Transcription
Summary Report2016 PRC-MCHC CommunityHealth Needs AssessmentAdventist Hinsdale Hospital Service AreaDuPage County, IllinoisPrepared for:METROPOLITAN CHICAGO HEALTHCARE COUNCIL (MCHC)On Behalf of Adventist Hinsdale HospitalBy:Professional Research Consultants, Inc.11326 P Street Omaha, NE 68136-2316www.PRCCustomResearch.com2015-0670-02 December 2015
COMMUNITY HEALTH NEEDS ASSESSMENTTable of ContentsIntroduction4About This Assessment5Methodology5PRC Community Health Survey5Online Key Informant Survey7Public Health, Vital Statistics & Other Data9Benchmark Data10Determining Significance11Information Gaps11IRS Form 990, Schedule H ComplianceSummary of Findings1213Significant Health Needs of the Community14Summary Tables: Comparisons With Benchmark Data15Reading the Data Summary TablesData Charts & Key Informant InputCommunity Characteristics151638Population Characteristics38Social Determinants of Health39General Health Status41Overall Health Status41Mental Health44Death, Disease & Chronic Conditions53Leading Causes of Death53Cardiovascular Disease55Cancer66Respiratory Disease75Injury & Violence81Diabetes91Alzheimer’s Disease98Kidney Disease101Sickle-Cell Anemia104Potentially Disabling Conditions1052
COMMUNITY HEALTH NEEDS ASSESSMENTInfectious Disease111Influenza & Pneumonia Vaccination112HIV114Sexually Transmitted Diseases117Immunization & Infectious Diseases121Births122Prenatal Care122Birth Outcomes & Risks123Family Planning126Modifiable Health Risks129Actual Causes Of Death129Nutrition, Physical Activity & Weight131Substance Abuse149Tobacco Use158Access to Health Services165Lack of Health Insurance Coverage (Age 18 to 64)165Difficulties Accessing Healthcare167Primary Care Services173Emergency Room Utilization177Oral Health178Vision Care183Local Healthcare184Perceptions of Local Healthcare Services184Healthcare Information Sources184Attendance at Health Promotion Events185Resources Available to Address the Significant Health Needs1863
Introduction
COMMUNITY HEALTH NEEDS ASSESSMENTAbout This AssessmentThis Community Health Needs Assessment is a systematic, data-driven approach to determining the healthstatus, behaviors and needs of residents in the service area of Adventist Hinsdale Hospital. Subsequently, thisinformation may be used to inform decisions and guide efforts to improve community health and wellness.A Community Health Needs Assessment provides information so that communities may identify issues ofgreatest concern and decide to commit resources to those areas, thereby making the greatest possible impacton community health status.This assessment was conducted on behalf of Adventist Hinsdale Hospital as part of a larger project sponsoredby the Metropolitan Chicago Healthcare Council (MCHC) by Professional Research Consultants, Inc. (PRC).PRC is a nationally-recognized healthcare consulting firm with extensive experience conducting CommunityHealth Needs Assessments such as this in hundreds of communities across the United States since 1994.MethodologyThis assessment incorporates data from both quantitative and qualitative sources. Quantitative data inputincludes primary research (the PRC Community Health Survey) and secondary research (vital statistics andother existing health-related data); these quantitative components allow for comparison to benchmark data atthe state and national levels. Qualitative data input includes primary research gathered through an Online KeyInformant Survey of various community stakeholders.PRC Community Health SurveySurvey InstrumentThe survey instrument used for this study is based largely on the Centers for Disease Control and Prevention(CDC) Behavioral Risk Factor Surveillance System (BRFSS), as well as various other public health surveysand customized questions addressing gaps in indicator data relative to health promotion and diseaseprevention objectives and other recognized health issues. The final survey instrument was developed by theMetropolitan Chicago Healthcare Council (MCHC) and PRC.Community Defined for This AssessmentThe study area for the survey effort (referred to as the “Adventist Hinsdale Hospital Service Area” in this report,or “AHH Service Area”) is comprised of 88 residential ZIP Codes based on patient origination. This areadefinition is illustrated in the following map.5
