Transcription
WoundAssessment andMeasurementContent Creators:Members of the South West Regional Wound Care Program’sClinical Practice and Knowledge Translation Learning CollaborativeLast updated: August 28, 2015
Learning Objectives2. Describe various common data collection anddocumentation forms, and why and how to use them3. Understand how to assess common wound characteristicsSouth West Regional WoundCare Program1. Explain the importance and frequency of accurate woundassessments2
Photographs and IllustrationsSouth West Regional WoundCare ProgramImages/illustrations obtained via Google Images, unlessotherwise stated3
South West Regional WoundCare ProgramWOUND ASSESSMENT AND DATACOLLECTION AND DOCUMENTATION4
What is Wound Assessment1? Systematic process of assigning numbers or grades to thewound/wound characteristics during an examination. Thisprocess includes: Instruments or means the wound/wound characteristics aremeasured/assessed Examination: Process of determining the values of the tests Evaluation: Process of making clinical judgments based on the data obtainedfrom the examSouth West Regional WoundCare Program Tests:5
Wound Assessment: Purposeand Frequency1 Examine the severity of the lesionDetermine the status of wound healingEstablish a baseline for the woundPrepare a plan of careReport observed changes in the wound over time Frequency: Assessment is done with/of a person with a wound before implementingspecial tests/examinations and before implementing interventions toensure that only medically necessary, reasonable, and appropriatecare/treatments/services are provided Re-assess at regular intervals to measure change in status of wound,ideally each time the dressing is changed, using the same tests selectedfor the initial assessmentSouth West Regional WoundCare Program Purpose:6
Wound Assessment:Procedure1 Information collection easier, better organized, moreconsistent when collected on form Use of standardized forms ensures that important informationis not lost Most common form is ‘Wound Care Flow Sheet’South West Regional WoundCare Program Use a standardized data collection and documentation formsthat list the significant skin and wound features at baseline andthat will be tracked over the course of care7
Wound Assessment1 Periwound skin attributes Wound tissue attributes Wound exudate characteristics Examples of valid, reliable wound healing tools: Pressure Ulcer Scale for Healing (PUSH) Bates-Jensen Wound Assessment Tool (BWAT) Photographic Wound Assessment Tool (PWAT)South West Regional WoundCare Program Recording method should allow for tracking of eachassessment item over time, in objective terms and show thechanges in the wound status, including:8
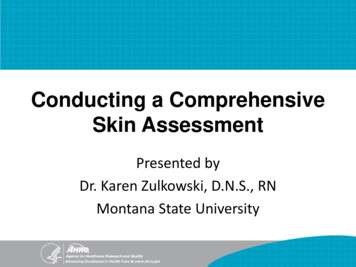
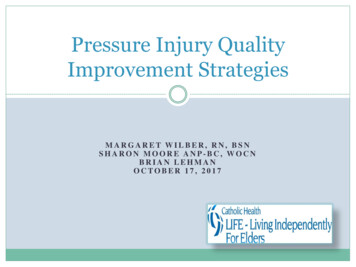
Pressure Ulcer Scale forHealing (PUSH Tool)1 Tool assesses three components: Surface area measurement (scored from 0-10) Exudate amount [scored from 0 (none) to 3 (heavy)] Tissue type [scored from 0 (closed) to 4 (necrotic tissue)]South West Regional WoundCare Program Developed by the National Pressure Ulcer Advisory Panel(NPUAP) 1996 to address practice of back staging pressureulcers9
