Transcription
The Family APGAR: A Proposal for aFamily Function Testand Its Use by PhysiciansGabriel Smilkstein, MDSeattle, WashingtonUnderstanding family function is an important aspect ofpatient care, yet a practical approach to the evaluation of fam ily function by the physician has not been devised. This paperintroduces a brief questionnaire that is designed to test fiveareas of family function. The acronym APGAR has beenapplied to the functional components of Adaptability, Partner ship, Growth, Affection, and Resolve. The use of the FamilyAPGAR is discussed, as well as ways of assessing family re sources and reporting data in a family problem-oriented rec ord. These guidelines are offered for the management of thefamily in trouble, so that the physician may view the use of theFamily APGAR in the context of clinical practice.Richardson, in 1948, was among the first tostress the necessity for physicians to view thepatient in the context of family. In his seminalbook on family dynamics in health care he noted,To say that patients have families is like saying that thediseased organ is part of the individual. Both facts seemtoo obvious to discuss, yet for a long time neither re ceived due recognition from the medical profession.1The significance of the patient as a familymember was elaborated further by Minuchin whowrote,The family, as an open socio-cultural system, is contin ually faced by demands for change. These demands aresparked by bio-psychological changes in one or more ofits members. . . ,2From the Department of Family Medicine, University ofWashington School of Medicine, Seattle, Washington. Re quests for reprints should be addressed to Dr. GabrielSmilkstein, Department of Family Medicine RF-30, Univer sity of Washington School of Medicine, Seattle, WA 98195.THE JOURNAL OF FAMILY PRACTICE, VOL. 6, NO. 6, 1978Today, although the concept of the patient as aninteracting member of a family unit is well ac cepted, a practical method still has not been de vised for the physician to use to collect data thatwill facilitate managing the family in trouble.A host of examinations and tests is available tothe physician for evaluating a diseased organ’sfunctional state. Similarly, in evaluating the fam ily, many questionnaires and procedures havebeen devised to establish the state of functionalintegrity of the family.3,4 However, none of thesemethods for testing the family has proven of prac tical value for daily use in the physician’s office.This paper will introduce a brief screeningquestionnaire called Family APGAR, which is de signed to elicit a data base that will reflect apatient’s view of the functional state of his or herfamily. It will also discuss ways of assessing fam ily resources and the use of a family problemoriented record that may be used by the physicianto improve family study, diagnosis, and manage ment.1231
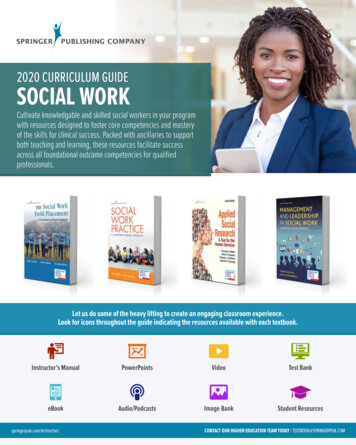
THE FAMILY APGARTable. Definitions of Family APGAR ComponentsComponentDefinitionAdaptationAdaptation is the utilization of intra and extrafamilialresources for problem solving when fam ilyequilibrium is stressed during a crisis.PartnershipPartnership is the sharing of decision making andnurturing responsibilities by fam ily members.GrowthGrowth is the physical and emotional maturation andself-fulfillment that is achieved by fam ily membersthrough mutual support and guidance.AffectionAffection is the caring or loving relationship thatexists among fam ily members.ResolveResolve is the commitment to devote time to othermembers of the fam ily for physical and emotionalnurturing. It also usually involves a decision toshare wealth and space.Definition of Family and Family FunctionWhen the physician interviews a patient for ahealth problem, the usual procedure is to gatheronly information concerning the patient’s familythat is pertinent to understanding a particularcomplaint. In most instances, the physician needsminimal or no family data to handle the complaint.Nevertheless, in some situations, knowledge ofthe structure and function of the patient’s familymay be required to resolve the health problem.For example, in evaluating a middle-aged manwith chest pain, it is important for the physician toinquire whether anyone in the patient’s geneticfamily has had coronary artery disease as well asto determine the structure and the function of thefamily to which the patient will return.Since family structure and function play a partin understanding and managing the complaint ofthe individual patient as well as of the family introuble, the following operational definition offamily is recommended for the physician involvedin family analysis: The family is a psychosocialgroup consisting o f the patient and one or morepersons, children or adults, in which there is acommitment fo r members to nurture each other.In this definition, family structure is definedsimply as the patient and one or more persons.Because structural or institutional relationshipsamong members are not specified, there is roomfor a wide range of family life-styles, including thetraditional nuclear family, communal groups, andnonmarried partners, whether heterosexual orhomosexual. Also in this definition the process ofnurturing is equated with family function thatpromotes emotional and physical growth and mat uration of all members.In order to establish the parameters by which afamily’s functional health can be measured, fivebasic components of family function were chosen.These components, which are defined in Table 1.were elected by the author since they appear torepresent common themes in the social science lit erature that deals with families. This empiricaldecision allowed the development of a familyfunction paradigm that may be likened to the1232THE JOURNAL OF FAMILY PRACTICE, VOL. 6, NO. 6, 1978