COMMUNITY HEALTH NEEDS ASSESSMENTSample Approach & DesignA precise and carefully executed methodology is critical in asserting the validity of the results gathered in thePRC Community Health Survey. Thus, to ensure the best representation of the population surveyed, atelephone interview methodology — one that incorporates both landline and cell phone interviews — wasemployed. The primary advantages of telephone interviewing are timeliness, efficiency and random-selectioncapabilities.The sample design used for this effort consisted of a sample of 1,615 individuals age 18 and older in theAdventist Hinsdale Hospital Service Area. Because this study is part of a larger effort involving multiple regionsand hospital service areas, the surveys were distributed among various strata. Once the interviews werecompleted, these were weighted in proportion to the actual population distribution so as to appropriatelyrepresent the Adventist Hinsdale Hospital Service Area as a whole. All administration of the surveys, datacollection and data analysis was conducted by Professional Research Consultants, Inc. (PRC).For statistical purposes, the maximum rate of error associated with a sample size of 1,615 respondents is 2.5% at the 95 percent level of confidence.Sample CharacteristicsTo accurately represent the population studied, PRC strives to minimize bias through application of a proventelephone methodology and random-selection techniques. And, while this random sampling of the populationproduces a highly representative sample, it is a common and preferred practice to “weight” the raw data toimprove this representativeness even further. This is accomplished by adjusting the results of a randomsample to match the geographic distribution and demographic characteristics of the population surveyed6
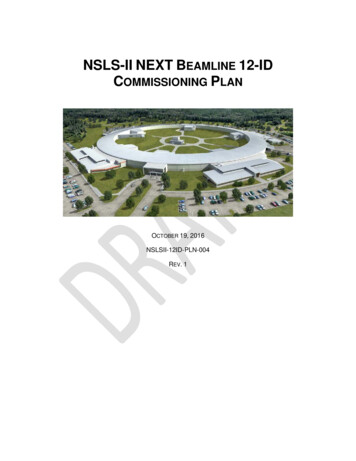
COMMUNITY HEALTH NEEDS ASSESSMENT(poststratification), so as to eliminate any naturally occurring bias.The following chart outlines the characteristics of the Adventist Hinsdale Hospital Service Area sample for keydemographic variables, compared to actual population characteristics revealed in census data. [Note that thesample consisted solely of area residents age 18 and older; data on children were given by proxy by the personmost responsible for that child’s healthcare needs, and these children are not represented demographically inthis chart.]Population & Survey Sample Characteristics(AHH Service Area, 2015)100%Actual 5%Weighted Survey Sample0%MenSources:Women18 to 3940 to 6465 WhiteHispanicOtherCensus 2010, Summary File 3 (SF 3). US Census Bureau.2015 PRC Community Health Survey, Professional Research Consultants, Inc.Further note that the poverty descriptions and segmentation used in this report are based on administrativepoverty thresholds determined by the US Department of Health & Human Services. These guidelines definepoverty status by household income level and number of persons in the household (e.g., the 2014 guidelinesplace the poverty threshold for a family of four at 23,850 annual household income or lower). In samplesegmentation: “very low income” refers to community members living in a household with defined povertystatus; “low income” refers to households with incomes just above the poverty level, earning up to twice thepoverty threshold; and “mid/high income” refers to those households living on incomes which are twice ormore the federal poverty level.The sample design and the quality control procedures used in the data collection ensure that the sample isrepresentative. Thus, the findings may be generalized to the total population of community members in thedefined area with a high degree of confidence.Online Key Informant SurveyTo solicit input from key informants, those individuals who have a broad interest in the health of the community,an Online Key Informant Survey was also implemented as part of this process. A list of recommendedparticipants was provided by MCHC member hospitals; this list included names and contact information forphysicians, public health representatives, other health professionals, social service providers, and a variety ofother community leaders. Potential participants were chosen because of their ability to identify primary7
