Transcription
Diagnostic UltrasoundMusculoskeletal
ii
Diagnostic UltrasoundMusculoskeletalJames F. GriffithMD, MRCP, FRCRProfessor of Imaging and Interventional RadiologyDepartment of Imaging and Interventional RadiologyThe Chinese University of Hong KongHong Kong (SAR), Chinaiii
ELSEVIER1600 John F. Kennedy Blvd.Ste 1800Philadelphia, PA 19103-2899DIAGNOSTIC ULTRASOUND: MUSCULOSKELETALISBN: 978-1-937242-17-6Copyright 2015 by Elsevier. All rights reserved.No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, includingphotocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Detailson how to seek permission, further information about the Publisher's permissions policies and our arrangements with organizationssuch as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may benoted herein).NoticesKnowledge and best practice in this field are constantly changing. As new research andexperience broaden our understanding, changes in research methods, professional practices,or medical treatment may become necessary.Practitioners and researchers must always rely on their own experience and knowledge inevaluating and using any information, methods, compounds, or experiments describedherein. In using such information or methods they should be mindful of their own safetyand the safety of others, including parties for whom they have a professional responsibility.With respect to any drug or pharmaceutical products identified, readers are advised to checkthe most current information provided (i) on procedures featured or (ii) by the manufacturerof each product to be administered, to verify the recommended dose or formula, themethod and duration of administration, and contraindications. It is the responsibility ofpractitioners, relying on their own experience and knowledge of their patients, to makediagnoses, to determine dosages and the best treatment for each individual patient, and totake all appropriate safety precautions.To the fullest extent of the law, neither the Publisher nor the authors, contributors, oreditors, assume any liability for any injury and/or damage to persons or property as a matterof products liability, negligence or otherwise, or from any use or operation of any methods,products, instructions, or ideas contained in the material herein.Publisher Cataloging-in-Publication DataDiagnostic ultrasound : musculoskeletal I [edited by] James F. Griffith.pages; cmMusculoskeletalIncludes bibliographical references and index.ISBN 978-1-937242-17-6 (hardback)1. Musculoskeletal system--Ultrasonic imaging. 2. Diagnostic ultrasonic imaging.I. Griffith, James F. II. Title: Musculoskeletal.[DNLM: 1. Musculoskeletal Diseases--ultrasonography--Atlases.2. Extremities--ultrasonography--Atlases. WE 141]RC925.7.D515 2014616.7075--dc23International Standard Book Number: 978-1-937242-17-6Cover Designer: Tom M. Olson, BACover Art: Lane R. Bennion, MSPrinted in Canada by F riesens, Altona, Manitoba, CanadaLast digit is the print number: 9 8 7 6 5 4 3 2 1ivELSEVIER Book AidInternationalWorking togetherto grow libraries indeveloping countrieswww.elsevier.com www.bookaid.org
Diagnostic UltrasoundMusculoskeletal
SECTION 1Upper LimbSternoclavicular and Acromioclavicular Joints.1-1-2Shoulder.1-1-8Axilla . 1-1-26Arm . 1-1-34Arm Vessels. 1-1-42Elbow . 1-1-50Forearm . 1-1-70Forearm Vessels . 1-1-78Wrist . 1-1-86Hand .1-1-100Hand Vessels1-1-112Thumb .1-1-118Fingers .1-1-128Radial Nerve1-1-140Median Nerve.1-1-148Ulnar Nerve .1-1-158
STERNOCLAVICULAR AND ACROMIOCLAVICULAR JOINTS.cE:.:::iTE RMINOLOGYI.Q)Cl.Cl.Superior AC ligament Sternoclavicular (SC) joint -Acromioclavicular (AC) joint0rac: C0Abbreviations::JELigaments of AC joint GROSS ANATOMY 0Synovial sellar-type (saddle) joint0Medial end of clavicle large and bulbous00Conoid ligament located posteromediallyMuch larger than manubrial concavity Mainly prevents upward movement of clavicle Trapezoid ligament located anterolaterally Attached to joint capsule anteriorly and posteriorly Complete or incomplete perforationsThickest posterosuperiorly (3 mm)Ligaments of sternoclavicular jointCapsular ligaments 0Muscle attachments to lateral clavicle Cover anterosuperior and posterior aspects of