Transcription
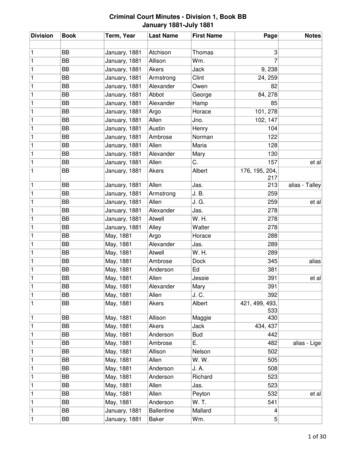
January 2010In this issue:CC Director’s AwardsGingerbread house contest winnersDoppman lecture on cancer visibilityClinical CenterCC pharmacologycourse expandsto ChinaThere is a growing interest in clini cal pharmacology worldwide, givendrug development and drug utiliza tion in therapeutics. China, like otheremerging medical communities, isinterested in establishing a viablepharmaceutical industry base and intraining professionals in the principlesof clinical pharmacology and drugdevelopment sciences.In November, the Clinical Centerand Medical Education was invited byAfter undergoing treatment for chronic myelogenous leukemia, Carlos Carleo was told his chances ofhaving a child with his wife Lilibeth were slim. Now the family, including little Carlos, travel to NIH yearly forfollow-up exams and to participate in a quality-of-life research survey.Finding the new ‘normal’ afterallogeneic stem cell transplantationAs any survivor knows, life doesn’t snapback to the way it was as soon as onehears that coveted “r” word—remission.Nurse researchers at the Clinical Centerare leading a study to examine function,adjustment, quality of life, and symptoms(FAQS) in long-term survivors who haveundergone an allogeneic (from a donor)hematopoietic (blood) stem cell transplant(HSCT).Dr. Margaret Bevans and Dr. SandraMitchell of Nursing and Patient CareServices and their multi-institute studyteam collect survey data once a year fromparticipants to characterize the patternof recovery after this intense treatmentregimen. Understanding the factors thatinfluence variation in these recovery pat terns can help patients know what toexpect over the long term and help clini cians improve services to aid in patients’recovery. “Together with other intramuralresearchers conducting survivorship studieshere on campus, we are contributing tothe evidence base to guide assessment andtailor interventions in transplant survivors,”Mitchell said [see sidebar, page 4].Mitchell and Bevans began their workin 2005, noting gaps in the understand ing of the recovery experience for severalspecific groups of transplant survivors. Asthe researchers noted in their summary ofthe study, most previous research had beencross-sectional (giving a snapshot ratherthan a timline) and had sampled a smallnumber of survivors with limited diversity.”In the FAQS study, Bevans and Mitchell areexamining the extent to which a patient’scondition improves, remains the same,or deteriorates with the passage of timeafter HSCT in a large sample of transplantsurvivors with clinical and demographicdiversity.The National Heart, Lung, and Blood In stitute performed its first allogeneic HSCTin 1993 on patient Javier Egremy-Gracia,who suffered from chronic myelogenousleukemia (CML). His doctors in Mexicoknew of an NIH protocol treating childrenwith the same disease and sent a letter de scribing his case. Dr. A. John Barrett, chiefcontinued on page 4to present its Principles of Clini cal Pharmacology course in Beijing.GlobalMD also welcomed CC DirectorDr. John I. Gallin in 2008 and 2009 toChina to present the CC’s Introduc tion to the Principles and Practice ofClinical Research course.Principles of Clinical Pharmacol ogy faculty members Dr. Juan Lertora,director of CC clinical pharmacology;Dr. Arthur Atkinson, adjunct professorat Northwestern University FeinbergSchool of Medicine Department ofMolecular Pharmacology and formerPrinciples of Clinical Pharmacologycourse director and textbook editor;and Dr. Diane Mould, president ofProjections Research, Inc., taught thecourse over four day-long sessions,November 16 to 19. Guest faculty Dr.Frank Gonzalez, director of the DrugMetabolism Laboratory at the NationalCancer Institute, and Dr. Shiew-MeiClinical Pharmacology at the Food andDrug Administration (FDA), alsoparticipated. Dr. David Flockhart, aPrinciples of Clinical Pharmacologyfaculty member and chief of theDivision of Clinical Pharmacology atthe Indiana University School ofMedicine, also took part in a panel onpharmacogenomics. continued on page 6