PUSH Continued1 Studies have found the tool to have content validity,correlation validity, prospective validity, and to be sensitive tochange5-8 Tool has been validated to assess healing of venous anddiabetic foot ulcers in addition to pressure ulcers32South West Regional WoundCare Program To ensure consistency, definitions for each scored item arefound at the bottom of the tool10
South West Regional WoundCare ProgramPUSH Tool 3.011
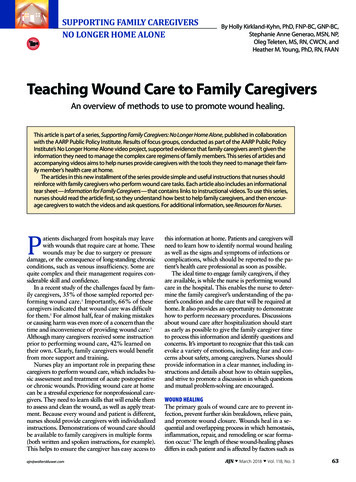
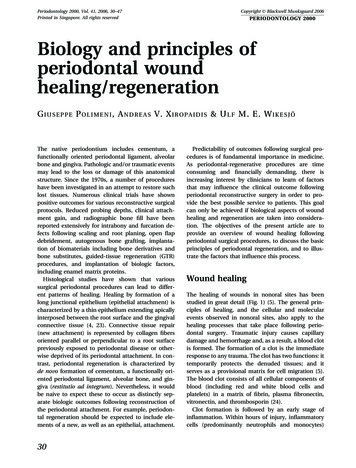
Bates-Jensen WoundAssessment Tool (BWAT) Evaluates 13 wound characteristics with a numerical ratingscale and rates from best (1) to worst (5) Total score ranges from 13 (skin closed) to 65 (profound tissuedegeneration) – watch total score to see if wound healing or not Has evolved to include measuring and predicting woundhealingSouth West Regional WoundCare Program Adapted from the Pressure Sore Status Tool9 by Barbara BatesJensen12 Average content validity 0.6210
South West Regional WoundCare ProgramBWAT Tool13
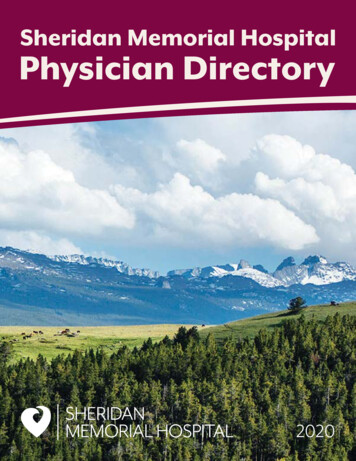
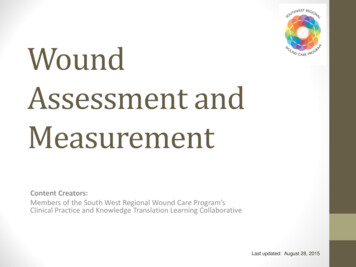
Photographic WoundAssessment Tool (PWAT) Consists of 6 items: edges, necrotic tissue type, necrotic tissueamount, skin color surrounding wound, granulation tissue,and epithelialization Scored 0 – 24 Valid, reliable, and responsive14-16South West Regional WoundCare Program Developed by wound care clinicians and researchers byextracting the Pressure Sore Status Tool subscales that couldbe evaluated from photographs14
South West Regional WoundCare ProgramPWAT15
Data Collection Forms Depending on the person’s medical diagnosis and/or medicalimpairments, multiple assessment forms may be required, i.e.: Initial Wound Assessment ScreenInterdisciplinary Lower Leg Assessment FormInterdisciplinary Diabetic/Neuropathic Foot Assessment FormInterdisciplinary Pressure Ulcer Contributing Factors Assessment ToolSouth West Regional WoundCare Program Regardless of the form you use to collect findings, all attributeson the form must be assessed16These forms and their instructions can be found online at:swrwoundcareprogram.ca
South West Regional WoundCare ProgramASSESSMENT OF WOUND CHARACTERISTICS17
Wound Characteristics LocationAge of woundSize of woundStage or depth of tissue involvementUndermining or tunnelingNecrotic tissueGranulation tissueEpitheliumExudatesSouth West Regional WoundCare Program Wound characteristics1:18
Location1 Where the wound occurs on the person’s anatomy Use anatomic terms Identify with letters, i.e. wound A, B, C Use references such as lateral, medial, proximal, distal, etc. Measure as a single woundSouth West Regional WoundCare Program If there are multiple wounds in a similar location:19
Wound Location1 Location may help determine etiology, i.e.: Venous ulcers: Arterial ulcers: Lower leg dorsum Foot, lateral border of foot, toe joints Malleolus Neuropathic ulcers: Plantar surface of foot and heel Metatarsal heads Lateral border of foot and mid-foot deformitiesSouth West Regional WoundCare Program Above ankle Medial lower leg20
South West Regional WoundCare ProgramWhere Are These Wounds?21
AnswersRight foreheadDorsum of the lefthandLeft medialmalleolusMid-abdominalincisionSouth West Regional WoundCare ProgramCoccyx22Right BKA stump
