other services that can leadto desired outcomes.RIGHTSThis work, with the exception of third party works, is licensed under the Creative Commons Attribution-NonCommercialNoDerivatives 4.0 International License. To view a copy of this license, visit 2019 Institute on Trauma and Trauma-Informed CareUniversity at Buffalo School of Social WorkDOCUMENT AVAILABLE FROMThe Institute on Trauma and Trauma-Informed CareBuffalo Center for Social ResearchSchool of Social Work219 Parker HallBuffalo, NY 14214-8004http://socialwork.buffalo.edu/ittic 2019 The Institute on Trauma and Trauma-Informed Care2
Samantha P. Koury and Susan A. Green from The Institute on Trauma andTrauma-Informed Care (ITTIC) developed the Trauma-InformedOrganizational Change Manual out of a labor of love.AcknowledgementsITTIC gives a special thank you for the supportUniversity at Buffalo, School of Social WorkUniversity at Buffalo, Buffalo Center for Social ResearchITTIC has had the privilege to be guided by those who began to do the work before usITTIC’s Expert Advisory PanelSandra L. Bloom, Associate Professor, Drexel University; Co-Creator of theSanctuary ModelLisa D. Butler, Associate Professor, University at Buffalo School of Social WorkRoger D. Fallot, Director of Research and Evaluation, CommunityConnections;Clinical Faculty, Department of Psychiatry, Yale UniversityLisa M. Najavits, Professor of Psychiatry, Boston UniversityITTIC’s Formation and strategic guidanceTamara B. Owen, PT, MS, MBA, CEO Olmsted Center for SightStephen Kishel, MBA, MBBSamantha and Sue give a special thank you to the followingindividuals who assisted in the creation of this manualContent ConsultantsThomas H. Nochajski, Co-Director, ITTIC; Research Professor, University at BuffaloSchool of Social WorkTravis W. Hales, Assistant Professor, University of North Carolina at CharlotteErin Gurnett, Project Manager/Trainer, ITTICSuzanne L. Bissonette, Executive Director, Cazenovia Recovery Systems, Inc.Samuel Thomas Dodson, Executive Director, Buffalo Psychiatric Center, New YorkState Office of Mental Health (Retired); WNY Trauma Informed Community InitiativeAdvisory CouncilEditing and Design ConsultantsMary F. Burich, Principal, The Auctor GroupJennifer Gogos, President, The Gogos Group 2019 The Institute on Trauma and Trauma-Informed Care3
Pre-ImplementationImplementationSustainabilityThe logo depicts a phoenix rising from the asheswith a mandala in the background.At ITTIC we are committed to working towards healing and re-birthfor people that have experienced trauma in their lives. This image speaks to our work:believing in the strength and resiliency of people to rise out of ashes into wholeness,and believing our systems of care can change to incorporate greater safety,trust, choice, empowerment and collaboration in their work.To read more about the logo below, visit the link here.We have been privileged to be guidedby so many who began to do the work before usand support our efforts now. Thank you to allwho have let us be witnesses to their stories andhave invited us to be part of the journeyto healing, resilience, growth.-The ITTIC Team 2019 The Institute on Trauma and Trauma-Informed Care4
Table of oductionForewordLegacyBackground121515Our ApproachEvaluation–Making Informed Decisions20Guiding Values and Principles–Safety, Trustworthiness,Choice, Collaboration & Empowerment21Re-traumatization – What We KnowThree Levels of a mentation & Sustainability24Trauma-Informed Organizational ModelStages of the Trauma-InformedOrganizational ModelKey Development AreasDomains of Consideration27Getting StartedHow to Use the Manual33Initial Assessment of Stages and KeyDevelopment Areas34Stage 1 – Pre-ImplementationOverview35Key Development Area #1:Leading and Communicating36Key Development Area #2:Hiring and Orientation Practices43Key Development Area #5:Establishing a Safe Environment47 2019 The Institute on Trauma and Trauma-Informed Care5
