Transcription
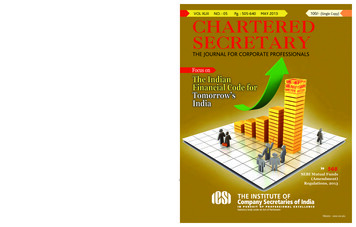
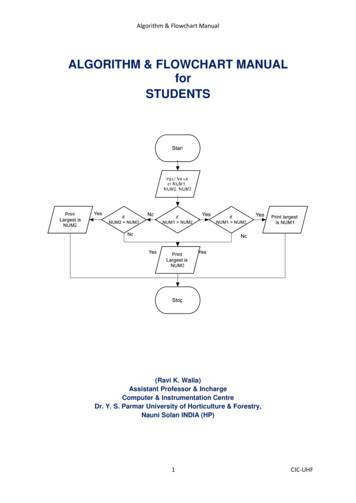
Health Care Guideline:Adult Acute and Subacute Low Back PainDiagnosis AlgorithmSixteenth EditionMarch 2018Text in blue in this algorithmindicates a linked correspondingannotation.Red Flags forUnderlyingPathology Cauda equinasymptoms Cancer risk Spinal infection risk Fragility fracturerisk Unrelenting pain Progressiveneurologic deficit TraumaYellow Flags(Psychosocial Factors) Work place Attitudes and beliefs Sociał/family Behaviors Affective/emotionsAdult patient presentwith acute or subacutelow back painComplete assessment toolsfor pain and functionHistory and exam: Pain characteristics Sensory and strength changes Prior treatment and responseIncapacitating painand/or advancingneurologic symptoms or otherunderlyingpathologyyesConsider reevaluation, imagingor referral tospecialistnoAddress modifiablepsychosocial factorsRoutine imaging is notrecommendedSee TreatmentAlgorithmAcute 4 weeksSubacute 4-12 weeksChronic 12 weekswww.icsi.orgCopyright 2017 by Institute for Clinical Systems Improvement1
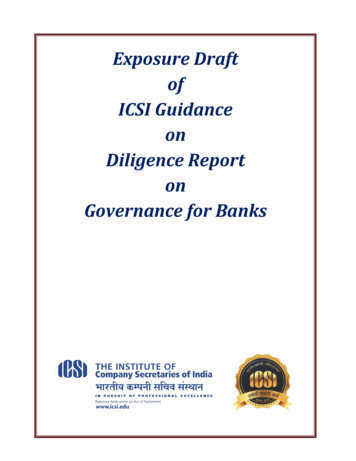
Adult Acute and Subacute Low Back PainSixteenth Edition/March 2018Yellow Flags(Psychosocial Factors) Work place Attitudes and beliefs Social /family Behaviors Affective/emotionsTreatment AlgorithmAcute or subacutelow back paindiagnosisRoutine imaging is notrecommendedEstablish treatment goals using shareddecision-making: Patient goals Clinical goals Patient barriers Psychosocial factorsDevelop a Treatment PlanPatient plement a jointly agreed upon care plan: Patient education and training Self-management plan Reassessment plan Return to work plan2-3 week follow upGoals met? Function PainnonoyesContinued selfmanagement andeducation to preventfuture episodesInstitute for Clinical Systems ImprovementPersistent orprogressivesymptoms?Is care planimplemented asplanned?yesnoConsider referral forepidural for subacuteradicular painShared DecisionMakingConsider re-evaluation,imaging or referral tospecialist Re-establlish treatement goals Reassess psychosocial factorsyes- Consider alternativediagnosis (return to DiagnosisAlgorithm)- Consider referralwww.icsi.org2
Adult Acute and Subacute Low Back PainSixteenth Edition/March 2018Table of ContentsWork Group LeaderDavid Thorson, MDSports Medicine, EntiraFamily ClinicsWork Group Members3MRobb Campbell, MD, MPHOccupational MedicineCentraCare Health SystemMichael Massey, DOPain MedicineBecky Mueller, DOFamily Medicine/SportsMedicineFairview Health ServicesBecky McCathie, MEd, ATCSpecialtyHeidi Richards, PT, MHAPhysical TherapyOSI Physical TherapySteven PetersonPhysical TherapyPark Nicollet HealthServicesChris Kramer, PT, DPT, OCS,FAAOMPTPhysical TherapyPhysicians' Diagnostics &Rehabilitation ClinicsTodd Ginkel, DCSpine RehabilitationICSIJodie Dvorkin, MD, MPHProject Manager/Health CareConsultantSenka Hadzic, MPHClinical Systems ImprovementFacilitatorAudrey Hansen, BSN, MA,PMPProject Manager/Health CareConsultantAlgorithms and Annotations . 1-25Algorithm – Diagnosis .1Algorithm – Treatment .2Evidence Grading .4Recommendations Table . 5-6ForewordIntroduction .7Scope and Target Population.7Aims .7Related ICSI Scienti ic Documents .7Definition .8Annotations . 9-25Initial Evaluation . 9-15Treatment Plan . 15-22Re-evaluation .23Radicular Pain - Special Considerations . 23-24Quality Improvement Support . 26-31Aims and Measures .27Measurement Speci ications . 28-29Implementation Tools and Resources .30Implementation Tools and Resources Table .31Supporting Evidence. 32-43References . 33-36Appendices . 37-43Appendix A – Patient Handout .37Appendix B – ICSI Shared Decision-Making Model . 38-43Disclosure of Potential Conflicts of Interest . 44-46Acknowledgements .47Document History and Development . 48-49Document History .48ICSI Document Development and Revision Process .49www.icsi.orgInstitute for Clinical Systems Improvement3