Age of Wound Describe in terms of days, weeks, months, years Acute – less than four weeks old Chronic – greater than four weeks old Age of the wound will help guide treatment and will informyou re the ‘healability’ of the woundSouth West Regional WoundCare Program The age of the wound will help you to determine whether thewound is:23
Size of Wound Three components: Area Depth Volume No current gold standard for wound measurement Measurements of wound size important to providers, payers,regulators, patient – your best legal defenseSouth West Regional WoundCare Program Accurate, complete, uniform, and consistent wound sizemeasurements required to establish diagnosis, plan of care,and to evaluate24
Tips to Measure More Accurately1 Take measurements the same way each time from noted reference point onthe body Use same units of measure and terminology for each measurement Have same person take measurementsSouth West Regional WoundCare Program Define specific procedures to determine: Wound edge Total wound area Use an assistant to record measurements Use a prepared form25
Wound Area24 Ruler methodAcetate tracingDigital tracingsWound photography Regardless of the method used, it should be consistentlyapplied, and the results should be meticulously documentedto assess progress of healing Wound surface area (l x w) is a geometric formula for arectangle – can inflate the area of the wound up to 44%South West Regional WoundCare Program A variety of methods are available to measure wound area:26
Ruler Measurement24 Simple, inconsistent Accuracy is increased by taking an average of threemeasurements Surface Area Measurement: The longest length The greatest width perpendicular to it Multiply length x width for surface areaSouth West Regional WoundCare Program Not reliable for irregular or large wounds27
South West Regional WoundCare ProgramWound AreaLongest lengthXWidest perpendicular axis28
South West Regional WoundCare ProgramWhere is the Length/Width?29
South West Regional WoundCare ProgramLocation Answers30
Acetate Tracing24 When tracing is made on metric graph paper, it’s calledplanimetry. Size is determined by counting graph squares Tracing can become a wound map, showing different areas ofnon-viable tissue and areas of undermining Commonly used on flat wounds, limited use on full thicknesswoundsSouth West Regional WoundCare Program Tracing of a wound shape on acetate paper – repeatedtracings show changes in size/shape over time31
Tracings24 Easy to learnInexpensiveReadily availableRequires minimal training Inaccuracy from: Estimating partial squares Tracing of wound edgesSouth West Regional WoundCare Program Benefits:32
Digital Tracings1 Benefits: Tablet can calculate wound area and % change size for youSimple to handle and useMinimizes risk of contamination (multilayer acetate)Tablet is portable, light weight, can be disinfectedCan track undermining, epithelialization, % of tissue types94% accuracy, more consistent and reliable measurementsSouth West Regional WoundCare Program Acetate tracing plus a digitizing tablet, i.e. Visitrak (Smith andNephew)33Click on the Visitrak to watch a video on how it works!