Interclavicular ligament Connects superomedial aspect of clavicle tocapsular ligaments and upper manubrium Covers anterosuperior and posterior aspects of joint Prevents excessive upward motion of clavicleCostoclavicular ligaments ANATOMY IMAGING ISSUESImaging RecommendationsHigh-resolution linear transducerAlign transducer transversely along SC or AC jointsAC joint laxity can be assessed by pulling down on armwhile observing change in joint width on ultrasound Compare with contralateral sideUnite inferior surface medial end clavicle to upperMain clinical presentation of SC joint is painless lumpsurface of 1st rib0Mild degrees of capsular thickening readily apparentclinically since joint just beneath skin surfaceAnterior fibers arise from anteromedial surface of1st rib and resist upward motion Trapezius attached to posterior surface lateral 1/3 ofclavicleshoulder0Deltoid attached to anterior surface lateral 1/3 ofclaviclePrevent upward displacement of medial clavicle,Anterior stronger than posterior portionMainly prevents lateral compression of clavicleagainst acromionwhich may be caused by downward force on Inserts to trapezoid ridge, which runs alonginferior surface, of lateral 1/3 of claviclesternoclavicular joint Inserts to conoid tubercle which is located whereclavicleStability through capsuloligamentous structures0 Vary significantly in length and width middle 1/3 of clavicle curves into lateral 1/3 ofIntraarticular disc0Conoid and trapezoid ligaments 1/2 of medial clavicle articulates with manubrium Clinical swelling often due to relative forwardpositioning of apparently swollen SC joint due toPosterior fibers arise lateral to anterior fibers andaxial rotation of upper trunkresist downward motionMuscle attachments to medial clavicle and sternum Occasionally due to mild capsular swelling mildsubluxation secondary to SC osteoarthritis0Pectoralis major from anterior aspect medial 2/30Sternocleidomastoid from posterior surface medialosteoarthritis, AC joint impingement, inflammatory1/3 of clavicle (clavicular head)arthropathy, and subluxation/dislocationclavicle (clavicular head)0Sternohyoid and sternothyroid muscles separate greatvessels from sternoclavicular jointAcromioclavicular Joint0SC or AC joints0Normally a step-off between medial clavicle andmanubrium and, to lesser degree, between lateralclavicle and acromionmedial end of acromion0Main clinical presentation of AC joint is pain due toImaging PitfallsSynovial joint between lateral end of clavicle andArticular surface of clavicle oriented posterolaterally0Should not be interpreted as subluxationwhereas articular surface of acromion oriented0Acromion normally elevates from rest position0AC joint index AC joint width of uninjured side/ACduring arm adductionanteromedially Angle of inclination between opposing articularjoint width of injured side 1.0 normallysurfaces varies with clavicle overriding acromion(50%), vertical orientation between acromion andclavicle (25%), clavicle underriding acromion (5%),0Determine whether AC joint not subluxed (similar to opposite side) : AC joint partially subluxed (clavicle subluxed AC joint severely subluxed or dislocated (clavicleGrade 1and mixed pattern (20%) Maximum width of normal joint on ultrasound 550% depth of AC joint) : Grade 2mm if 35 years and 4.4 mm if 35 years 2(8 mm) and medialCoracoclavicular ligaments Sternoclavicular JointBetween medial end of clavicle and manubrium1Inserts along lateral clavicleacromion (10 mm)-IStronger and thicker (2.0-5.5 mm) than thin orabsent inferior AC ligamentMaximum thickness of capsule from bony surface 2.7 mm if 35 years and 3.6 mm if 35 yearsIntraarticular disc0Undergoes rapid degeneration beginning in 2nddecade- marked degeneration of disc by 4th decadesubluxed 50% depth of AC joint) : Grade 3