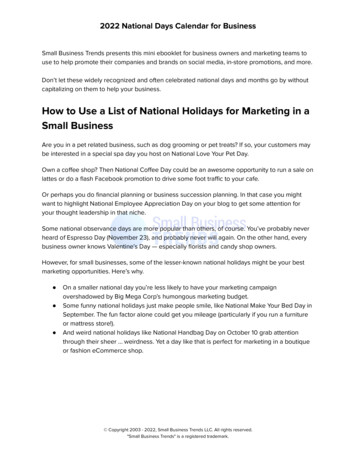
Central Hospital Supply responsible for tools of the tradeBandages, needles, sterile equipment, and isolation carts are neces sary items in any hospital, and the Clinical Center is no different.The group that assures such specialized items are provided to thedepartments of the CC, which has about 7,000 inpatient admis sions and 100,000 outpatient visits a year, is Central Hospital Sup ply (CHS).“We are the hub of this Clinical Center. The doctors and nursescouldn’t do their job without supplies,” said medical supply techni cian Kerry Bruton.CHS, a division of the Materials Management Department,distributes medical-surgical supplies and biomedical equipmentthrough an established system based on historical consumption andan online response system for immediate or unique demands. Anautomated station in virtually every patient-care area—inpatientunits and day hospitals, outpatient clinics, phlebotomy, Radiologyand Imaging Sciences, the Department of Anesthesia and SurgicalServices—and in the Department of Laboratory Medicine maintainsa standard complement of medical-surgical supplies specific to theneeds of each patient-care or service unit.To use the system, clinical staff log on to the station and press atake or return button on the bin of their selected item. This crucialstep links to the CHS inventory to alert staff when they need toreplenish the machine’s supply. Completing this step rather thansimply taking an item or putting one back without registering theaction is crucial to help CHS equip the units with what they need.Larger orders or those for materials not found in the unit’ssupply station (routine or stat requests) come in through the visualsupply catalog, which is constantly monitored. The catalog identi fies by description and photograph the more than 3,000 items inthe supply inventory. This assures that the requestor is clear on theproduct needed and the correct product is sent without delay. Thenext step takes CHS employees to an online inventory database,which reports the desired item’s location in one of the two CHSlocations (Hatfield and Magnuson buildings).Another service of CHS is decontamination and sterilization.Metal and plastic reusable instruments are cleaned, sterilized,inspected, assembled, and packaged as needed. Rows of surgerysupply carts line the hallways, filled with clean instruments readyto picked up for the day’s procedures. CHS also provides technicalsupport on new protocol designs that may include determination ofappropriate sterilization methods or the creation of new instrumenttrays or custom care kits.“CHS, in a team effort, achieves excellence in customer serviceby providing safe medical-surgical supplies in a cost-effective andtimely manner for clinical care and protocol support,” said PaulaWrenn, chief of CHS.This article is part of a series profiling the many Clinical Centerservices that contribute to the advancement and enhancement ofpatient care, research, and training. If you would like your sectionto be featured in an upcoming issue of CCNews, contact editorMaggie McGuire at 301-594-5789 or mcguirema@cc.nih.gov.Clinical Center News ove, Kerry Bruton sends a box of surgical gloves to a patient unitusing the tele-car system. Smaller items travel through the CC’s tubesystem. Such efficiency helps keep the hospital moving. Below, ConnieWilliams, sterile supply technician, organizes metal instruments forsterilization with heat/steam. Her department, Central Hospital Supply,also manages sterilization of items using low temperature methodssuch as ethylene oxide gas and vaporized hydrogen peroxide.Maggie McGuire, editorClinical Center NewsNational Institutes of HealthDepartment of Health and Human ServicesBuilding 10, 10 Center Drive, Room B1L409Bethesda, MD 20892-1504Tel: 301-496-2563 Fax: 301-480-31632 Clinical Center news January 2010Published monthly for Clinical Center employeesby the Office of Communications, Patient Recruit ment, and Public Liaison, Sara Byars, chief.News, article ideas, calendar events, letters, andphotos are welcome.Submissions may be edited.