Wound Photography1 Prevent litigationPermanent record of woundSerial photos can show progression towards healing, can be used asteaching toolReliable, accurate, improves measurement consistencyNo contaminationNo damage to wound bedLess painful Disadvantages/challenges: Need consentLighting may affect color of wound characteristicsDifficulty measuring wounds on a curved surfaceCost of cameraSouth West Regional WoundCare Program Benefits:34
Use good lighting sourceScreen private areas from the cameraPosition ruler to show relative sizeUse a string of known length and position camera from woundthe same distance every time Use id signs with pt. id, wound location, and date Use a ring flash attachment to reduce shadows Use an assistant to position the person and id signSouth West Regional WoundCare ProgramTips for Good Photos135
Using Wound Measurements toTrack Healing1 The precision of wound measurement and the method ofcalculating the rate of change can influence clinical decisionsSouth West Regional WoundCare Program Wound care providers must regularly re-evaluate the rate ofwound surface area closure to help determine whether or notthe wound is closing at an expected rate36
Calculating % Reduction in WoundSize Over Time1 Specific wound closure rates based on wound etiology:Etiology% Reduction in Surface Area as aPredictor of Wound HealingVenous Leg Ulcer25 28.79% at 4 weeks will close by 24weeksDiabetic Foot Ulcer26-27 50% a 4 weeks will close by 12 weeksPressure Ulcer28-30 39% after 2 weeks will close morequicklyOpen Surgical Wound (average size of10cm2)3150% at 13 days will close by 21 daysSouth West Regional WoundCare Program In general, a 20-30% reduction in surface area over a three tofour week period is a reliable predictive indicator of chronicwound healing37
Calculating % Surface AreaReductionXNOTE: Surface area length x width (in centimeters)100 % reductionSouth West Regional WoundCare ProgramSurface Area (admission) – Surface Area (current)Surface Area (admission)38
Calculation PracticeWound Admission Surface Area Surface Area at One MonthA15 cm223.7 cm2B22.4 cm29.2 cm2C76.3 cm266.9 cm2D3.1 cm25.2 cm2South West Regional WoundCare Program What is the % reduction in wound surface area for thefollowing wounds:39
Calculation Practice AnswersWoundAdmission Surface AreaSurface Area at One Month% ChangeA15 cm223.7 cm2 58%B22.4 cm29.2 cm258.9%C76.3 cm266.9 cm212.3%D3.1 cm25.2 cm2 66.7% Which wound is closing at an expected rate (i.e. 20-30% over aperiod of 3-4 weeks)?South West Regional WoundCare Program What is the % reduction in wound surface area for thefollowing wounds:40
Wound Surface Area The wound should continue to progressively close as it movesthrough the phases of wound healing If a ‘healable’ wound is not getting smaller, a full reassessmentof the cause and corrective therapies needs to occur If despite reassessment and implementation of best practicesa wound continues to fail to proceed towards closure in atimely manner, advanced therapies may need to beconsideredSouth West Regional WoundCare Program In general, the wound surface area should initially reducerapidly and then slow41
Wound Depth1 Distanced from the visible skin surface to the wound bed Crude method of tracking growth of granulation tissue Methods: Find deepest site and measure Clock methodSouth West Regional WoundCare Program Associated with extent of tissue damage42
The Clock Method1 12 o’clock3 o’clock6 o’clock9 o’clockSouth West Regional WoundCare Program Take depth measurements at:43
Wound Volume1 Difficult, usually limited to research studies Filling the wound with a measured amount of saline Pouring Jeltrate (alginate hydrocolloid used by dentists) into thewound, making a mold Significant inaccuraciesSouth West Regional WoundCare Program Two methods:44
Indistinct, diffuse Unable to distinguish wound outline clearly Normal tissues have blended into the wound bed Attached Even or flush with the wound base, no sides or walls present, flat Unattached Sides or walls are present; floor or base of wound is deeper than edge Rolled under, thickened Soft to firm and flexible to touch Hyperkeratosis Callus like tissue formation around wound and at the edgesSouth West Regional WoundCare ProgramWound Edges145
South West Regional WoundCare ProgramHow Would You DescribeThese Wound Edges?46
Wound Edge AnswersUnattachedSouth West Regional WoundCare ProgramAttached47Hyperkeratotic,Indistinct
Tunnelling1 A separation of the fascial planes leading to sinus tracts Usually narrow and long, and seems to have a destinationSouth West Regional WoundCare Program Usually involves a small % of the wound margins48