STERNOCLAVICULAR AND ACROMIOCLAVICULAR JOINTSTRANSVERSE US, STERNOCLAVICULAR JOINTInterclavicular ligament1st ribAnterior sternoclavicular ligament -----" ---- -ClavicleArticular disc1st costal cartilageCostoclavicular ligamentManubrium sternumSternoclavicular jointManubrium, sternumInterclavicular ligamentMedial end of clavicleJoint capsuleInterclavicular ligamentManubrium, sternum(Top) Graphic shows the anterior aspect of the sternoclavicular joint. Note the joint capsule, articular disc, and interclavicular ligament.(Middle) Transverse grayscale ultrasound shows the anterosuperior aspect of the sternoclavicular joint. The medial clavicle is much largerthan the articulating surface of the manubrium. The thin interclavicular ligament is closely applied to the superior aspect of manubrium, andits connection with the medial ends of both clavicles is depicted. (Bottom) Transverse grayscale ultrasound shows the superior aspect of thesternoclavicular joint. The costoclavicular ligament prevents upward movement of the medial clavicle when the lateral clavicle or shoulder isdepressed.I13
STERNOCLAVICULAR AND ACROMIOCLAVICULAR JOINTS.cE:.:::iLONGITUDINAL US, STERNOCLAVICULAR JOINTI.Q)Cl.Cl.::J -E0rac: C-Pectoralis major muscleCostoclavicular ligamentMedial end of clavicle1st ribSternocleidomastoid muscle, sternalendSternumSternocleidomastoid muscle, sternalinsertionSubclavian arterySternocleidomastoid, clavicularinsertionMedial end of clavicleSternocleidomastoid muscleSubclavian veinSubclavian artery(Top) Longitudinal grayscale US shows sternoclavicular joint. Costoclavicular ligament prevents upward movement of the medial clavicle whenshoulder is depressed. Pectoralis major muscle arises from the medial 712 of the anterior surface of the clavicle as well as from the sternum,upper costal cartilages, and upper part of external oblique aponeurosis. (Middle) Longitudinal grayscale US shows sternoclavicular joint region.I14Sternocleidomastoid is attached to the upper surface of the medial end of the clavicle as well as the upper anterior surface of the manubrium.Sternohyoid and sternothyroid are attached to the posterior aspect of the sternum as well as the clavicle and 7 st costal cartilage. (Bottom)Longitudinal grayscale US shows sternoclavicular joint. Great vessels lie posterior to sternoclavicular joint and may get injured in posteriordislocation. All tendinous attachments should be assessed if dislocation is present as they may also be injured.
STERNOCLAVICULAR AND ACROMIOCLAVICULAR JOINTSUS, ACROMIOCLAVICULAR JOINTSuperior acromioclavicular ligamentInferior acromioclavicular ligamentCoracoacromial ligamentCoracoclavicular ligament, trapezoidcomponentCoracohumeral ligamentClavicle, distalCoracoclavicular ligament, conoidbandCoracoid processTransverse humeral ligamentBiceps tendon, long headSubscapularis muscleBiceps tendon, short headLatissimus dorsi muscleTeres major muscleLateral end of clavicleCoracoclavicular ligament, trapezoidcomponentCoracoid processDeltoid muscleCoracoacromial ligamentCoracoid processAcromionSupraspinatus muscleHumeral head(Top) Anterior graphic shows the shoulder in superficial dissection. (Middle) Longitudinal grayscale ultrasound shows the acromioclavicular jointregion. The coracoclavicular ligament is demonstrated but is not as clearly depicted on US as it is on MR exam. These ligaments prevent upwardand lateral movement of the clavicle. (Bottom) Transverse grayscale ultrasound of the acromioclavicular joint region shows the coracoacromialligament. The supraspinatus tendon and intervening bursa can impinge against the coracoacromial ligament during arm abduction.I15
STERNOCLAVICULAR AND ACROMIOCLAVICULAR JOINTS.cE:.:::iTRANSVERSE US, ACROMIOCLAVICULAR JOINTI.Q)Cl.Cl.::J -E0rac: CSuperior acromioclavicular ligament-ClavicleAcromionAnterior capsuleSuperior acromioclavicular ligamentClavicleJoint capsuleAcromionSuperior acromioclavicular ligamentClavicleJoint capsuleAcromion(Top) Transverse grayscale ultrasound shows the anterior aspect of the acromioclavicular joint. The joint capsule of the acromioclavicularjoint is thin with a strong supporting superior acromioclavicular ligament. (Middle) Transverse grayscale ultrasound shows the anterosuperioracromioclavicular joint. Separation of the clavicle and acromion can be readily appreciated. Note how opposing bone margins are not verticallyI16aligned. (Bottom) Transverse grayscale ultrasound shows the superior aspect of the acromioclavicular joint. In this image, the clavicle slightlyoverrides the acromion. This is a normal configuration.