Exceptional individuals and teams presented CC Director’s AwardsThe 2009 Clinical Center Director’sAwards recognized 98 employees whoembody what is best about the CCfamily—the ability to work creatively,collaboratively, and effectively in carryingout our mission. “Their efforts inspireall of us to renew our commitment todo our best—not only for our patients,but for each other as colleagues work ing toward this common goal,” said CCDirector, Dr. John I. Gallin, at the Decem ber 18 ceremony.AdministrationDr. David Bluemke, director, RIS; SaraByars, chief, OCPRPL; Lillie Coleman,OAM; Mary Hall, CCMD; RebekahGeiger, OD; Dr. Christine Grady, actingdirector, Bioethics; Diane Jenifer, Hos pitality Services; Ann Marie Matlock,NPCS; Colleen McGowan, OAM; PatriciaSengstack, DCRI; Maggi Stakem, OD Nurse Administrative Coordinators(Nursing and Patient Care Services):Courtney Cornell, Rebecca Dove,Chanelle Gutari, Marie-CaroleHenry, Maureen O’Bryan, DonnaOwolabi, Jane Romero, Anita Segar Department of Clinical ResearchInformatics Project Management Of fice: Susan Houston, Ryan Kennedy,Judy Wight, Nicole White BarCoding Initiative Team: CherylClarke, DLM; Elizabeth McNamara, LID Critical Care Medicine Team: Carolea Logun, Melanie Reagan, Dr. Steven Solomon Data Transformation Initiative Team: ErinDominick, OFRM; Chris Epinger, OFRM;Dr. Srini Iyer, OMAR; Dr. Jon McKeeby,chief information officer, DCRI; MelissaMoore, OMAR; Joe Pardi, OFRM; JamesPitts, DCRI; Daniel Rinehuls, OFRM; RachelSchacherer, OD Omnicell Implementation Team: Dr. Mi chael Brown, Pharmacy; Jason Chan, DCRI61. Janice Davis, NPCS; Thomas Dorworth,Pharmacy; Justine Harris, Pharmacy; Dr.Chau Hoang, Pharmacy; Peter Matias,Pharmacy; Jharana Patel, Pharmacy; Anu radha Pendlimarri, Pharmacy; Isolina Ri vera, DCRI; James Schlick, Pharmacy; DavidVinh, DCRI; Christine Yoon, Pharmacy; Dr.Jessica Weintraub, Pharmacy Office of Purchasing and ContractsSmall Business Outreach Team: JaniceBrunson, Malinda Dehner, Maryel Herzog,Susan Huddleston, Jearnean Jack son, Henry Primas, Joe Tewes, DiannaSnowden-Robinson Rehabilitation Medicine Data Trans formation-Activity Management Team:Diane Brandt, Willie Ching, BonnieHodsdon, Donna Gregory, Dr. GalenJoe, Marcia Smith, Michaele Smith, BethSolomon, Lucy SwanTeaching/TrainingDr. Cheryl Fisher, NPCS; Dr. RobertLembo, OCRTME; Dr. Sandra Mitchell,NPCS; Emmanuel Samedi, NPCS; Dr.David Wendler, BioethicsQuality of Worklife/DiversityEsther Wolfrey, RISSpecial RecognitionWilliam Cullen, NIH ORS; AntoinetteRoyster, Patient Advisory Group; DanielWheeland, NIH ORSJesse Ferguson Customer ServiceAwardVicki Chang, OFRM; Maria Guzman,SWD; Mary Haak, OPC; TiffanyHeath, NPCS; Brenda Jimenez,NPCS; Tor Moore, DLM; Mary EllenSavarese, NIH ORSMentoringLynda Ray, OAMPatient CareKathleen Castro, NPCS; Gerard Ja cobs, PET; Shelia Richardson, NPCS;Beverly Smith, NPCS; James Vucich,RISScienceDr. Yuen-Yi “Christine” Hon,Pharmacy; Dr. Elizabeth Rasch,RMD; Nancy Sebring, Nutrition; Dr.Shuibang Wang, CCMDStrategic InitiativesRaymond Bowen, OFM; Dr. JamesCimino, chief, LID; David Folio,chief, Nutrition; John Kocher, DCRISanta makes a stop at the Clinical CenterThe Rehabilitation Medicine Department Recreation Therapy Section hosted a special gueston December 15. Santa Claus made an appearance in the Clinical Center Main Playroom,and to get ready for their time with the jolly old soul, pediatric patients first made a wishlist with Recreation Therapy staff and medical student volunteers. Also there to entertain:The Pipettes, an a cappella group of NIH and Howard Hughes Medical Institute trainees(see page 8). Above, art therapist Megan Robb (right) and Radiology and Imaging Sciencesfellow Hilary Hancock, a Recreation Therapy Section volunteer, work with (from left) RudiBelen, Benjamin Lopez, and Maggie Cobb on their letters to Santa.January 2010 Clinical Center news 3