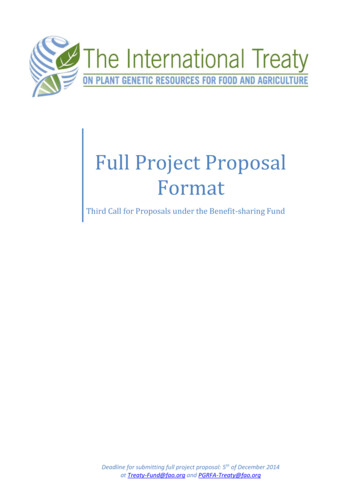
THE FAMILY APGARTable 2. Open-Ended Requests for Family Function InformationComponentRelevant Open-Ended QuestionsAdaptationHow have fam ily members aided each other in time ofneed?In what w ay have fam ily members received help orassistance from friends and community agencies?PartnershipHow do fam ily members communicate with each otherabout such matters as vacations, finances, medicalcare, large purchases, and personal problems?G rowthHow have fam ily members changed during the past years?How has this change been accepted by fam ily members?In what w ays have fam ily members aided each other ingrowing or developing independent life-styles?How have fam ily members reacted to your desires forchange?AffectionHow have members of your fam ily responded to emotionalexpressions such as affection, love, sorrow, or anger?ResolveHow do members of your fam ily share time, space, andmoney?body’s organ system, in that each component hasa unique function, yet each is interrelated to thewhole. The family in health may be considered tobe a nurturing unit that demonstrates integrity ofthe components of (1) Adaptability, (2) Partner ship, (3) Growth, (4) Affection, and (5) Resolve(APGAR).Family Function QuestionnaireWhen a family member reports the history of acrisis to a physician, the general status of this fam ily’s function can usually be discovered. Consid erable information about family function may beobtained when the patient describes how familymembers eat, sleep, and carry out home, school,and job responsibilities. Evidence of dysfunctionin these activities should alert the physician to theneed to evaluate family function in greater depth.THE JOURNAL OF FAMILY PRACTICE, VOL. 6, NO. 6, 1978To obtain more definitive data, the physicianmust use questions that are likely to elicit perti nent information on the five components of familyfunction. Table 2 lists some relevant open-endedrequests for information on family function. Al though open-ended questions are preferable be cause they can lead to the most detailed flow ofinformation, they often require more time than thephysician has available. Consequently, closedended questions, while limiting the scope of thepatient’s responses, can give data in a few minutesthat highlight the quality of the patient’s interac tion with his or her family and do not overburdenthe busy clinician.In 1973, Pless and Satterwhite introduced aFamily Function Index (FFI) that was developedas a “ simple, easily administered test to reflect thedynamics of family interaction.” 4'5 The FFI con sists of 15 questions and requires about 15 minutes1233
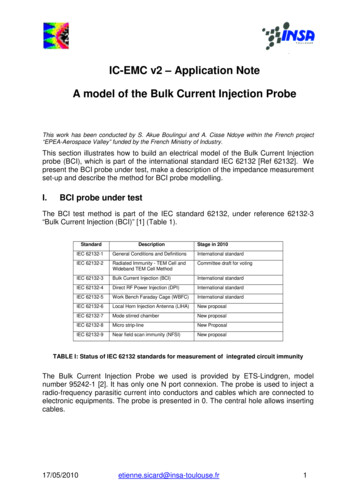
THE FAMILY APGARTable 3. Family APGAR QuestionnaireAlmostalwaysSome ofthe timeHardlyeverI am satisfied with the help thatI receive from my fam ily* whensomething is troubling me.I am satisfied with the w ay myfam ily* discusses items of commoninterest and shares problemsolving with me.I find that my fam ily* accepts myw ishes to take on new activitiesor make changes in my life-style.I am satisfied with the w ay myfam ily* expresses affection andresponds to my feelings such asanger, sorrow, and love.I am satisfied with the amountof time my fam ily* and I spendtogether.Scoring: The patient checks one of three choices which are scored asfollow s: 'Alm ost alw ays' (2 points), 'Som e of the tim e' (1) point, or'Hardly ever' (0). The scores for each of the five questions are thentotaled. A score of 7 to 10 suggests a highly functional fam ily. A score of4 to 6 suggests a moderately dysfunctional fam ily. A score of 0 to 3suggests a severely dysfunctional family.