Key Development Area #8:Collaborating with Partners and Referrals49Key Development Area #9:Reviewing Policies and Procedures51Stage 2 – ImplementationOverview53Key Development Area #1:Leading and Communicating55Key Development Area #2:Hiring and Orientation Practices59Key Development Area #3:Training Clinical and Non-Clinical Staff62Key Development Area #4:Preventing Secondary Traumatic Stress in Staff67Key Development Area #5:Safe Environment71Key Development Area #6:Screening for Trauma75Key Development Area #7:Treating Trauma78Key Development Area #8:Collaborating with Partners and Referrals80Key Development Area #9:Reviewing Policies and Procedures83SustainabilityOverview87Key Development Area #10:Evaluation and Progress Monitoring88Revisiting Key Development Areas #1-990Additional Resources92 2019 The Institute on Trauma and Trauma-Informed Care6
AppendicesAppendix A: Key Development Area Scaling Chart (Full)100Appendix B: Pre-Implementation – Leading and Communicating Scaling Chart107Appendix C: Pre-Implementation – Leading and Communicating Planning Chart109Appendix D: Sample Trauma-Informed Hiring Questions111Appendix E: Pre-Implementation – Hiring and Orientation Practices Scaling Chart113Appendix F: Pre-Implementation – Hiring and Orientation Practices Planning Chart115Appendix G: Pre-Implementation – Establishing a Safe Environment Scaling Chart117Appendix H: Pre-Implementation – Establishing a Safe Environment Planning Chart119Appendix I: Identifying Collaborations Worksheet121Appendix J: Pre-Implementation – Collaborating with Others (Partners and Referrals) Scaling Chart123Appendix K: Pre-Implementation – Collaborating with Others (Partners and Referrals) Planning Chart125Appendix L: Pre-Implementation – Reviewing Policies and Procedures Scaling Chart127Appendix M: Pre-Implementation – Reviewing Policies and Procedures Planning Chart129Appendix N: Sample Trauma-Informed Messaging Posters131Appendix O: Implementation - Leading and Communicating Scaling Chart133Appendix P: Implementation - Leading and Communicating Planning Chart135Appendix Q: Implementation – Hiring and Orientation Practices Scaling Chart137Appendix R: Implementation – Hiring and Orientation Practices Planning Chart139Appendix S: Developing a Training Plan Worksheet141Appendix T: Implementation – Training the Workforce (Clinical and Non-Clinical) Scaling Chart144Appendix U: Implementation – Training the Workforce (Clinical and Non-Clinical) Planning Chart146Appendix V: Implementation – Addressing the Impact of the Work Scaling Chart148Appendix W: Implementation – Addressing the Impact of the Work Planning Chart150Appendix X: Sample Trauma-Informed Environment Walk-Through153Appendix Y: Implementation – Establishing a Safe Environment Scaling Chart159Appendix Z: Implementation – Establishing a Safe Environment Planning Chart161Appendix AA: Implementation – Screening for Trauma Scaling Chart164Appendix BB: Implementation – Screening for Trauma Planning Chart166Appendix CC: Implementation – Treating Trauma Scaling Chart168Appendix DD: Implementation – Treating Trauma Planning Chart170Appendix EE: Implementation – Collaborating with Others (Partners and Referrals) Scaling Chart172Appendix FF: Implementation – Collaborating with Others (Partners and Referrals) Planning Chart174Appendix GG: Checklist for Reviewing Policies and Procedures176Appendix HH: Implementation – Reviewing Policies and Procedures Scaling Chart179Appendix II: Implementation – Reviewing Policies and Procedures Planning Chart181Appendix JJ: Identified Area Scaling Chart183Appendix KK: Action Planning Worksheet185Appendix LL: Sustainability – Evaluating and Monitoring Progress Scaling Chart187Appendix MM: Sustainability – Evaluating and Monitoring Progress Planning ChartAppendix NN: Trauma-Informed Climate Scale-10 (TICS-10)189191References193 2019 The Institute on Trauma and Trauma-Informed Care7
GlossaryManual ntUniversal ExampleEducation ExampleMedical ExampleAcronymsCPT:Cognitive Processing TherapyEMDR:Eye Movement Desensitization and ReprocessingPE:Prolonged ExposureTF-CBT: Trauma-Focused Cognitive Behavioral TherapyTI-EP:Trauma-Informed Educational PracticesTIM:Trauma-Informed Medicine 2019 The Institute on Trauma and Trauma-Informed Care8