Survivorship study addresses function after stem cell transplantcontinued from page 1of the NHLBI Hematology Branch StemCell Allogeneic Transplantation Section,performed the transplant with donorcells from Egremy-Garcia’s brother,Alfredo.“My improvement was not immedi ate, but little by little, I started recover ing,” Egremy-Garcia said. In the 16 yearssince his treatment, he says he has feltmostly healthy, except for an infection,three years ago. He suffers from fatigue,peripheral nerve damage, and diabetes,but describes his health as good and isoften too busy with work as a lawyer toschedule follow-up trips to NIH.Mitchell and Bevans’ FAQS studyproceeds in tandem with other intramu ral NIH research examining late effectsof this intense, often curative treatmentfor cancer or a serious bone marrowdisorder. These late effects may includechronic graft-versus-host disease, osteo porosis, endocrine complications, andsecondary cancers.“All typical problems seen in cancersurvivors are multiplied after allogeneicHSCT. Therefore the treatment presentsa unique opportunity for researchers todevelop strategies to address late effectsof cancer therapy,” said Dr. Steven Z.Pavletic, head of the Graft-Versus-Hostand Autoimmunity Unit in the NationalCancer Institute Experimental Transplan tation and Immunology Branch.As nurse scientists, Bevans and Mitch ell are particularly interested in the im pact these late effects may have on howpatients feel and function as they resumeusual activities and roles in their daily lives.In the early period of recovery afteran allogeneic HSCT, patients and familiesare often focused on aspects of physicalrecovery from an aggressive treatmentregimen. As they proceed into the survivor ship phase, other dimensions of well-be ing including mood, relationships, andsymptoms such as fatigue and impairedsleep problems come to the forefront. Theopportunity to complete the study ques tionnaires may help to validate the impor tance of these issues, and “may empowersurvivors to be their own advocates andraise such concerns with the doctors,nurses, and social workers on their trans plant team,” Bevans said.Study results to date suggest that anumber of these dimensions are affectedin transplant survivors. For example, theteam has found that approximately 45percent of study participants had insom nia, and that those with more physical andpsychological symptom distress reportedmore problems with sleep. Survivorsexperiencing difficulties with psychosocialadjustment reported the greatest concernswith immediate and extended family is sues, sexual relationships, and emotionaldistress. Ultimately, Bevans and Mitchellbelieve that a better understanding ofthe factors associated with variability inrecovery can be applied to develop waysto help patients return to a fulfilling andproductive life.“The FAQS study is making majorprogress in this direction, but it onlyaddresses the first step—describingthe scope of the problem. The big nextchallenge is to decide what to do aboutthe problem,” Pavletic said. “Survivorsface a number of challenges affectingtheir health and well-being. Much workremains to be done in this arena, andthe NIH can be a major contributor.”Carlos Carleo is living a life he didn’tknow was possible following his CMLtreatments. As his 4-year-old son playedat his feet, Carleo told his tale of radia tion, chemotherapy, and a HSCT in 1994from his sister’s donor cells. Conceptionafter cancer