* According to which member of the fam ily is being interviewed thephysician may substitute for the word 'fam ily' either spouse, significantother, parents, or children.to administer. It estimates family function byevaluating areas of nuclear family interaction suchas marital satisfaction, frequency of disagreement,communication, problem solving, and feelings ofhappiness and closeness. The reliability of the FFIwas established by comparing index scores withratings of the same families by experienced Caseworkers. The FFI has been used to study the nu clear families of children with chronic physicaldisorders, and it is claimed by its authors to iden tify accurately which chronically ill children arelikely to experience secondary psychological diffi culties.The Family APGAR, a questionnaire that fea tures five closed-ended questions, is introduced bythe author as a screening test to give a rapid over view of the components of family function. Table 3demonstrates this new questionnaire. It is de signed so that it may be given to members of either1234nuclear or alternative life-style families. TheAPGAR acronym has been applied since it is feltthat the familiarity that physicians have with theApgar6 evaluation of the newborn will encouragethem to remember a similar format that scores thefunctional status of a family. Field tests with theFamily APGAR are presently being conducted andearly results are promising. A validity index forthis questionnaire is now being established utiliz ing both Pless and Satterwhite’s FFI and theevaluation of family function by social workersand psychologists.What Does the Family APGAR Measure?The questions in the Family APGAR are de signed to permit qualitative measurement of thefamily member’s satisfaction with each of the fivebasic components of family function. Table 4 liststhe functional components of the Family APGARTHE JOURNAL OF FAMILY PRACTICE, VOL. 6, NO. 6, 1978
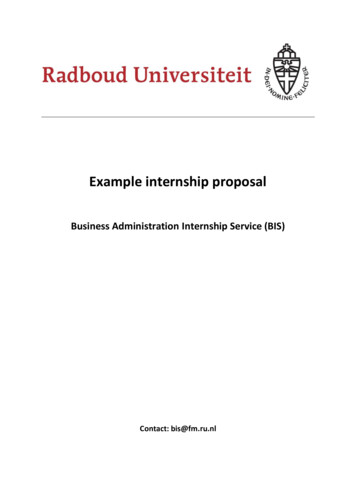
THE FAMILY APGARTable 4. What is Measured by the Family APGAR?ComponentAdaptationHow resources are shared, or the degree to which amember is satisfied with the assistance receivedwhen fam ily resources are needed.PartnershipHow decisions are shared, or the member's satisfactionwith mutuality in fam ily communication andproblem solving.G rowthHow nuturing is shared, or the member's satisfactionwith the freedom available within the familyto change roles and attain physical and emotionalgrowth or maturation.AffectionHow emotional experiences are shared, or the member'ssatisfaction with the intimacy and emotional interactionthat exists in a family.ResolveHow time (and space and money*) is shared, or them em ber's satisfaction with the time commitment thathas been made to the fam ily by its members.*Besides sharing time, fam ily members usually have a commitment toshare space and money. Because of its primacy, time was the only itemincluded in the Fam ily A PG A R; however, the physician who is con cerned with fam ily function will enlarge his/her understanding of thefam ily's resolve if he inquires about fam ily member's satisfaction withshared space and money.and indicates the qualitative data that may begained.The following vignettes are examples of patientproblems that have been evaluated by the FamilyAPGAR.Case 1Family crisis: A 40-year-old father died as a re sult of metastatic lung cancer after a hospital stayof three months. The physician record indicated aFamily APGAR score of 10. The questionnairewas completed by both spouses prior to the hus band’s hospitalization. The physician anticipatedthat existing resources would maintain the fam ily’s nurturing functions. Investigation of theAPGAR components revealed the following:Adaptability: The mother spent most of hertime in the hospital during the father’s illness.Relatives were called in as resources, and the fourtheJOURNAL OF FAMILY PRACTICE, VOL. 6, NO. 6, 1978children, ages 8 to 15, participated in householdchores and mutual support activities.Partnership: There were weekly family meet ings to discuss problems such as allowances, bor rowing clothes, and household responsibilities.Growth: Roles in the family were well definedand rather classical for a nuclear middle class fam ily; however, all family members had the oppor tunity to discuss change during Sunday night meet ings.Affection: A great deal of warmth and under standing was demonstrated by the parents with anopen display of affection. The children were af forded much physical touching and reassurancewhen needed.Resolve: The family functioned well as a unit.Parents demonstrated a commitment of time,space, and money, and they clearly indicated tothe children that the family came before work re-1235
THE FAMILY APGARsponsibilities.During the crisis period that followed thefather’s death there was a rapid gathering of re sources, eg, minister, relatives, and friends. Fam ily dysfunction was minimal. The children re mained at home to assist the mother during thefuneral and memorial services. The grief processwas shared by all members of the family.This family required little in the way of supportfrom the family physician. Intra and extrafamilialresources continued to maintain the family unitduring the post crisis period.C a se 2Family crisis: A 16-year-old daughter was ar rested for shoplifting. The juvenile officer recom mended individual counseling for the daughter.The family physician was consulted by themother. At the time of consultation a severely dys functional family was anticipated when a FamilyAPGAR score of 1 was obtained from the daugh ter, while the mother, age 39, scored 3. The fatherrefused to see the physician or complete theAPGAR questionnaire. The physician foresaw afamily