TerminologyAdverse Childhood Experiences (ACE) StudyA groundbreaking research study conducted by Dr. Vincent Felitti, Dr. Rob Anda and colleagues that showedthe high prevalence of adversity in childhood (ACEs), and a relationship between ACEs and negative healthoutcomes through the lifespan.BurnoutA gradual process of a staff member experiencing feelings of hopelessness, fatigue and being overwhelmedas a result of a lack of support, excessive workloads and unrealistic expectations.ChampionAn individual or individuals who are trained specifically to take on roles such as educator, trainer, mentor,coach and/or advocate for a trauma-informed approach in order to ensure overall sustainability.Compassion Fatigue (CF)A combination of secondary traumatic stress, vicarious trauma and/or burnout that manifests in a worker.Domains of ConsiderationDomains of organizational change that the Substance Abuse and Mental Health Services Administration(SAMHSA) cross-walked with trauma-specific content and the values and principles of Trauma-InformedCare. These domains provide a framework for organizational change structures within each of thismanual’s key development areas.Guiding Values and PrinciplesA framework and a lens proposed by Dr. Roger Fallot and Dr. Maxine Harris for individuals, organizationsand systems to consider their day-to-day activities in a way that prevents re-traumatization. Includessafety, trustworthiness, choice, collaboration and empowerment.Key Development AreasTen specific aspects of organizational functioning that need to be addressed through a trauma-informedlens to best create overall trauma-informed organizational change; a key component of the traumainformed organizational model.Post-Traumatic Growth (PTG)The process of making meaning out of one’s experience of trauma and experiencing a positive change asa result. 2019 The Institute on Trauma and Trauma-Informed Care9
ResilienceThe process of adapting to trauma and adversity; the ability to bounce back, or return to the level offunctioning before the trauma/adversity occurred.Re-TraumatizationWhen a policy, procedure, interaction, or the physical environment replicates someone’s original traumaliterally or symbolically—triggering the emotions and thoughts associated with the original experience.Sanctuary ModelAn evidence-based approach for changing organizational culture to be more trauma-informed andresponsive that was created by Dr. Sandra Bloom and her colleagues.Secondary Traumatic Stress (STS)The onset of trauma-related symptoms in a worker as a result of witnessing the trauma/adversity ofanother.StagesThe first component of the trauma-informed organizational model that defines the things to consider,needs and resources for trauma-informed organizational change. Includes Pre-Implementation,Implementation and Sustainability.Trauma-InformedOne of the three levels of a trauma-informed approach; the overarching umbrella that provides the filterfor everything we do in a way that ensures universal precaution.Trauma-SensitiveOne of the three levels of a trauma-informed approach; the way that an organization/system/individualresponds to trauma and adversity in a sensitive manner.Trauma-SpecificOne of the three levels of a trauma-informed approach; the trauma-specific treatment interventions.Universal PrecautionSimilar to how health care professionals put on gloves to prevent the spread of blood borne pathogens, atrauma-informed approach involves putting on metaphorical gloves (changing our interactions, policies,etc.) to prevent the possibility of re-traumatization. 2019 The Institute on Trauma and Trauma-Informed Care10
Vicarious Post-Traumatic Growth (VPTG)Development of positive changes and growth in a worker’s world view as a result of witnessing the posttraumatic growth of others.Vicarious Resilience (VR)Positive meaning-making and shift of a worker’s experience as a result of witnessing the resilience ofothers.Vicarious Trauma (VT)The development of negative changes in world view of a worker as a result of the cumulative impact ofwitnessing the trauma/adversity of others over time. 2019 The Institute on Trauma and Trauma-Informed Care11