therapies is rare, but Carleotold doctors he would not freeze hissperm before treatment. “If God wantsme to have kids, I’ll have them.” Carleoand his wife, Lilibeth, call their son, Car los’ namesake, “such a blessing.”He returns to the NIH each year formonitoring and completes the qualitycontinued on next pageNIH intramural researchon late effects ofallogeneic HSCT05-H-0130—Long-Term Evaluationand Follow-Up Care of PatientsTreated with Allogeneic Transplants05-CC-0216—Quality of Life inAllogeneic Transplant Survivors04-C-0281—Natural History Studyof Clinical and Biological FactorsDetermining Outcomes in ChronicGVHD04-NR-0069—Effectiveness ofTopical Thalidomide to Treat ChronicGVHD-related Stomatitis08-C-0097—Montelukast in Treat ing Patient with Bronchiolitis Oblit erans After Stem Cell TransplantContributing to the FAQS study are (from left) Kathleen (Kate) Castro, Olena Prachenko, and Eleftheria(Libby) Koklanaris. Also on the team, but not pictured, is Lisa Cook.4 Clinical Center news January 201008-C-0148—Imatinib Mesylate inTreating Patient with Scleroderma tous Chronic GVHD
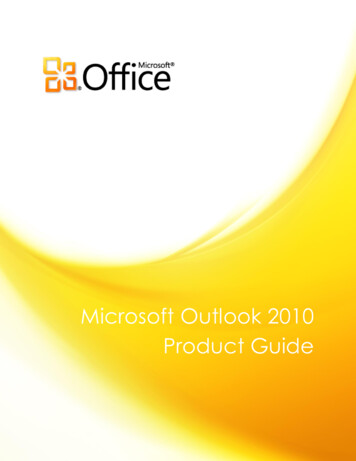
NIH in unique place to continue research in long-term survivorsof-life surveys, reporting everythingis fine. “I like to see the otherpatients and try to lift their spirits,”Carleo said. “I feel very blessed, verylucky.”Another transplant survivor, Nori ne Denise Birckhead had an HCST in1994 after a diagnosis of CML. Thelast 15 years have been a journey,especially the debilitating loss ofindependence during her illness andrecovery. Today, though, Birckheadis healthy and happy to participatein the follow-up protocols. “I hopethey find something that can helpothers,” she said.Mitchell and Bevans report thatpatients are enthusiastic aboutparticipating in survivorship studies,saying that they feel like they arehelping future transplant recipientsand contributing to the mission ofthe NIH to develop new knowledgethat improves outcomes. “The NIHdedicates itself to cases like me the research at the NIH is the reasonI survived,” said Egremy-Gracia.The FAQS study team, including (from left, back) Bazetta Blacklock-Schuver, Nonniekaye Shelburne, Dr. Sandra Mitchell, Patricia Prince, Michael Krumlauf, Dr. Margaret Bevans, and (front) Leslie Wehrlen and CarolineStewart, have seen great participation from NIH HSCT survivors.Doppman lecture presents better visualization of cancerDr. Elliot K. Fishman presented the Ninth Annual John Doppman Me morial Lecture on December 16 to an audience that included the wifeand former colleagues of the late chief of the Clinical Center’s Diagnos tic Radiology Department.Dr. Richard Chang, chief of the Interventional Radiology Section inCC Radiology and Imaging Sciences, profiled Doppman before the lec ture began. Chang mentioned in his mentor’s biography that Doppmansold Good Humor ice cream bars in his youth, included because theformer chief had such a great sense of humor and was so well regard ed by his staff, Chang said.Fishman, professor of radiology and oncology at Johns HopkinsUniversity School of Medicine, and director of the Division of Diagnos tic Imaging and the Division of Abdominal Imaging and ComputedBody Tomography at The Johns Hopkins Hospital, referenced his sharedgoal of Doppman’s—to improve patient care and patient outcomes—inhis lecture “CTA and 3-D Visualization: Its Evolving Role in OncologicImaging.”New technologies that offer arterial and venous views of potentialmalignancies allow for better tracking of transition, texture, and neo vascularity of abnormalities, Fishman said. Such advances in imaging,coupled with advances in surgery, are helping