that would require much aid in the way ofextrafamilial resources.Investigation of the APGAR components of thisfamily revealed the following:Adaptability: The mother was in charge of thefamily, but she claimed she received little or nosupport from her daughter or husband. A son,aged 10, was cooperative but his assistance waslimited since he had cerebral palsy and required awheelchair for ambulation. Father and daughterdid their own “ thing” and left mother to managemost of the home problems. There were no ex tended family members in the community.Partnership: Mother and daughter shared opin ions, but their differences were so marked therewas little cooperation. Daughter and father wereusually at odds. Father indicated that he wouldlike to see the daughter removed from the home(especially after the shoplifting episode). Motherand son had a close relationship and exchangedideas and feelings. The husband made decisionsregarding his activities, but he left household de cisions to the wife.Growth: Daughter had been allowed much free dom outside the home since age 12; however, herhome activities were restricted by the father. Forexample, he did not allow her to watch television.1236Shoplifting was the third arrest experienced by thedaughter. Her previous two experiences with thepolice were for drunken and disorderly conductand being a runaway. Mother had high educationalgoals for the children; however, daughter had a Daverage, and although the son tried, his educa tional accomplishments were limited.Affection: There was no evidence of physicalaffection when family members were togetherHusband and wife apparently related well at asexual level, but there was little else in the way ofemotional interchange. Mother and son seemed todemonstrate some measure of intimacy.Resolve: Husband helped meet physical needsof home and family, but he tended to spend as littletime at home as possible. He shared most of hispaycheck with his wife. The daughter spent muchof her time either isolated in her room or out of thehouse with her peers.The Family APGAR scores of 1 and 3 obtainedfrom the daughter and mother indicated to thephysician the gravity of family dysfunction. Thephysician elected to act as a facilitator and referthis family to a mental health clinic for familytherapy. The father initially would not cooperatewith the counselor, but he was finally convincedby the physician and juvenile officer to participatein a family discussion. Roles were discussed and amore equitable distribution of household tasks wasarranged. The 16-year-old daughter was assignedan advocate (college student as role model) by thejuvenile officer. The advocate reported that afterthree months the daughter had demonstrated someimprovement in her school work and claimed tohave established an improved relationship withboth her father and mother.When Should the Family APGAR Ques tionnaire be Used?Three situations have been identified in whichthe physician may need information on the func tional state of the patient’s family.1.Functional information is needed when thefamily will be involved with the patient’s care. Allillnesses and injuries represent some measure ofstress to the family. An understanding of thebaseline level of family function is necessarywhenever the physician wishes to involve thefamily in the care of the patient. In the case of apatient with coronary artery disease, informationon family function would assist in ascertaining theTHE JOURNAL OF FAMILY PRACTICE, VOL. 6, NO. 6, 1978
THE FAMILY APGARpatient’s ability to return home and play the role ofa passive convalescent. A high Family APGARscore would suggest that the family could adapt tothe crisis of the patient’s illness and role change. Alow score would warn the physician that the homeenvironment might be stressful to the coronarypatient. The physician might then wish to take acloser look at family member interaction beforesending the patient home.2. Family function data may be needed when anew patient is introduced into a physician’s prac tice. There is merit in seeing the family as a unit onat least one occasion,7 since such an encounterallows the physician to meet the family membersand gain some insight into family interaction.While the interview process does not usually allowthe physician time to gain an adequate view of thestatus of family function, giving the FamilyAPGAR questionnaire to the whole family permitsthe physician to establish a baseline view of familyfunction (See Case 3). Just as the pediatricApgar uses one and five-minute evaluations tojudge the progress of a newborn infant, the familyphysician may wish to administer the FamilyAPGAR at the first visit and repeat it in five yearsto judge the changes in functional status of a fam ily under his/her care.3. Family function information is essentialwhen the physician is involved in managing a fam ily in trouble. When a patient reports a familycrisis to the physician, it usually indicates that thefamily’s resources are inadequate to cope with theproblem. In this situation the Family