IntroductionForewordThe purpose of the Trauma-Informed Care Implementation Manual is to helporganizations and systems plan for, implement and sustain Trauma-Informed Care(TIC). The manual is separated into three main sections that will deliberately walkyou through the stages of trauma-informed organizational change and the keydevelopment areas in each stage, and provide resources and examples that canbe used for action planning. This manual serves as both a guide and a workbookby providing opportunities for you to utilize specific tools and worksheets in order toassess your organization/system’s current state and plan for next steps.Our best hope is that this manual will:1Be a means of acknowledging the work your organization/system is engagingin already in response to trauma, and2Provide a framework with guidance for moving forward.The Trauma-Informed Care Implementation Manual is intended for: organizations,systems of care, hospitals, schools and businesses that are considering and/orinterested in implementing a trauma-informed approach.The manual is separated into three main sectionsthat will deliberately walk you through the stagesof trauma-informed organizational change andthe key development areas in each stage. 2019 The Institute on Trauma and Trauma-Informed Care12
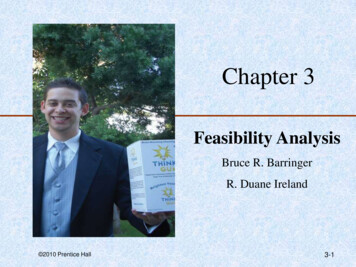
TRAUMA-INFORMED ORGANIZATIONAL YKey Development Areas:Key Development Areas:Key Development Areas:#1: Leading andCommunicating#1: Leading andCommunicating#1: Leading andCommunicating#2: Hiring and OrientationPractices#2: Hiring and OrientationPractices#2: Hiring and OrientationPractices#5: Establishing a SafeEnvironment#3: Training the Workforce(Clinical and Non-Clinical)#3: Training the Workforce(Clinical and Non-Clinical)#8: Collaborating with Others(Partners and Referrals)#4: Addressing the Impact ofthe Work#4: Addressing the Impact ofthe Work#9: Reviewing Policies andProcedures#5: Establishing a SafeEnvironment#5: Establishing a SafeEnvironment#6: Screening for Trauma#6: Screening for Trauma#7: Treating Trauma#7: Treating Trauma#8: Collaborating with Others(Partners and Referrals)#8: Collaborating with Others(Partners and Referrals)#9: Reviewing Policies andProcedures#9: Reviewing Policies andProcedures#10: Evaluation and ProgressDomains of Consideration (SAMHSA, 2014a): Governance and Leadership, Policy, Physical Environment, Engagement andInvolvement, Cross Sector Collaboration, Screening Assessment Treatment Services, Training and Workforce Development,Progress Monitoring and Quality Assurance, Financing, Evaluation 2019 The Institute on Trauma and Trauma-Informed Care13
Adapting to your SystemDifferent systems adapt TIC as an approach to the work they do—which may or may not involve care. Forexample, we have adopted the title of Trauma-Informed Educational Practices (TI-EP) in our work withschools and Trauma-Informed Medicine (TIM) in our work with health care settings. It is important to notethat similarly to how we worked with systems to adapt TIC to TI-EP or TIM, the language in this manual canalways be adapted to your specific system. For the sake of consistency throughout this manual, TI-EP andTIM will be used when discussing examples related to those settings, but otherwise we will use the termtrauma-informed approach.NOTE: Look for the icons below throughout the manual, as they indicate real-life implementation examplesfrom our work in different organizations/systems.UniversalAny organization, system or business, regardless of itsrole/functionTrauma-Informed Educational Practices (TI-EP)Specific to education/schoolsTrauma-Informed Medicine (TIM)Specific to hospitals, primary care and other healthcare systemsFor more details regarding how to use this manual, please read the section on page 32. 2019 The Institute on Trauma and Trauma-Informed Care14