Adult Acute and Subacute Low Back PainSixteenth Edition/March 2018Evidence GradingLiterature SearchA consistent and defined process is used for literature search and review for the development and revisionof ICSI guidelines. Literature searches for this guideline were done under the following parameters: Time frame: January 1, 2000 – May 1, 2017. Types of studies searched for: systematic reviews and meta-analysis, randomized controlled trials andobservational studies (case-control, cohort and cross-sectional studies). Population: adults, 18 years of age and over, with acute and subacute low back pain or radiculopathy. All studies were published in English and included humans.In addition to the literature searches, articles were obtained by work group members and ICSI staff. Thosevetted by the work group were included in the guideline when appropriate.Literature search terms used:STarT Back screening tool; Keele stratified care model; imaging for low back pain; imaging for low backradiculopathy; red flags; clinical prediction rule; fear avoidance; modifiable risk factors; cognitive behavioral therapy; mindfulness-based stress reduction therapy; patient education; education; normal activity vs.staying active; activities of daily living; exercise for prevention; exercise for treatment; bed rest; acupuncture;dry needling; heat therapy; cold therapy; healing efficacy of cold therapy; traction; physical therapy/spinalmanipulation therapy/chiropractic care; NSAIDs for treatment; anti-inflammatories; Tylenol for treatment;corticosteroids for treatment; opioids for treatment; tramadol for treatment; muscle relaxants; benzodiazepines; weight loss for treatment to prevent recurrence of low back pain; obesity and acute/subacute low backpain; obesity and chronic low back pain; acceptance and commitment therapy; regenerative medicine/stemcells/platelet-rich plasma/prolotherapy; medial branch blocks; rhizotomy; functional restoration programfor subacute low back pain; cold laser therapy; radiofrequency ablation; low back pain in pregnancy.MethodologyICSI utilizes a modified version of the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology system. GRADE involves systematically evaluating the quality of evidence(high, moderate, low, very low) and developing a strength of recommendation (strong, weak). For moredetailed information on GRADE, please visit http://www.gradeworkinggroup.org/.When there was a paucity of systematic reveiws and randomized controlled trials, the work group could notapply the GRADE methodology. In these cases, the work group used the best available evidence to reachconsensus recommendations. For each consensus recommendation, the releveant resources used to supportthat recommendation are noted.Return to Table of ContentsInstitute for Clinical Systems Improvementwww.icsi.org4
Adult Acute and Subacute Low Back PainSixteenth Edition/March 2018Recommendations TableThe following table is a list of evidence-based recommendations for adult acute and subacute low back pain.Quality ofEvidence(For GRADERecommendations)Strength ofRecommendation(For luationFor patients with acute and subacutelow back pain, a biopsychosocialassessment should be performed.ImagingClinicians should not routinelyrecommend imaging (x-ray,computed tomography [CT],magnetic resonance imaging [MRI]for patients with nonspecific orradicular low back pain with anabsence of red flags on clinicalpresentation.Quality of Evidence:ModerateStrongRecommendationChou 2009(Systematic Reviewand Meta-analysis);Patel, 2016(Guideline)All patients should receiveappropriate education on thetreatment and recovery expectationsfor acute and subacute