COMMUNITY HEALTH NEEDS ASSESSMENTconcerns of the populations with whom they work, as well as of the community overall.Key informants were contacted by email, introducing the purpose of the survey and providing a link to take thesurvey online; reminder emails were sent as needed to increase participation. In all, 55 communitystakeholders in the Adventist Hinsdale Hospital Service Area took part in the Online Key Informant Survey, asoutlined below:Online Key Informant Survey ParticipationKey Informant TypeNumber InvitedNumber ParticipatingCommunity/Business Leader8618Other Health (Non-Physician)259Physician303Public Health Expert399Social Services Representative5816Final participation included representatives of the organizations outlined below. A Safe Haven Foundation Austin Childcare Providers Network Better Health Network Chicago Department of Public Health Dominican University Health Services DuPage County Health Department DuPage Federation on Human Services Reform Elmhurst CUSD 205 Enlace Chicago EverThrive Illinois Growing Home, Inc. Housing Forward Illinois Department of Public Health, Bellwood Regional Office Loretto Hospital Metropolitan Chicago Healthcare Council Naperville School District 203 New Moms, Inc. Oak Park Elementary School District Oak Park Township Senior Services PCC Community Wellness Center People’s Resource Center PLOWS Council on Aging8
COMMUNITY HEALTH NEEDS ASSESSMENT Saint Anthony Hospital St. Bernard Hospital and Health Care Center Stickney Public Health Department St. Joseph Services Teamwork Englewood United Way of Metropolitan Chicago Universidad Popular Village of Addison West Humboldt Park Development Council West Side WomenThrough this process, input was gathered from several individuals whose organizations work with low-income,minority populations (including African-American, Arabic, Asian, autistic children, Caucasian, Chinese, thedisabled, the elderly, ethnic minorities, Hispanic, the homeless, immigrants, Indian, LGBT population, lowincome residents, Middle Eastern, multilingual, non-English speaking, Polish, undocumented, uninsured/underinsured, youth), or other medically underserved populations (including African-American, the disabled,elderly, ex-offenders, foreign-born residents, Hispanic, the homeless, immigrants, LGBT community, lowincome, Medicaid/Medicare, the mentally ill, non-English speaking adults, undocumented, uninsured/underinsured, veterans, women, young adults, youth).In the online survey, key informants were asked to rate the degree to which various health issues are aproblem in their own community. Follow-up questions asked them to describe why they identify problem areasas such, and how these might be better addressed. Results of their ratings, as well as their verbatimcomments, are included throughout this report as they relate to the various other data presented.NOTE: These findings represent qualitative rather than quantitative data. The Online Key Informant Survey wasdesigned to gather input from participants regarding their opinions and perceptions of the health of theresidents in the area. Thus, these findings are based on perceptions, not facts.Public Health, Vital Statistics & Other DataA variety of existing (secondary) data sources was consulted to complement the research quality of thisCommunity Health Needs Assessment. Data were obtained from the following sources (specific citations areincluded with the graphs throughout this report): Center for Applied Research and Environmental Systems (CARES) Centers for Disease Control & Prevention, Office of Infectious Disease, National Center for HIV/AIDS,Viral Hepatitis, STD, and TB Prevention Centers for Disease Control & Prevention, Office of Public Health Science Services, Center forSurveillance, Epidemiology and Laboratory Services, Division of Health Informatics and Surveillance(DHIS) Centers for Disease Control & Prevention, Office of Public Health Science Services, National Centerfor Health Statistics Community Commons9
COMMUNITY HEALTH NEEDS ASSESSMENT Connecticut Department of Public Health ESRI ArcGIS Map Gallery National Cancer Institute, State Cancer Profiles OpenStreetMap (OSM) US Census Bureau, American Community Survey US Census Bureau, County Business Patterns US Census Bureau, Decennial Census US Department of Agriculture, Economic Research Service US Department of Health & Human Services US Department of Health & Human Services, Health Resources and Services Administration (HRSA) US Department of Justice, Federal Bureau of Investigation US Department of Labor, Bureau of Labor StatisticsNote that secondary data indicators reflect DuPage County data.Benchmark DataIllinois Risk Factor DataStatewide risk factor data are provided where available as an additional benchmark against which to comparelocal survey findings; these data are reported in the most recent