LegacyBeing trauma-informed and providing Trauma-Informed Care (TIC) have their origins in Dr. SandraBloom’s work of creating sanctuary (The Sanctuary Model). Others—notably Dr. Roger Fallot and Dr.Maxine Harris (2001) in their Using Trauma Theory to Design Service Systems: New Directions for MentalHealth Services and Dr. Ann Jennings (The Anna Institute, formally the Anna Foundation)—have contributeda substantial platform for the world to understand, accept and respond effectively to the impacts traumaand adversity have.The comprehensive trauma-informed treatment approaches introduced by Dr. Ricky Greenwald (2005)and Dr. Lisa Najavits (2002) profoundly influence how we treat trauma. The Substance Abuse and MentalHealth Services Administration (SAMHSA)’s (2014) Trauma-Informed Care in Behavioral Health Services(TIP-57) has provided a practical tool for us all.BackgroundTrauma-Informed Care (TIC) is an organizational culture change process that requires the traditionalpower hierarchy to be a more flattened, collaborative environment, while reflecting the paradigm shiftfrom “What is wrong with you?” to “What has happened to you?” in all that we do (Bloom, 1994; Bloom,2013; Harris & Fallot, 2001).Trauma and adversity are growing public health concerns that impact all. Using a trauma-informedapproach in organizations, systems of care, schools, hospitals and businesses is critical to the persistenceof a movement—one of universal precaution, which involves all of us (Bloom & Farragher, 2013, p.29; BurkeHarris, 2014).Universal precaution is often used within the medical field todenote preventative measures of containment of potentiallyhazardous or infectious materials/fluids.When taking universal precaution, a professional approachesall fluid in the same manner without first determining the levelof hazard—generally this is done by putting on gloves or glovingup to protect against exposure.Trauma-Informed Care is also universal precaution in that aprofessional is asked to just assume that all individuals have ahistory of trauma by gloving up metaphorically (i.e., changinginteraction style, policies, procedures, etc.) in order to reducethe possibility of triggering or re-traumatizing others. 2019 The Institute on Trauma and Trauma-Informed Care15
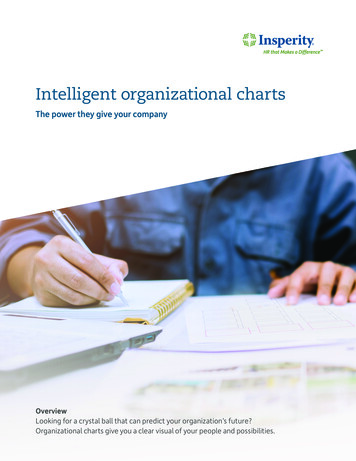
Post-traumatic stress disorder (PTSD)and acute stress disorder (ASD) are thetwo diagnoses related to traumaTrauma and Adversity: What Do I Need to Know?Trauma is conceptualized by considering the events/circumstances that occur, the characteristics ofthose events/circumstances and the negative effect(s) they have on the individual’s well-being. Moreimportantly is the individual’s perception of the event/circumstances, which is ultimately what determinesif it is traumatic or not (SAMHSA, 2014a).Trauma overwhelms an individual’s ability to cope.Post-traumatic stress disorder (PTSD) and acute stress disorder (ASD) are the two diagnoses related totrauma.The Adverse Childhood Experiences (ACE) Study found a relationship between childhood adversity andnegative health outcomes in adulthood (Felitti et al., 1998).The 10 types of childhood adversity (referred to as ACEs) included in the study were: physical, emotionaland sexual abuse, physical and emotional neglect, and growing up in a household with a caretakerwho had a mental illness, abused substances, was incarcerated, was a victim of domestic violence orwas divorced.While ACEs can be considered traumatic, experiencing adversity does not necessarily equal trauma.WORLDVIEWEXPERIENCEPERCEPTIONTRAUMAFigure 1 – What Shapes Trauma 2019 The Institute on Trauma and Trauma-Informed Care16
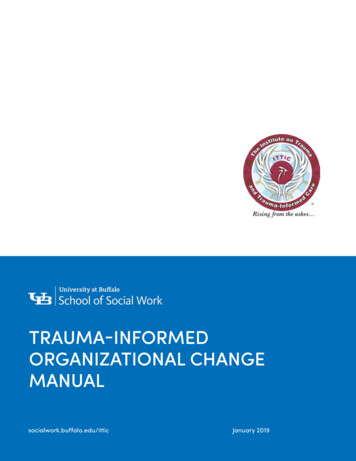