low back pain.Quality of Evidence:Moderate-HighStrongRecommendationTraeger, 2015(Systematic Reviewand Meta-Analysis)Heat may be used for pain relief foracute and subacute low back pain.Quality of Evidence:ModerateWeakRecommendationColdCold therapy may be used for painrelief.N/A (Consensus Recommendation)Chou, 2016(ComparativeEffectiveness Review)ActivityClinicians should advise patientswith acute and subacute low backpain to stay active and continueactivities of daily living within thelimits permitted by their symptoms.Quality of Evidence:ModerateStrongRecommendationDahm 2010(Systematic Review);McIntosh 2011(Systematic Review)Spinal manipulation should beconsidered in early intervention foracute and subacute low back pain.Quality of reAcupuncture should be consideredfor subacute low back pain.Quality of Evidence:LowWeakRecommendationPaige, 2017(Systematic Reviewand Meta-Analysis);Chou, 2016(ComparativeEffectiveness Review)NSAIDSNon-steroidal anti-inflammatorymedication may be used for shortterm relief in patients with acute andsubacute low back pain. Patientshould be counseled on potential sideeffects.Quality of SpinalManipulationReturn to Table of ContentsInstitute for Clinical Systems ImprovementN/A (Consensus Recommendation)Relevant ResourcesPapageorgiou, 1998(Observational Study);Waddell, 1987(Report); Waddell,1992 (Report)Chou, 2016(ComparativeEffectiveness Review)Chou, 2016(ComparativeEffectiveness Review)Chou, 2016(ComparativeEffectiveness Review)www.icsi.org5
Adult Acute and Subacute Low Back PainSixteenth Edition/March 2018TopicRecommendationQuality of Evidence(For GRADE Recommendations)AcetaminophenAcetaminophen may be used as anoption for pain relief in patients withacute and subacute low back pain.Patients should be counseled onpotential side effects.N/A (Consensus Recommendation)MuscleRelaxantsOpioidsEpidural SteroidInjectionsMuscle relaxants may be used as ashort-term option ( one week) in thetreatment of acute low back pain.Possible side effects should beconsidered.In general, opioids are notrecommended for acute and subacutelow back pain.Epidural steroid injections may beused as an adjunct treatment for acuteand subacute low back pain with aradicular component to assist withpain relief.Return to Table of ContentsInstitute for Clinical Systems ImprovementQuality of Evidence:ModerateWeakRecommendationN/A (Consensus Recommendation)Quality of Evidence:ModerateStrongRecommendationStrength ofRecommendation(For GRADERecommendations)Chou, 2016(ComparativeEffectiveness Review;Saragiotto, 2016(Systematic Review)Chou, 2016(ComparativeEffectiveness Review)Chou, 2016(ComparativeEffectiveness Review)Chou, 2015(TechnologyAssessment);Manchikanti, 2016(Systematic Review)www.icsi.org6
Adult Acute and Subacute Low Back PainSixteenth Edition/March 2018ForewordIntroductionStudies have estimated the one-year incidence of a first-ever episode of low back pain ranges between 6.3%and 15.4%, while estimates of the one-year incidence of any episode of low back pain range between 1.5%and 36% (Hoy, 2010).Once a patient experiences back pain he or she is more likely to experience it again. Estimates of recurrence at one year range from 24% to 80% (Hoy, 2010). Many environmental and personal factors influencethe onset and course of low back pain. Studies have found the incidence of low back pain is highest in thethird decade, and overall prevalence increases with age until th
08.03.2019 · radicular pain Establish treatment goals using shared decision-making: Patient goals Clinical goals Patient barriers Psychosocial factors. Develop a Treatment Plan. Patient education Self-care Non-pharmacologic Pharmacologic Implement a jointly agreed upon care plan: Patient education and training Self-management plan Reassessment plan Return to work plan 2-3 .