APGARquestionnaire can highlight specific areas of weak ness in family function that interfere with the abil ity of family members to communicate or identifyresources. Furthermore, the family member’s re sponse to a given item may provide a lead ininitiating a discussion. For example, if the patientscores 0 on the question of “ I am satisfied with theamount of time my family and I spend together,”the physician could use an open-ended questionsuch as, ‘‘I see that you have a problem with theamount of time that your family spends together.Tell me about it.” Thus, the questionnaire servesas a timesaving device that will help the physicianfocus on the critical problems of the family introuble.What Are Family Resources?The family’s ability to adapt to or cope with aTHE JOURNAL OF FAMILY PRACTICE, VOL. 6, NO. 6, 1978crisis depends largely on its resources. Since thephysician is usually consulted only when the fam ily members are unable by themselves to identifyor utilize resources to meet a crisis situation, thephysician who wishes to give supportive therapyor make an appropriate referral for the dysfunc tional family will need to help family membersidentify and assess their resources. The majorfamily resources are Social, Cultural, Religious,Economic, Educational, and Medical. The ac ronym SCREEM may serve to remind the physi cian of the family resources. These resources areconsidered effective in a family when the followingconditions are met:1. Social interaction is evident among familymembers. Family members have well-balancedlines of communication within areas of extrafamilial social interaction such as friends, sport groups,clubs, and other community organizations.2. Cultural pride or satisfaction can be iden tified, especially in distinct ethnic groups.3. Religion offers satisfying spiritual experi ences as well as contacts with an extrafamilialsupport group.4. Economic stability is sufficient to provideboth reasonable satisfaction with financial statusand an ability to meet the economic demands ofnormal life events.5. Education of family members is adequate toallow members to solve or comprehend most ofthe problems that arise within the format of thelife-style established by the family.6. Medical care is available through channelsthat are easily established and have previouslybeen experienced satisfactorily.Pathology in the various family resources isconsidered to exist when the following conditionsare present:1. Social: The family is socially isolated fromextrafamilial groups. If extrafamilial aid is re quired the resource-poor family may not knowwhom to turn to for assistance. This situation isnot uncommon when a family undergoes a crisisshortly after moving to a new community. At theother end of the spectrum of social activity is theproblem of overcommitment. Under these cir cumstances family members are so involved withactivities outside the home that they become dis associated from their own family and may be un available as resources in times of family need.2. Cultural: The family has feelings of1237
THE FAMILY APGARcultural-ethnic inferiority or shame, often as aconsequence of having been subjected to years ofghettoization as well as vocational and educationaldiscrimination.3. Religious: Dogma and rituals are so rigid thatthey limit the family’s problem solving capacity.The physician must consider ethical questionswhen a crisis involves religious beliefs. Difficultiesoften arise when dealing with questions such ascontraception, abortion, and blood transfusions.Overcommitment to religious activities by onefamily member may limit his/her value as a re source to the rest of the family.4. Economic: Financial problems may make itdifficult for the family to meet the monetary de mands of a crisis. The physician must be aware ofthe family’s ability or inability to meet the eco nomic requirements of any plan that he designs. Ifthe physician’s plan, however ideal for the prob lem, is economically inappropriate, the plan is use less.5. Educational: Handicaps limit the ability offamily members to comprehend the problem or therecommended solution. Unless the physician or anappropriate counselor can explain to the family thenature of the problem and its solution, the familymembers cannot be expected to participate as re sources in problem solving.6. Medical: A family has not established linesof medical care or is unable to use health-carefacilities due to problems such as unwillingness toseek care, inadequate finances, language barriers,absence of transportation, refusal of care by alocal practitioner, or long-term or recurrent illnes ses that deplete family reserves.How Should a Data Base on the Family inTrouble be Collected?In practice, of course, the family is rarelyinterviewed as a unit. The family data base, ob tained from as many family members as possible,will therefore be a cumulative record that must bemodified as various members of the family con tribute to the account of the family’s crises, func tions, and resources.The workup of the family in trouble requires (1)identifying and