BRFSS (Behavioral Risk Factor SurveillanceSystem) Prevalence and Trend Data published by the Centers for Disease Control and Prevention and the USDepartment of Health & Human Services. State-level vital statistics are also provided for comparison ofsecondary data indicators.Nationwide Risk Factor DataNationwide risk factor data, which are also provided in comparison charts, are taken from the 2013 PRCNational Health Survey; the methodological approach for the national study is identical to that employed in thisassessment, and these data may be generalized to the US population with a high degree of confidence.National-level vital statistics are also provided for comparison of secondary data indicators.Healthy People 2020Healthy People provides science-based, 10-year national objectives for improving the health of all Americans.The Healthy People initiative is grounded in the principle that setting national objectives and monitoringprogress can motivate action. For three decades, Healthy People has established benchmarks and monitoredprogress over time in order to: Encourage collaborations across sectors. Guide individuals toward making informed health decisions. Measure the impact of prevention activities.Healthy People 2020 is the product of an extensive stakeholder feedbackprocess that is unparalleled in government and health. It integrates input from public health and preventionexperts, a wide range of federal, state and local government officials, a consortium of more than 2,000organizations, and perhaps most importantly, the public. More than 8,000 comments were considered in10
COMMUNITY HEALTH NEEDS ASSESSMENTdrafting a comprehensive set of Healthy People 2020 objectives.Determining SignificanceDifferences noted in this report represent those determined to be significant. For secondary data indicators(which do not carry sampling error, but might be subject to reporting error), “significance,” for the purpose ofthis report, is determined by a 5% variation from the comparative measure.Information GapsWhile this assessment is quite comprehensive, it cannot measure all possible aspects of health in thecommunity, nor can it adequately represent all possible populations of interest.It must be recognized thatthese information gaps might in some ways limit the ability to assess all of the community’s health needs.For example, certain population groups — such as the homeless, institutionalized persons, or those who onlyspeak a language other than English or Spanish — are not represented in the survey data. Other populationgroups — for example, pregnant women, lesbian/gay/bisexual/transgender residents, undocumented residents,and members of certain racial/ethnic or immigrant groups — might not be identifiable or might not berepresented in numbers sufficient for independent analyses.In terms of content, this assessment was designed to provide a comprehensive and broad picture of the healthof the overall community. However, there are certainly a great number of medical conditions that are notspecifically addressed.11
COMMUNITY HEALTH NEEDS ASSESSMENTIRS Form 990, Schedule H ComplianceFor non-profit hospitals, a Community Health Needs Assessment (CHNA) also serves to satisfy certainrequirements of tax reporting, pursuant to provisions of the Patient Protection & Affordable Care Act of 2010.To understand which elements of this report relate to those requested as part of hospitals’ reporting on IRSForm 990 Schedule H, the following table cross-references related sections.IRS Form 990, Schedule HPart V Section B Line 1aA definition of the community served by the hospital facilityPart V Section B Line 1bDemographics of the communitySee ReportPage(s)538Part V Section B Line 1cExisting health care facilities and resources within the community that are available to185respond to the health needs of the communityPart V Section B Line 1dHow data was obtainedPart V Section B Line 1fPrimary and chronic disease needs and other health issues of uninsured persons, lowincome persons, and minority groups5AddressedThroughoutPart V Section B Line 1gThe process for identifying and prioritizing community health14needs and services to meet the community health needsPart V Section B Line 1hThe process for consulting with persons7representing the community's interestsPart V Section B Line 1iInformation gaps that limit the hospital facility's11ability to assess the community's health needs12
Summary of Findings