COGNITIVE FUNCTIONINGTrauma/adversity affects one’sability to:Form memoriesLearn and concentrateMake decisionsEMOTION REGULATIONProcess and express languageTrauma/adversity affects one’sability to:Control impulsesInterpret emotional cuesTrust in the reliability of othersWHATHAPPENS?Establish a predictable senseof selfPHYSICAL & MENTAL HEALTHTrauma/adversity affects one’sability of:Developing diabetes, heart disease,cancer and other ailmentsEngaging in substance abuseAttempting suicideDeveloping a sexually transmitteddiseaseRELATIONSHIPSTrauma/adversity affects one’sability to:Identify and form healthyrelationshipsTrust othersExpress needs and wants to othersPERCEPTIONS & BELIEFSSet boundariesTrauma/adversity affects one’s:Core beliefs about self, othersand the worldAbility to hopeFigure 2 – The Imoact of Trauma and Adversity 2019 The Institute on Trauma and Trauma-Informed Care17
Resilience and Post-TraumaticGrowthADVERSEEVENTGROWTHLEVEL OF FUNCTIONINGAs noted in Figure 2, experiencingtrauma/adversity can lead to varyingRESILIENCElevels of impairment and distress. Thereaction could illicit several differentoutcomes:resilience, growth andIMPAIRMENTimpairment. Resilience is the process ofadapting to trauma and adversity—theability to bounce back, or return to thelevel of functioning prior to the trauma/TIMEadversity occurring. When individuals areable to derive meaning from the event orFigure 3 – Trajectories Following Traumacircumstances and experience a positive(Butler, 2010; O’Leary & Ickovics, 1995)change as a result, they undergo whatis called (Tedeschi & Calhoun, 2004). Anexample of PTG is a mother who lost herchild to an accident caused by an intoxicated driver joining Mothers Against Drunk Driving in order toadvocate for and support others.RESILIENCE is the process of adapting to trauma and adversity—the ability tobounce back, or return to the level of functioning prior to the trauma/adversityoccurring.POST-TRAUMATIC GROWTH [PTG] occurs when individuals are able to derivemeaning from the event or circumstances and experience a positive change asa resultExperiencing trauma/adversitycan lead to varying levels of impairmentand distress. The reaction could illicitseveral different outcomes: resilience,growth and impairment. 2019 The Institute on Trauma and Trauma-Informed Care18
Impact of the Work: Considering the WorkforceA trauma-informed entity not only recognizes the effect of trauma on clients/patients/students/consumers,but also the impact on the workforce based on their own and others’ experiences of trauma and/oradversity. Figure 4 below describes those impacts:IMPACTDEFINITIONSecondary Traumatic Stress (STS)Experience of trauma-related symptoms in a worker as a result of witnessingthe trauma/adversity of another; typically quick in onsetVicarious Trauma (VT)Development of negative changes in work world view as a result of thecumulative impact of witnessing trauma/adversity over timeCompassion Fatigue (CF)Experiencing the combination of STS, VT and/or burnoutVicarious Resilience (VR)Positive meaning-making and shift of the worker’s experience as a result ofwitnessing the resilience of othersVicarious Post-Traumatic Growth (VPTG)Development of positive changes and growth in worker’s world view as aresult of witnessing the post-traumatic growth of othersFigure 4 – The Impact of the Work, Adapted from Krause & Green (2015) and Tedeschi & Calhoun (2004)Examples to operationalize some of the concepts above are indicated in Figure 5 below. The impact ofthe work may look different depending on the profession—consider how your organization/system may beimpacted as you read the examples below.SECONDARY TRAUMATIC STRESS: Shortly after interviewing a victim of physical abuse, anurse begins to have a headache and is unable to concentrate, which results in her leavingher shift early.VICARIOUS TRAUMA: A child welfare worker finds herself not wanting to let her daughterout of her sight after taking the position six-months prior because she feels the world is notsafe for children.VICARIOUS RESILIENCE: A teacher reaffirms the reason he decided to go into educationafter witnessing one of his students excel in his classroom despite the struggles she had atthe beginning of the year due to family adversity.VICARIOUS POST-TRAUMATIC GROWTH: A counselor reflects on how he has become morecompassionate and self-aware over the years as a result of witnessing the growth of his clients.Figure 5 – Examples of STS, VT, VR & VPTG 2019 The Institute on Trauma and Trauma-Informed Care19