evaluating the family’s crises, pres ent and past, (2) determining the level of familyfunction through the Family APGAR, and (3) as certaining the family’s resources through theassessment of family resources. This information1238should be noted in a practical and graphic record ing system.The problem-oriented record has been chosenby increasing numbers of physicians as an effec tive method of recording a patient’s health statusTo make this concept useful for family study anddiagnosis, the problem-oriented record for the in dividual is modified so that the format (data basenumbered problem list, titled plan, and follow-up)may be applied to the family. The goal of the Fam ily Problem-Oriented Record (Family POR)9is toprovide a vehicle that will systematize the study ofthe family and enhance the exchange of informa tion among health science students, teachers, andpractitioners.The data base of the Family POR is a record ofthree areas: the present and past family crises, theintra and extrafamilial resources, and the APGARcomponents of family function.The assessment is a report of (1) thesignificance of various crises to family mem bers,9-10 (2) the level of Family APGAR function,and (3) the status of family resources (SCREEMitems).The plan should note the intra and extrafamilialresources the physician will recommend to assistmembers in improving family function.The follow-up will record whether the plan waseffective or not, as well as the physician’s futureplans for the family.Guidelines for the Management of theFamily in TroubleThe primary responsibility of physicians in volved in family therapy is to match their personalresources (skills, knowledge, and attitudes in fam ily counseling) against the severity and complexityof a family’s functional disability. The FamilyAPGAR serves as a screening test for functionaldisability; however, as in all phases of medical in vestigation, the test must be put into perspectiveby the physician. In family therapy this is done byassessing the overall pattern of family function.Mild functional disability exists in a familywhose life-style may be adversely affected butwhich remains functionally intact; that is, there isa continuation of most nurturing activities. Inthese circumstances the plan requires that thefamily be given assistance in improving communi cation and identifying those resources needed tohelp resolve the crisis episode. Supportive coun-THE JOURNAL OF FAMILY PRACTICE, VOL. 6, NO. 6, 1978
THE FAMILY APGARseling may also be instituted to assist the familymembers most affected by the crisis.Case 3A family was evaluated as a unit as new mem bers of a practice. The Family APGAR scoreswere as follows: Father, age 58, 7; mother, age 54,9; son, age 22, 8; daughter, age 20, 9; and son, age16, 6. The physician recognized that with the ex ception of the 16-year-old son, and perhaps thefather, the Family APGAR scores suggested afamily that functioned well.The physician elected to speak with the parentsabout the test results. The father indicated that hehad been having some disciplinary problems withhis 16-year-old son. Permission was granted thephysician to invite the son to the office to discussthe Family APGAR test. The son was initiallyhesitant but he did comply. After an introductorydiscussion about the son’s routine health statusand activities, open-ended questions were askedrelated to the items that were scored low on theFamily APGAR, eg, “ You indicated on yourquestionnaire that you were not entirely satisfiedwith the way your family accepted your desires totake on new activities.” This question led to adiscussion of how strict the father had been re garding the son’s social activities, dress,homework, and television use. The 16-year-oldclaimed that he was responsible for most of theyard work, yet he received little; recognition for hisefforts. Father-son arguments had apparently beenescalating for about a year, and according to theson, in recent months the father seemed to be crit ical almost all the time.Permission was granted to the physician by theson to talk over the situation with the father. One40-minute session was held during which time thefather ventilated his feelings regarding his atti tudes about his youngest son. The physician spentan equal amount of time counseling the father onparenting a teenager. Major emphasis was given tooffering recognition and rewards for positive ac complishments, drawing up limited guidelines forbehavioral expectations, and giving the teenagerthat degree of independence that seemed appro priate for his age. The father was able to arrange acontract” with his son. A three-month reportindicated improved communication betweenfather and son, and apparently an improvement infamily function (son’s three-month FamilyTHE
From the Department of Family Medicine, University of Washington School of Medicine, Seattle, Washington. Re quests for reprints should be addressed to Dr. Gabriel Smilkstein, Department of Family Medicine RF-30, Univer sity of Washington School of Medicine, Seattle, WA 98195. THE JOURNAL