STERNOCLAVICULAR AND ACROMIOCLAVICULAR JOINTSTRANSVERSE US, ACROMIOCLAVICULAR JOINTJoint capsuleClavicleSuperior acromioclavicular ligamentJoint capsuleAcromionClavicleJoint capsuleAcromionClavicle(Top) Transverse grayscale ultrasound shows the anterosuperior aspect of the acromioclavicular joint with the arm positioned by the side of thebody. Note that the clavicle slightly overrides the acromion. (Middle) Transverse grayscale ultrasound shows the acromioclavicular joint with thearm in abducted position. The acromion is now level with the lateral aspect of the clavicle. Note how the joint capsule bulges superiorly and theopposing bones are approximated with the arm abducted. (Bottom) Transverse grayscale ultrasound shows the acromioclavicular joint with thearm in an adducted position. The acromion is now depressed relative to this lateral end of the clavicle.I17
SHOULDER.cE:.:::iQ)Cl.Cl.::J -E0rac: C- However, insertional area is more prone to tearingIMAGING ANATOMYI.than critical zoneOverviewBiceps tendon, long head0 Origin: Superior glenoid labrum (biceps anchor)Rotator cuff Portions may attach to supraglenoid tubercle,Consists of supraspinatus, infraspinatus, teres minor,anterosuperior labrum, posterosuperior labrum,subscapularis muscles, and tendons and coracoid baseCuff tendons blend with shoulder joint capsule0 Supraspinatus and infraspinatus tendons are0 Runs along superior aspect shoulder to bicipitalgrooveinseparable at insertion0 Anterior 2.25 cm of tendon comprises supraspinatustendon insertional area0 Action: Stabilizes and depresses humeral head0 Anatomic variants: Anomalous intra- & extraarticularorigins from rotator cuff and joint capsuleSupraspinatus muscle0 Tendon sheath communicates with glenohumeral0 Origin: Supraspinatus fossa of scapulajoint and normally contains small amount of fluid0 Insertion: Superior facet (horizontal orientation) andanterior portion of middle facet of greater tuberositySubacromial-subdeltoid fat plane Broad insertional area0 Subacromial and subdeltoid portions subcoracoid extension in some patients0 Nerve supply: Suprascapular nerve0 Blood supply: Suprascapular artery and circumflexFat plane is superficial to bursa0 May be interrupted or absent in normal patientsscapular branches of subscapular artery0 Attached along free border of coracoacromial0 Action: Abduction of humerus0 Muscle consists of 2 distinct portionsligament and adjacent deep surface of deltoid muscle,and humeral neck region Anterior portion is larger, fusiform in shape, hasdominant tendon, and is more likely to tear Posterior portion is flat and has terminal tendonRotator cuff interval0 Space between supraspinatus and subscapularistendon through which biceps tendon passes0 Most commonly injured rotator cuff tendon0 Borders of rotator cuff intervalInfraspinatus muscle0 Origin: Infraspinatus fossa of scapula Triangular-shaped space0 Insertion: Mid to posterior aspects of middle facet of Reflections of glenohumeral ligament andgreater tuberositycoracohumeral ligament form biceps reflection Centrally positioned within tendonpulley Biceps reflection pulley stabilizes biceps tendon0 Nerve supply: Suprascapular nerve, distal fiberswithin rotator cuff interval0 Blood supply: Suprascapular artery and circumflex Superior border: Leading edge of supraspinatusscapular branches of subscapular artery Inferior border: Superior aspect subscapularis0 Action: External