Undermining1 Usually involves a greater % of the wound margins, with moreshallow length than tunneling An erosion under the edge of the woundSouth West Regional WoundCare Program Usually involves subcutaneous tissues49
South West Regional WoundCare ProgramTunnel or Undermining?50
Undermining/Tunneling AnswersTunnelingSouth West Regional WoundCare ProgramUndermining51UnderminingTunneling
Measuring Undermining1 Method #1: Connect the points and measure length and width, multiplying tocalculate the overall undermined estimateSouth West Regional WoundCare Program Map undermining around the entire wound perimeter by using aprobe and marker52
Undermining Measurement1 Method #2: A.K.A. The Sussman MethodSouth West Regional WoundCare Program Using four cardinal points of the clock53
Necrotic Tissue1 Impairs wound healing as it: The more non-viable tissue there is in a wound: The more severe the underlying damage The longer it will take to close the woundSouth West Regional WoundCare Program Is a physical barrier to granulation, contraction and reepithelialization Can harbor bacteria54
Necrotic Tissue Color: White/gray Yellow fibrinous Yellow/tan (slough) Black/brown (eschar) Consistency: Mucinious Soft, stringy Soft, soggy Hard Adherence: Clumps Loosely attached Attached at base only Firmly adherent at base and edgesSouth West Regional WoundCare Program As tissue dies, it changes in color, consistency and adherence to the wound bed55
Red/Yellow/Black System33Red Wound bed is clean and tissue is red/pink Goal: maintain moist wound healing environment Wound bed has slough/fibrin present and tissue may be combo ofred/pink ivory/canary yellow/green (depending if infection ispresent)Yellow Not all yellow is bad – granulation grows through yellow fibrin andhealthy tendon may appear as white/yellow Goal: maintain moist environment whilst managing excess exudateand remove sloughBlack Non-viable tissue present. Color may be dark brown/black/grey /red/pink /- canary yellow/green Goal: remove non-viable tissue, except stable eschar on a heelSouth West Regional WoundCare Program The type of non-viable tissue present can help identify thephase of wound healing that the wound is in, and as such, canhelp to direct treatment options.56
Necrotic Tissue Amount 25%25 50% 50 75%75 100%South West Regional WoundCare Program Use clinical judgment to estimate the percentage of thewound covered with necrosis in quarters. i.e.:57
Types of Necrotic Tissue Indicates less severityYellow to tan mucinous or stringy materialLoosely adherent to wound bedIf non-adherent will be scattered through out wound Eschar Indicates deeper tissue damageBlack, gray, brown in colorUsually adherent or firmly adherentMay be soggy and soft or hard and leatherySouth West Regional WoundCare Program Slough58
South West Regional WoundCare ProgramDescribe This Necrotic Tissue59
Necrotic Tissue AnswersSloughSloughEscharSouth West Regional WoundCare ProgramEschar60
Granulation Tissue1 Healthy when bright, beefy red, shiny, and granular with avelvety appearance A paler appearance with spontaneous bleeding may indicateischemia, infection, or a co-morbidity such as anemiaSouth West Regional WoundCare Program The growth of small blood vessels and connective tissue intothe wound cavity61
Granulation Tissue Continued1 A building up of tissue that prevents epidermal migration orresurfacing across the wound, by proliferating above the intactmargins of the skinSouth West Regional WoundCare Program Hypergranulation may indicate excessive moisture at thewound surface62
Granulation Tissue Amount 25%25 50% 50 75%75 100%South West Regional WoundCare Program Use clinical judgment to estimate the percentage of thewound filled with granulation in quarters. i.e.:63
Epithelial Tissue1 Process of epidermal resurfacing May migrate from islands on the wound surface, the woundedges, or bothSouth West Regional WoundCare Program Appears as red or pink skin64
Epithelial Tissue Amount 25%25 50% 50 75%75 100%South West Regional WoundCare Program Use clinical judgment to estimate the percentage of thewound covered with epithelium in quarters. i.e.:65
Exudate1 The term given to the fluid that leaks from a wound Wound etiologyWound healing physiologyWound environmentCompounding pathological factors Asses color, consistency, amount and odor by looking at: The wound itself, post wound cleansing and debridement The dressingSouth West Regional WoundCare Program Exudate characteristics are influenced by:66
Exudate Color and Consistency1Color and ConsistencySerousClear/light yellow, thing/waterySero-sangPink light red, thin/waterySangBright red, thin/wateryPurulentDarker yellow/tan or blue/green,thin thick, watery opaqueImageSouth West Regional WoundCare ProgramExudateDescriptor67OtherSome dressings and topicals canalter the appearance of exudate,i.e. silver, cadexomer iodine, etc.