COMMUNITY HEALTH NEEDS ASSESSMENTSignificant Health Needs of the CommunityThe following “areas of opportunity” represent the significant health needs of the community,based on the information gathered through this Community Health Needs Assessment andthe guidelines set forth in Healthy People 2020. From these data, opportunities for healthimprovement exist in the area with regard to the following health issues (see also thesummary tables presented in the following section).Areas of Opportunity Identified Through This AssessmentAccess toHealthcare Services Specific Source of Ongoing Medical Care [65 ] Access to Healthcare ranked as a top concern in the Online KeyInformant Survey. Cancer Deathso Including Female Breast Cancer DeathsCancer Cancer Incidenceo Including Female Breast Cancer Incidence Colorectal Cancer ScreeningDiabetes Prevalence of Borderline/Pre-Diabetes Diabetes ranked as a top concern in the Online Key InformantSurvey.Heart Disease& Stroke Heart Disease & Stroke ranked as a top concern in the OnlineKey Informant Survey.Immunization &Infectious Diseases Pneumonia/Influenza Deaths Hepatitis B VaccinationInjury & Violence Bicycle Helmet Usage [Children] Violent Crime ExperienceMental Health Mental Health ranked as a top concern in the Online KeyInformant Survey.Nutrition,Physical Activity& Weight Low Food Access Nutrition, Physical Activity & Weight ranked as a top concern inthe Online Key Informant Survey.Substance Abuse Overall Alcohol Use Seeking Help for Alcohol/Drug Issues Substance Abuse ranked as a top concern in the Online KeyInformant Survey.14
COMMUNITY HEALTH NEEDS ASSESSMENTSummary Tables:Comparisons With Benchmark DataThe following tables provide an overview of indicators in the Adventist Hinsdale HospitalService Area. These data are grouped to correspond with the Focus Areas presented inHealthy People 2020.Reading the Data Summary Tables In the following charts, Adventist Hinsdale Hospital Service Area results are shown in thelarger, blue column. The columns to the right of the AHH Service Area column provide comparisons betweenlocal data and any available state and national findings, and Healthy People 2020 targets.Symbols indicate whether the service area compares favorably (B), unfavorably (h), orcomparably (d) to these external data.Note that blank table cells signify that data are not available or are not reliable for that areaand/or for that indicator.15
COMMUNITY HEALTH NEEDS ASSESSMENTPSA vs. SSAAHHServiceAreaOverall HealthPSASSA% "Fair/Poor" Physical Healthd16.815.5d17.3dd21.1% Activity Limitations22.5AHH Service Area vs. Benchmarksvs. MCHCRegiond16.620.6d21.4Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.PSA vs. SSAAHHServiceAreaAccess to Health ServicesPSASSA% [Age 18-64] Lack Health 0.96.6% [Insured] Went Without Coverage in Past Year3.9% Difficulty Accessing Healthcare in Past Year (Composite)% Inconvenient Hrs Prevented Dr Visit in Past Year% Cost Prevented Getting Prescription in Past Year10.88.310.9d16.9hvs. eAHH Service Area vs. Benchmarksvs. MCHCRegiond8.15.9vs. ILB7.1d37.6d18.6d12.6vs. ILB19.4vs. USvs.HP2020Bh15.1TREND0.0B8.1d39.9d15.4B15.816
COMMUNITY HEALTH NEEDS ASSESSMENTPSA vs. SSAAHHServiceAreaAccess to Health Services (continued)PSASSA% Cost Prevented Physician Visit in Past 3d12.9Bh2.5% Difficulty Getting Appointment in Past Year% Difficulty Finding Physician in Past Year10.8% Transportation Hindered Dr Visit in Past Year4.2% Skipped Prescription Doses to Save Costs% Difficulty Getting Child's Healthcare in Past Year0.3vs. .3dB6.0B79.0d76.3dd74.4% [Age 65 ] Have a Specific Source of Ongoing Care% Have Had Routine Checkup in Past .5d73.977.1% [Age 18-64] Have a Specific Source of Ongoing CareBdBTREND17.03.6134.1vs.HP2020B8.53.3vs. US18.215.198.6% [Age 18 ] Have a Specific Source of Ongoing Carevs. IL12.09.5Primary Care Doctors per 100,000AHH Service Area vs. Benchmarks80.0B66.5h95.0h89.4h100.0B65.017
COMMUNITY HEALTH NEEDS ASSESSMENTPSA vs. SSAAHHServiceAreaAccess to Health Services (continued)PSASSA% Child Has Had Checkup in Past Yeard90.391.6d89.8dd6.6dd11.9% Two or More ER Visits in Past Year6.0% Rate Local Healthcare "Fair/Poor"11.86.8AHH Service Area vs. Benchmarksvs. MCHCRegionddBArthritis, Osteoporosis & Chronic Back ConditionsPSASSA% [50 ] Arthritis/Rheumatismd33.534.6d33.0dd8.4dd16.7% [50 ] Osteoporosis9.8% Sciatica/Chronic Back Pain18.616.1Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.B16.5BdhbettersimilarworseAHH Service Area vs. Benchmarksvs. MCHCRegionvs. ILdvs. USvs.HP2020TRENDd36.37.9TREND8.9dNote: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.vs.HP2020B84.113.5AHHServiceAreavs. US91.87.511.9PSA vs. SSAvs. e18