rotation of humerus and resiststendonposterior subluxation Lateral border: Long head of biceps tendon andTeres minor muscle0 Origin: Lateral scapular border, middle1/2bicipital groove Medial border: Base of coracoid process0 Insertion: Inferior facet (vertical orientation) ofgreater tuberosity Biceps reflection pulley0 Blood supply: Posterior circumflex humeral artery &circumflex scapular branches of subscapular artery0 Action: External rotation of humerus0 Least commonly injured rotator cuff tendonContents of rotator interval Long head of biceps tendon0 Nerve supply: Axillary nerveCoracoacromial ligament Forms coracoacromial arch along with acromion andcoracoid process Reinforces inferior aspect of acromioclavicular jointSubscapularis muscle0 Origin: Subscapular fossa of scapula0 Extends from distal coracoid to subacromial area0 Insertion: Lesser tuberosity and up to 40% may insert0 Broad insertion to undersurface acromion Ligament is thicker at acromion (normal thicknessat surgical neck0 Also some fibers cross over to lateral lip of bicipital 2.5 mm)Glenoid labrumtransverse ligament0 Triangular-shaped rim of fibrocartilage, which0 Nerve supply: Subscapular nerve, upper and lowerextends around periphery of glenoid0 Blood supply: Subscapularis arteryANATOMY IMAGING ISSUES0 Action: Internal rotation of humerus, also adduction,extension, depression, and flexion0 4-6 tendon slips converge into main tendon;multipennate morphology increases strengthRotator cuff tendon blood supply0 Derived from adjacent muscle, bone, and bursae0 Normal hypovascular regions in tendonsI18and may be associated with spursgroove reinforcing and blending with fibers of Termed "critical zone"-1 cm proximal to insertion This area is vulnerable to degeneration and calcificdepositionImaging ApproachesTendons best seen when on stretch0 High-resolution linear transducer0 Long-axis (longitudinal) and transverse view of eachtendon0 Each part of tendon needs to be examined;anisotropy prevents all parts of curved rotator cufftendons being seen at same time0 Need to realign ("toggle") probe to see different partsof tendons
SHOULDERSupraspinatus tendonTendon edges0 Arm extended and internally rotated behind lumbar0 Interfaces of tendons with adjacent structures maysimulate tearsregion (Crass position) Or, if too painful, hand in posterior hip region("back pocket") with elbow close to body (modifiedCrass position)Infraspinatus and teres minor tendons0 All tears and other tendon pathology should beconfirmed in 2 planesRotator cuff cable0 Thick band of fibers running perpendicular to0 Arm flexed and internally rotated with hand placedon contralateral shouldersupraspinatus tendon0 Located on deeper aspect of tendon just proximal to0 Teres minor tendon located posteroinferior toinfraspinatus tendonSubscapularis tendoninsertional area0 May reinforce 'critical zone' supraspinatus fibers 0 Arm neutral and externally rotatedLong head of biceps tendonCable thicker in young subjects but more easily seenin elderly subjects due to supraspinatus tendinosis Can simulate tendinosis or partial thickness tear0 Arm neutral and externally rotatedTendinous interspace at rotator cuff interval0 Vary degree of external rotation for optimal view of0 Interspace between leading edge (anterior edge) of biceps tendonsupraspinatus and long head of biceps tendon mayCheck for tendon subluxationsimulate tearSubacromial-subdeltoid bursa0 