patients with borderlineresectable masses choose a treatment method that favors the best pos sible outcome. “I think in radiology, as Dr. Doppman said 30 years ago,opportunities have never been greater. Challenges have never beenmore difficult, but the future has never been brighter,” said Fishman.Following his speech, Fishman was presented a certificate memo rializing the event by CC Radiology and Imaging Sciences director, Dr.David Bluemke.Dr. Elliot K. Fishman of The Johns Hopkins Hospital presented advancements in oncologic imaging at the JohnDoppman Memorial Lecture in December.January 2010 Clinical Center news 5
Pharmacologytaught in Chinacontinued from page 1“Our Chinese hosts value theleading role of the NIH in bio medical and clinical research andwant to adopt similar standards intheir country,” Lertora said. “Ourtarget audience was made up ofphysicians, pharmacists, basic andclinical pharmacologists, and otherbiomedical scientists working inChinese academic, industrial, andgovernmental institutions.” Hostorganizations were the 307 Hospi tal in Beijing and the Chinese Clini cal Pharmacology Association.Clinical pharmacology is atranslational discipline in the broadfield of clinical research. Once anew molecular entity is discoveredand its effects on biological systemsare defined in cell systems in vitro(outside the body) and in wholeanimal experiments, the entity maybecome a drug candidate. Thus thedrug development process starts:pre-clinical (animal) and clinical (hu man) phases are required to dem onstrate that the drug candidate isboth safe and effective before thedrug is approved by the FDA andis marketed for clinical use. Clinicalpharmacologists are involved in thetranslation of knowledge acquiredin the pre-clinical phase to theclinical phase of drug development,as well as in the conduct of earlyclinical trials—Phase I, for proof ofsufficient safety to be given to hu mans and to define how the drugis handled by the body, and PhaseII, for proof of concept in terms oftherapeutic efficacy.While in Beijing, the coursefaculty were also invited to par ticipate in a special workshop andpanel discussion with their Chinesecounterparts and members of theChinese State FDA that consideredChinese clinical pharmacologyresearch and drug trials regulation,as well as the standards promotedby the US FDA and the NIH for theconduct of clinical research anddrug development studies.Learn more about the Principlesof Clinical Pharmacology courseat .html.6 Clinical Center news January 2010CFC drawing raises 10K for charitiesGina Ford goes in for a celebratory hug with Clinical Center director Dr. John I. Gallinafter winning the CC Combined Federal Campaign (CFC) Basket Drawing’s Stay-cationBasket. Behind them, the CC CFC coordinators cheer on their coworker.Ford, nurse consultant to the CC’s deputy director of clinical care, took hometwo-night stays at The Ritz-Carlton in Washington, DC, and the Doubletree Hotel inBethesda and a 100 American Express gift card.The CFC Basket Drawing offered a chance to win one of 20 themed baskets, con tents donated by various CC departments. Tickets were sold over four days, and thedrawing was held December 3. This year’s drawing raised 10,538 in ticket sales, withall proceeds donated to CFC charities.News briefsMedical arts drops hourly labor rate by more than 25 percentIn a continued effort to meet the needs of the NIH community, Medical Arts now offersa 91 hourly labor rate (previously 125) for medical illustration, express services, designillustration, photomic and photomac services.This reduction in rate affects the cost of design of posters, brochures, publications,and other