Our ApproachEvaluationEvaluation is a key component of the trauma-informed approach. It allows us totake a pulse and reassess how trauma-informed we are. Evaluating how traumainformed an organization/system is involves looking at the culture and climate, aswell as its policies and procedures, through a trauma-informed lens. Our evaluationprocess utilizes an organizational assessment tool which asks staff (and sometimesclient/patient/student/consumer) for their perceptions of the five guiding values andprinciples of a trauma-informed approach, and about specific policies/procedureswithin their work at their organization/system that are trauma-informed. There aremultiple trauma-informed organizational assessment tools to choose from, whichwe will discuss later in the manual within the key development areas.Taking a pulse refers to assessing wherean organization/system currently is in thetrauma-informed change process in orderto make informed decisions about next steps.Having a big picture evaluation plan is critical for measuring the progress andoverall success of trauma-informed organizational change. Part of the evaluationplan is taking a baseline, which means evaluating before any trauma-informedtraining or implementation steps occur. The organization/system can then use theresults of the evaluation to make deliberate decisions regarding trauma-informedchange—mainly what to focus energy and resources on first based on reportedstrengths and areas for improvement. In addition to identifying where to start, theorganization/system can also use the baseline evaluation as an anchoring pointto monitor progress moving forward. As can be seen in Figure 6 below, regularmonitoring of progress via evaluation of implementation steps (what is working,what needs to be tweaked, etc.) is the central component of sustaining traumainformed organizational change. Strategies and considerations for creating anoverall evaluation plan will be discussed later in the manual under the Evaluatingand Monitoring Progress section. 2019 The Institute on Trauma and Trauma-Informed Care20
TIONEVALUATIONSUSTAINABILITYFigure 6 – Trauma-Informed Evaluation PlanADJUST PLANAS NEEDEDFive Guiding Values and PrinciplesThe five guiding values and principles proposed by Harris and Fallot (2001) provide a generalframework that can be used in any organization/system with everyone, including at a worker-toclient/patient/student/consumer level, a worker-to-worker level and a leadership-to-worker level.While we strive to incorporate all five to the best of our ability, we may not be able to use all of themin every interaction. As can be seen in Figure 7, the values and principles are unique and stronglyrelated (Hales, Kusmaul & Nochajski, 2016). This means that the values and principles can be usedflexibly. For example, if we truly cannot provide any choice in a specific mandated situation, howcan we at least let the individual know what to expect (trustworthiness) and/or ensure emotionalsafety during the process? Having a good understanding of each of the values and principles iscritical for being able to be deliberate in their use.1. Safety5. Empowerment4. Collaboration2. Trustworthiness3. ChoiceFigure 7 – The Five Guiding Values and Principles Adapted from Harris & Fallot (2001) 2019 The Institute on Trauma and Trauma-Informed Care21
The five values and principles are listed below withdescriptions and examples of what they can looklike in different systems:Safety is broken down intoconsiderations of physical andemotional safety of all individuals inthe organization/system. Physicalsafety involves thinking aboutsecurity and the aesthetics of the bu
coach and/or advocate for a trauma-informed approach in order to ensure overall sustainability. Compassion Fatigue (CF) A combination of secondary traumatic stress, vicarious trauma and/or burnout that manifests in a worker. Domains of Consideration Domains of organizational change that the Substance Abuse a