Overcome by recognizing ovoid or rounded shape of0 Stretching tendons may squeeze fluid from area ofbursa under inspectionbiceps tendon0 Rotator cuff inter val best seen with arm in external0 Examine in all positions and also in neutral position rotationacromion, lateral to proximal humerus, and nearFocal thinning at supraspinatus-infraspinatusjunctioncoracoacromial ligament0 Mild diffuse thinning of supraspinatus andFluid collects preferentially just lateral toinfraspinatus tendon junction is normal findingCoracoid process and coracoacromial ligament0 Neutral positionAcromioclavicular joint0 Neutral position Can pull down on arm when examining0 Should not be mistaken for tendon attenuation orpartial thickness tearMusculotendinous junction0 Supraspinatus tendonacromioclavicular joint to assess joint laxity 0 Neutral positionsubdeltoid bursal distension0 Best seen from posterior aspect of joint 0 Passive movement of arm during scanning can helpin identifying posterior glenoid labrum0 Infraspinatus tendon 0 Neutral position just medial to glenohumeral jointcoronal and sagittal planes)0 t muscle bulk, t muscle echogenicity and reduced0 Subscapularis tendon Fibrocartilaginous insertion0 Thin layer of fibrocartilage exists between tendon andbone at insertional areaImaging Sweet SpotsLook for tears particularly at anterior leading edge ofsupraspinatus tendon0 Unexplained bursal fluid is a good secondary sign ofrotator cuff tearBursal fluid is often best seen with arm in neutralposition or t internal rotation (hand in back pocket)Imaging PitfallsAnisotropy0 Echoes are optimally reflected when transducer isparallel to tendon fibers0 Rotator cuff tendons are prone to anisotropy due tocurved course0 If transducer is not at right angles to tendon, it willappear either isoechoic or hypoechoic to muscle 0 The steeper the tendon insertion, the thicker thefibrocartilaginous layerCompare muscle echogenicity to that of trapeziusor deltoid muscleMay simulate tendinosis or partial tear4-6 tendon slips converging into main tendon maysimulate tendinosisvisibility of central tendon are signs of muscleatrophy with fatty replacementMuscle fibers surrounding centrally positionedtendon may be confused with tear0 Neutral position with hands resting on thigh0 Examine thickest part of muscles from behind (inInterdigitating tendons of anterior and posteriorportions may simulate tendinosis or tearSpinoglenoid notchSupraspinatus and infraspinatus musclesHypoechoic muscle extending along superficialaspect of tendon may simulate subacromial Glenohumeral joint0 This thin hypoechoic layer of fibrocartilage maysimulate avulsive tearSubacromial-subdeltoid fat plane Fat plane lies mainly superficial to bursa and deep todeltoid muscle0 Normal bursa is very thin0 Thickness of echogenic fat plane is variable amongpatients though usually similar from side to side0 May be wrongly interpreted as bursal fluid Look for intrabursal fluid hyperemia (latter is afeature of inflammatory arthropathy)Fluid in biceps tendon sheath Communicates with glenohumeral joint0 Small amount of fluid is normal Do not misinterpret as long head of bicepstenosynovitis0 t fluid in biceps tendon sheath usually reflects t fluidin glenohumeral jointI19
.cE:.:::iI.Q)Cl.Cl.::J -E0rac: C-I110
I111
.cE:.:::iI.Q)Cl.Cl.::J -E0rac: C-I112
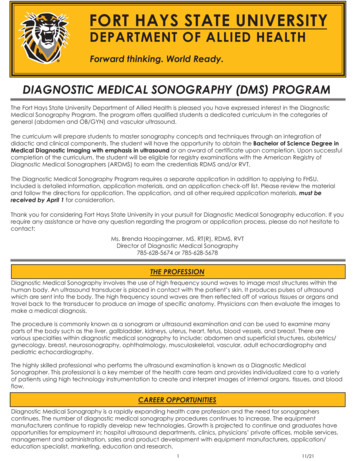