COMMUNITY HEALTH NEEDS ASSESSMENTPSA vs. SSACancerPSASSAAHHServiceArea149.3Cancer (Age-Adjusted Death Rate)AHH Service Area vs. Benchmarksvs. MCHCRegionB169.236.5Lung Cancer (Age-Adjusted Death Rate)vs. ILB174.2B47.517.7Prostate Cancer (Age-Adjusted Death Rate)B20.524.2Female Breast Cancer (Age-Adjusted Death Rate)h22.812.5Colorectal Cancer (Age-Adjusted Death Rate)B15.9148.0Prostate Cancer Incidence per 100,000B156.2140.6Female Breast Cancer Incidence per 100,000h129.460.6Lung Cancer Incidence per 100,000B64.841.0Colorectal Cancer Incidence per 100,0005.7Cervical Cancer Incidence per 2% Skin Cancerd149.4vs. US7.86.719
COMMUNITY HEALTH NEEDS ASSESSMENTPSA vs. SSAAHHServiceAreaCancer (continued)PSASSA% Cancer (Other Than .2dd67.25.2% [Men 50 ] Prostate Exam in Past 2 Years% [Women 50-74] Mammogram in Past 2 Years% [Women 21-65] Pap Smear in Past 3 Years% [Age 50-75] Colorectal Cancer Screening63.16.8AHH Service Area vs. Benchmarksvs. MCHCRegionvs. ILvs. USddd5.2dd79.1h84.668.8Chronic Kidney DiseasePSASSA13.0Kidney Disease (Age-Adjusted Death Rate)% Kidney Diseased3.1d2.9Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful NDd69.2Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.PSA vs. ttersimilarworseAHH Service Area vs. Benchmarksvs. MCHCRegionBvs. ILBvs. .72.4TREND14.53.020
COMMUNITY HEALTH NEEDS ASSESSMENTPSA vs. SSADementias, Including Alzheimer's DiseasePSASSAAHHServiceArea19.9Alzheimer's Disease (Age-Adjusted Death Rate)AHH Service Area vs. Benchmarksvs. MCHCRegionh16.4Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.PSA vs. SSADiabetesPSASSA11.3Diabetes Mellitus (Age-Adjusted Death Rate)% Diabetes/High Blood Sugar% 7% [Non-Diabetes] Blood Sugar Tested in Past 3 YearsAHHServiceArea50.754.4Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.dvs. eAHH Service Area vs. Benchmarksvs. MCHCRegionBvs. ILB19.319.4dh11.58.3vs. IL9.9dvs. 9.2Bdhbettersimilarworse21
COMMUNITY HEALTH NEEDS ASSESSMENTPSA vs. SSAEducational & Community-Based ProgramsPSASSA% Attended Health Event in Past Yeardd19.7AHHServiceArea21.722.4AHH Service Area vs. Benchmarksvs. MCHCRegiondFamily PlanningPSASSAAHHServiceArea23.1% Unwed Mothers3.4% Teen Birthsvs. MCHCRegionHearing & Other Sensory or Communication DisordersPSASSA% Deafness/Trouble Hearingdd10.08.1Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.8.6TREND23.8BdhbettersimilarworseBvs. ILBvs. ilarworseNote: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.AHHServiceAreavs.HP2020AHH Service Area vs. Benchmarks7.2PSA vs. SSAvs. USd21.1Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.PSA vs. SSAvs. IL7.67.84.3AHH Service Area vs. Benchmarksvs. MCHCRegionvs. ILhvs. USvs.HP2020TRENDd6.710.3Bdhbettersimilarworse22
COMMUNITY HEALTH NEEDS ASSESSMENTPSA vs. SSAHeart Disease & StrokePSASSAAHHServiceArea133.0Diseases of the Heart (Age-Adjusted Death Rate)AHH Service Area vs. Benchmarksvs. MCHCRegionB172.030.8Stroke (Age-Adjusted Death Rate)B35.4% Heart Disease (Heart Attack, Angina, Coronary 094.6d95.2B93.096.7h91.7d32.635.1d31.8dd88.24.9% Stroke3.2% Blood Pressure Checked in Past 2 Years% Told Have High Blood Pressure (Ever)% [HBP] Taking Action to Control High Blood Pressure% Cholesterol Checked in Past 5 Years% Told Have High Cholesterol (Ever)% [HBC] Taking Action to Control High Blood . USd5.42.088.1vs. IL89.2B74.0B36.6B86.6d29.9B82.1h13.5B81.423
COMMUNITY HEALTH NEEDS ASSESSMENTPSA vs. SSAHeart Disease & Stroke (continued)PSASSA% 1 Cardiovascular Risk Factordd83.2AHHServiceArea80.980.1AHH Service Area vs. Benchmarksvs. MCHCRegiondHIVPSASSAAHHServiceArea80.2HIV Prevalence per 100,000d27.4d22.2Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful eAHH Service Area vs. Benchmarksvs. MCHCRegionB449.1% [Age 18-44] HIV Test in the Past Yearvs. USd80.9Note: In the green section, eachservice area is compared againstthe other. Throughout thesetables, a blank or empty cellindicates that data are notavailable for this indicator or thatsample sizes are too small toprovide meaningful results.PSA vs. SSAvs. ILvs. ILB300.1dvs. USvs.HP2020TRE
Dominican University Health Services DuPage County Health Department DuPage Federation on Human Services Reform Elmhurst CUSD 205 Enlace Chicago EverThrive Illinois Growing Home, Inc. Housing Forward Illinois Department of Public Health, Bellwood Regional Offi