materials; medical animation or illustration; and close-up and microscopicphotography.Medical Arts has served the NIH community for more than 80 years as part of theOffice of Research Services. For more information on the new rates or any of the Medi cal Arts services, visit http://medarts.nih.gov.A green idea from the Clinical Center Green TeamThe Clinical Center is committed to using natural resources responsibly and that in cludes our use of energy. The NIH Bethesda campus is the largest user of energy inMontgomery County, spending more than 65.5 million on electricity every year.Approximately 10 percent of that is used by the CC, amounting to about 6.5 millionworth of electricity.How can you help get that number down? Contribute to the CC’s commitment toenvironmental stewardship by turning off any unnecessary lights. If you are leaving aroom for more than five minutes, flip the switch to help save the earth.
Kermit and the gang earn 3SE-N first place in gingerbread contestNote to future gingerbread contest entries: pop culture references are acrowd pleaser. Two of the top three immortalized recognizable loca tions—Sesame Street and McDonald’s—in fondant and candies for thesixth annual contest, which pulled 28 submissions made by variousClinical Center departments and more than 2,500 votes.Organized by Ann Marie Matlock of Nursing and Patient CareServices (NPCS), the contest displayed the entries in the CC atrium fora month through the holidays, inviting passersby to vote between De cember 4 and 17 on their pick for most creative and best executed. Dr.David Henderson, deputy director of clinical care, announced the resultson December 18.Laura Kannaian, a member of the winning 3SE-N team, said oftheir Sesame Street-themed work of art, “There are a lot of man hoursin this. It was a total floor effort.” Second place went to the 3SW-Nsteamboat recreation, and completing the third floor sweep was 3NE’sMcDonald’s gingerbread “house.”Partnered with the contest was a food drive to benefit The Children’sInn. Cynthia Herringa, nursing recruitment consultant in NPCS, hascoordinated the drive for the last four years and was pleased with the2009 turnout. “Everyone was very generous this year,” she said.From left, Amy Stewart, Laura Kannaian, and Yvonne Wall were onthe 3SE-N team that created the winning 2009 gingerbread house.NCRR forum promotes workwith academia and industryAbove, second place team from 3SW-N included (from left) Deborah Gutierrez,Bethzaida Matos, Caroline Samedy, Linda Tondreau, and Kinneret Broder. Below,the 3NE team that took third place included (from left) Jennifer Gatt, NicoleRitzau, Shawna Oliver-Wilder, Phyllis Vincent, Diane Aker, Beverly Smith, RebeccaBadu, and Galine Malysheza.The Clinical and Translational Science Award (CTSA)Industry Forum: Promoting Efficient and EffectiveCollaborations among Academia, Government andIndustry on February 17 and 18, hosted by the NationalCenter for Research Resources, will explore ways tostreamline the development of new drugs, devices, anddiagnostics.Both days will begin at 8:00 am in the Natcher Con ference Center (Building 45), and the event is free andopen to the public.NIH Director Dr. Francis Collins will present “WhyIndustry and Academia Should Work Together: An NIHPerspective.” Other speakers from academia, govern ment, nonprofit, venture capital, and industry willdiscuss translational research topics including opportu nities and unmet needs; issues and barriers to drug, di agnostic, and device development; international efforts;and educational curriculum.Poster topic areas will focus on two key areas: translational research collaboration among academia,industry, nonprofit organizations, or government tocomercialize items such as new therapeutics, devices,and diagnostics to improve public health, and prior successful models or new proposed models fortranslational research collaboration among academia,industry, nonprofit organizations, or government.Posters are due by February 1; registration closes onFebruary 5. To register or to submit a poster, visit y 2010 Clinical Center news 7