Exudate AmountDefinitionNoneNo visible exudate on the dressing or on the wound.ScantNo measurable exudate on the dressing; however the woundtissues are moist.Small 25% of the dressing has drainage on it Wound tissues are visibly moist Moisture is evenly distributed in the woundModerateLarge Drainage involves 25% to 75% of the dressing Wound tissues are saturated Moisture is/isn’t evenly distributed in the wound Drainage involves 75% of the dressingWound tissues are saturatedDrainage is freely expressed from the tissueMoisture is/isn’t evenly distributed in the woundSouth West Regional WoundCare ProgramDescriptor68
Exudate Odor1 No standard terminology All occluded wounds have an odor Necrotic tissue in a wound contaminated with anaerobes mayproduce a foul odor Pseudomonas has a sickening sweet odor along with blue/greenexudate Odor is significant when it is new orwhen it has changedSouth West Regional WoundCare Program Odor69
TendonVesselsCapsuleBoneNerveSouth West Regional WoundCare ProgramAnatomical StructuresMuscle70
South West Regional WoundCare ProgramSWRWCP Wound AssessmentResources71
Review1. The importance of accurate wound assessment3. Assessment of common wound characteristicsSouth West Regional WoundCare Program2. Common data collection and documentation forms, and whyand how to use them72
South West Regional WoundCare ProgramFor more information visit: swrwoundcareprogram.ca73
1.2.3.4.5.6.7.8.9.10.11.12.13.14.15.16.Sussman C, Bates-Jensen B. Wound care: A collaborative practice manual for health professionals.USA:Lippincott Williams & Wilkins;2007.VanRijswijk L, Polansky M. Predictors of time to healing deep pressure ulcers. Ostomy Wound Management.October 1994;40(8):40-42, 44, 46-48.Bergstrom N, Allman RM, Alvarez OM, et al. Clinical practice guideline: Treatment of pressure ulcers. RockvilleMD: US Department of Health and Human Services Public Health Service Agency for Health Care Policy andResearch; 1994. 15.www.npuap.orgThomas DR, Rodeheaver GT, Bartolucci AA, et al. Pressure Ulcer Scale for Healing: Derivation and validation of thePUSH tool. Adv Wound Care. 1997;10(5):96-101.Gardner SE, Frantz RA, Bergouist S, Shin CD. A prospective study of the pressure ulcer scale for healing (PUSH). Jof Gerontology. 2005;60A(1):93-97.Stotts NA, Thomas DR, Frantz RA, et al. An instrument to measure healing in pressure ulcers: Development andvalidation of the pressure ulcer scale for healing (PUSH). J Gerontol Series A. 2001;56(12):M795-799.Lee S, Kwon PME, Dorner B, et al. Pressure ulcer healing with a concentrated, fortified collagen proteinhydrolysate supplement: A randomized controlled trial. Advances in Skin and Wound Care. 2006;19(2):92-96.Bates-Jensen BM, Vredevoe D, Brecht ML. Validity and reliability of the pressure sore status tool. Decubitus.1992;5(6):20-28.Bolton L, McNees P, Van Rijswijk L, et al. Wound healing outcomes using standardized assessment and care inclinical practices. J Wound Ostomy Continence Nursing. 2004;31(2):65-71.Ferrell BA, Artinian BM, Sessing D. The sessing scale for assessment of pressure ulcer healing. J Am Geriatr Soc.1995;43(1):37–40.Ferrell BA, Keeler E, Siu AL, Ahn S-H, Osterweil D. Cost-effectiveness of low-air-loss beds for treatment of pressureulcers. J Gerontol A Biol Sci Med Sci. 1995;50A(3):M141–M146.Ferrell BA. The Sessing Scale for measurement of pressure ulcer healing. Adv Wound Care. 1997;10(5):78-80.Houghton PE, Kincaid CB, Campbell KE, et al. Photographic assessment of the appearance of chronic pressure andleg ulcers. Ostomy Wound Management. 