SHOULDERLONGITUDINAL US, SUPRASPINATUS INSERTIONAL AREADeltoid muscleGreater tuberositySubdeltoid peribursal fatInser tional areaSupraspinatus tendonArticu lar cartilageHumeral headDeltoid muscleGreater tuberositySubdeltoid peribursal fatSupraspinatus tendonArticu lar cartilageHumeral headDeltoid muscleSharpey fibers at insertional siteGreater tuberositySubdeltoid peribursal fatSupraspinatus tendonHumeral head(Top) Longitudinal grayscale ultrasound shows the anterior fibers of the supraspinatus tendon insertional area. The supraspinatus tendon insertsover a wide area (footprint) on the anterior aspect of the greater tuberosity. Many tears of the supraspinatus tendon involve avulsion of thetendon from its insertional site. (Middle) Longitudinal grayscale ultrasound shows the supraspinatus tendon midfibers. There is often a thinhypoechoic line at the insertional area. This represents Sharpey fibers and fibrocartilage. (Bottom) Longitudinal grayscale ultrasound shows thesupraspinatus tendon posterior fibers. The anterior, middle, and posterior fibers should be evaluated in turn.I113
SHOULDER.cE:.:::iTRANSVERSE US, SUPRASPINATUS INSERTIONAL AREAI.Q)Cl.Cl.::J -E0rac: C-Deltoid muscleGreater tuberositySubdeltoid peribursal fatInsertional area, lateral fibersSupraspinatus tendonHumeral headDeltoid muscleGreater tuberosityInsertional area, middle fibersSubdeltoid peribursal fatSupraspinatus tendonHumeral headDeltoid muscleGreater tuberosityInsertional area, medial fibersSupraspinatus tendonHumeral head(Top) Transverse grayscale ultrasound shows the supraspinatus tendon insertional area. Angulation and slight movement of the transducerwill allow visualization of the lateral, middle, and medial fibers, respectively. The leading anterior edge of the supraspinatus is a commonsite of tear (rim rent tear). (Middle) Transverse grayscale ultrasound shows the supraspinatus tendon at the insertional area of midfibers. TheI114fibrillar echotexture of the supraspinatus tendon can be seen but is prone to anisotropy. (Bottom) Transverse grayscale ultrasound shows thesupraspinatus midfibers insertional area. Subdeltoid peribursal fat is variable in depth. The normal bursa cannot be depicted. It is seen only whendistended with fluid or thickened due to synovitis.
SHOULDERTRANSVERSE AND LONGITUDINAL US, SUPRASPINATUSSubdeltoid peribursal fatSupraspinatus tendon ,s "' - ;:"" Insertional areaHumeral headJ l!!l !::::: liil.i;.-;AcromionDeltoid muscleSubdeltoid peribursal fatSupraspinatus tendonArticular cartilageHumeral headDeltoid muscleSubdeltoid peribursal fatSupraspinatus tendonHumeral headMusculotendinous junctionArticular cartilageGlenoid(Top) Transverse grayscale ultrasound shows the supraspinatus tendon just medial to the insertional area. The critical zone is located just medialto the insertional area. This is a relatively hypovascular area. It is prone to calcific tendinosis and tears, though most tears tend to occur atthe insertional site. (Middle) Transverse grayscale ultrasound shows the supraspinatus medial to the insertional area. The fibrillar pattern ofthe supraspinatus tendon is prone to anisotropy With tendinosis, the fibrillar pattern is disrupted. The tendon becomes more hypoechoicand thickened. (Bottom) Longitudinal grayscale ultrasound shows the supraspinatus tendon at a slightly more medial aspect. Tears of themusculotendinous junction are relatively uncommon.I115
.cE:.:::iI.Q)Cl.Cl.::J -E0rac: C-I116
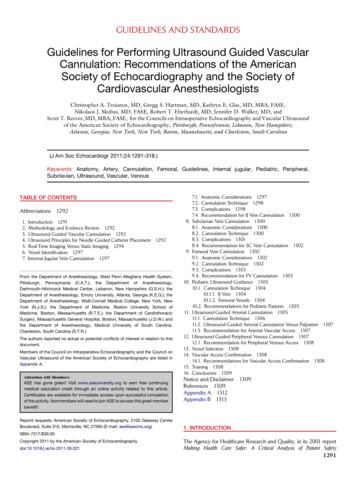