Upcoming Lectures All will be videocast at http://videocast.nih.gov.January 6, 2010January 13, 2010January 20, 2010January 27, 2010CC Grand RoundsLipsett Amphitheater, 12 noonCC Grand RoundsLipsett Amphitheater, 12 noonCC Grand RoundsLipsett Amphitheater, 12 noonCC Grand RoundsLipsett Amphitheater, 12 noonHuman Subjects Researchand the Internet EraRobert Martensen, MD, PhDDirector, Office of History andMuseum, NIHContemporary Clinical Medicine:Great TeachersTreating Chronic Hepatitis B and CJenny Heathcote, MBBS, MDProfessor of Medicine and FrancisFamily Chair in Hepatology, Universityof TorontoDivision Head, Patient Based ClinicalResearch, Toronto Western ResearchInstituteUpdates in Obesity ResearchGiovanni Cizza, MD, PhD, ScTenure-Track Investigator, ClinicalEndocrinology Branch, Division ofIntramural Research, NIDDKCiliary Diseases: ConvergingObservations and DivergingModelsMeral Gunay-Aygun, MDStaff Clinician, Medical GeneticsBranch, NHGRIUpdates on Therapiesfor Hairy Cell LeukemiaRobert Kreitman, MDChief, Clinical Immunotherapy Section,Laboratory of Molecular Biology, NCIWednesday AfternoonLecture SeriesMasur Auditorium, 3 pmWrong Place, Wrong Time:Understanding Trauma andViolence in the Livesof Young Black MenJohn Rich, MD, MPHProfessor and Chair, Department ofHealth Management and PolicyDirector, Center for Nonviolence andSocial JusticeDirector, Center for Academic PublicHealth PracticeDrexel UniversityWednesday AfternoonLecture SeriesMasur Auditorium, 3 pmProtein Folding: Seeing isDeceivingGeorge Rose, PhDKrieger-Eisenhower Professor ofBiophysics, Johns Hopkins UniversityMeasuring Energy Expenditure inHumans: Tales from the MetabolicChamberKong Chen, PhD, MSCIDirector, Metabolic Research Core,Division of Intramural ResearchTenure-Track Investigator, ClinicalEndocrinology Branch, Division ofIntramural Research, NIDDKGregory G. Germino, MDDeputy Director, NIDDKWednesday AfternoonLecture SeriesMasur Auditorium, 3 pmMolecular Chaperones in ProteinFolding and NeurodegenerationArthur Horwich, MDSterling Professor of Genetics, YaleSchool of MedicineHHMI InvestigatorClinical research trainees share a different talent with CC patientsIn addition to sharing a passion for science andresearch, a group of medical students participatingin year-long mentored research programs at theNIH also share a love for music. These nine, affili ated with either the NIH Clinical Research TrainingProgram (CRTP) or the Howard Hughes MedicalInstitute (HHMI)-NIH Research Scholars Program,formed the a capella singing group The Pipettesand have performed at various events around theClinical Center, most recently in the atrium onDecember 17.“It’s great to connect with patients on a differ ent level then we normally do,” said CRTP fellowAmbereen Kurwa.The group is comprised of musicians with vari ous backgrounds and manages to rehearse twice aweek—once as a large group and once as smallergroups working on individual parts.D
Williams, sterile supply technician, organizes metal instruments for sterilization with heat/steam. Her department, Central Hospital Supply, also manages sterilization of items using low temperature methods such as ethylene oxide gas and vaporized hydrogen peroxide. Ano