2000;46(4):20-30.Houghton PE, Kincaid CB, Lovell M, et al. Effect of Electrical Stimulation on Chronic Leg Ulcer Size and Appearance.Physical Therapy. 2003;83(1):17-28.Thawer HA, Houghton PE, Woodbury MG, et al. A Comparison of Computer-assisted and Manual Wound SizeMeasurement. Ostomy Wound Management . 2002;48(10):46-53.South West Regional WoundCare ProgramReferences74
.Woodbury MG, Houghton PE, Keast DH, Campbell KE. Development, Validity, Reliability and Responsiveness of a New LegUlcer Measurement Tool. Advances in Skin & Wound Care 2004;17:187-196.Woodbury MG, Houghton PE, Campbell KE, Keast DH. Leg ulcer measurement tool (LUMT): more about its ability to detectchange. Ostomy Wound Management . 2004;50(10):78.Nachbar F SW, Merkle T, Cognetta AB, et al. The ABCD rule of dermatoscopy, High prospective value in the diagnosis ofdoubtful melanocytic skin lesions. J Am Acad Dermatol. Apr 1994;30(4):551-559.Throne N. The problem of black skin. Nursing Times; 1969”999-1001.Weiss EL. Connective tissue in wound healing. McCulloch J KL, Feedar J, ed. Wound Healing Alternatives in Management.Second ed. Philadelphia: FA Davis; 1995:26-28.Makelbust J, Sieggreen M. Etiology and pathophysiology of pressure ulcers. In: Makelbust J SM, ed. Makelbust J,Sieggreen M. First ed. West Dundee, IL:S.N. Publications; 1991:19-27.Dorland. Dorland’s Illustrated Medical Dictionary. W.B. Saunders (Harcourt Health Services) [electronic]. Available at:http://www.mercksource.com/pp/us/cns/cns hl dorlands. Accessed September 19, 2005.Keast DH, Bowering CK, Evans AW, et al. MEASURE: A proposed assessment framework for developing best practicerecommendations for wound assessment. Wound Rep Reg. 2004;12:S1-S17.Kantor J, Margolis DJ. A multicenter study of percentage change in venous leg ulcer area as a prognostic index of healing at24 weeks. Br J Dermatol. 2000;142:960-964.Snyder RJ, Cardinal M, Dauphinee DM, et al. A post-hoc analysis of reduction in diabetic foot ulcer size at 4 weeks as apredictor of healing by 12 weeks. Ostomy Wound Management. 2010;56(3):44-50.Bolton L. Chronic wounds and delayed healing risk. Wounds. 2010;22(6):8-12.Flanagan M. Improving accuracy of wound measurement in clinical practice. Ostomy/Wound Management.2003;49(10):28-40.Van Rijswijk L. Full-thickness pressure ulcers: Patient and wound healing characteristics. Decubitus. 1993;6:16-21.Gunes UY. A prospective study evaluating the pressure ulcer scale for healing to assess stage II, stage III, and stage IVpressure ulcers.Ramirez AT, Soroff HS, Schwartz MS, et al. Experimental wound healing in man. Surg Gynecol Obstet. Feb.1969;128(2):283-293.Hon J, Lagden K, McLaren AM, et al. A prospective multicenter study to validate use of the PUSH in patients with diabetic,venous, and pressure ulcers. Ostomy Wound Management. 2010;56(2):26-36.Krasner D. Wound care: how to use the red-yellow-black system. Am J Nurs. 1995:95(5):44–47.South West Regional WoundCare ProgramReferences Continued75
Developed by wound care clinicians and researchers by extracting the Pressure Sore Status Tool subscales that could be evaluated from photographs Consists of 6 items: edges, necrotic tissue type, necrotic tissue amount, skin color surrounding wound,