SHOULDERTRANSVERSE US, BICEPS TENDONDeltoid muscleBiceps tendonSubdeltoid peribursal fatHumeral headUpper end ofbicipital grooveDeltoid muscleTransverse ligamentSubscapularis tendonBiceps tendonBicipital grooveHumeral headMedial lip ofbicipital grooveDeltoid muscleTransverse ligamentLateral lip ofbicipital grooveBiceps tendonSubscapularis muscleHumeral headMedial lip ofbicipital groove(Top) Transverse grayscale ultrasound at the proximal aspect of the biceps tendon: The bicipital groove forms a fibroosseous tunnel for the bicepstendon. The normal biceps tendon has an ovoid configuration. With tendinosis, the tendon becomes larger and more rounded in appearance.(Middle) Transverse grayscale US shows the biceps tendon. The biceps tendon is held in position by the transverse ligament. The subscapularistendon inserts into the lesser tuberosity. which forms the medial lip of the bicipital groove. The biceps tendon may sublux medially from thegroove and may be associated with subscapularis tendon injury. (Bottom) Transverse grayscale US shows relations of the biceps tendon. Thetransverse ligament is not a distinct entity but consists of a fibrous expansion of both the pectoralis major tendon and subscapularis tendoninserting into the lateral lip of the bicipital groove.I117
SHOULDER.cE:.:::iLONGITUDINAL US, BICEPS TENDONI.Q)Cl.Cl.::J -E0rac: C-Subcutaneous fatDeltoid muscleBiceps tendon entering shoulder jointHumeral headSubcutaneous fatDeltoid muscleBiceps tendonHumeral headSubcutaneous fatDeltoid muscleBiceps tendonHumeral shaft(Top) Longitudinal grayscale ultrasound shows the uppermost section of the biceps tendon. The intraarticular portion of the biceps long headtendon cannot be fully depicted on longitudinal imaging. On longitudinal section, the biceps tendon seems to expand at its upper end as itbecomes more ovoid in contour. This location is also the most common site of biceps tendinosis, which also manifests as enlargement of theI118biceps tendon. (Middle) Longitudinal grayscale ultrasound shows the upper section of the biceps tendon. A small amount of fluid in the bicepstendon sheath, which is continuous with the glenohumeral joint, is normal and should not be mistaken for tenosynovitis. No fluid is depicted inthis image. (Bottom) Longitudinal grayscale ultrasound shows the lower aspect of the biceps tendon. Most incomplete tears of the biceps tendonsare longitudinal in orientation and are best depicted on transverse imaging.
SHOULDERLONGITUDINAL, SUBSCAPULARISDeltoid muscleSubscapularis tendonBiceps tendonBicipital groove, lateral lipBicipital groove, medial lipDeltoid muscleSubscapularis tendonDeltoid muscleSubscapularis tendonCoracoid processHumeral head(Top) Longitudinal grayscale ultrasound shows the subscapularis insertion. The subscapularis inserts into the medial lip of the bicipital groove buthas a fibrous expansion traversing the biceps tendon, through which it also gains attachment to the lateral lip of the bicipital groove. (Middle)Longitudinal grayscale ultrasound shows the subscapularis insertional area. Complete tears of the subscapularis are uncommon and usuallyfollow a severe traumatic event. Partial tears are more common and usually involve the superior edge o
Diagnostic Ultrasound Musculoskeletal James F. Griffith MD, MRCP, FRCR Professor of Imaging and Interventional Radiology Department of Imaging and Interventional Radiology The Chine