Transcription
Residency Training Profilefor Family Medicineand Enhanced SkillsPrograms Leadingto Certificates ofAdded CompetenceOutcomes of Training ProjectCollege of Family Physicians of CanadaMay 2021
The College of Family Physicians of Canada2630 Skymark AvenueMississauga, ON L4W 5A4Telephone: 905-629-0900Toll-free: 1-800-387-6197Email: academicfm@cfpc.ca 2021 The College of Family Physicians of CanadaAll rights reserved. This material may be reproduced in full for educational, personal, andnon-commercial use only, with attribution provided according to the citation information below.For all other uses permission must be acquired from the College of Family Physicians of Canada.How to cite this documentFowler N, Wyman R, eds. Residency Training Profile for Family Medicine and Enhanced Skills Programs Leadingto Certificates of Added Competence. Mississauga, ON: College of Family Physicians of Canada; 2021.AcknowledgementsThe College of Family Physicians of Canada (CFPC) thanks the many committees, departments offamily medicine, resident and medical student groups, Chapters, partner and specialty organizations,and individuals (CFPC members, professional colleagues, CFPC staff, and members of the public whocontributed to the development of this document. The Residency Training Profile was created underthe leadership of the CFPC’s Family Medicine Specialty Committee and overseen by the dedicatedOutcomes of Training Project staff in the CFPC’s Academic Family Medicine Division.
Family Medicine Specialty Committee (fall 2018 to spring 2021)Jennifer Hall (Chair)Armand AalamianBilal Akil (Resident)Sandra BannerJessica BeatonLisa BonangFraser BrenneisJohn ChmelicekSabrina Dzafovic (Resident)José FrançoisDavid GassJames GoertzenLee GreenDaniel GrushkaErich HanelKenneth HarrisEdouard HendricksAaron JohnstonKathrine LawrenceAnne-Marie MacLellanAinslie MihalchukPaul MironBaijayanta MukhopadhyayDominique PilonVivian RamsdenDavid RossKaren SchultzDave ThomasGalt WilsonMark Woo (Resident)Keith Wycliffe-JonesOutcomes of Training ProjectAdvisory GroupOutcomes of TrainingScholarship GroupEditors, French-languagetranslators, and reviewersNancy Fowler (Chair)Sandra BannerBeth BeaupreGuillaume CharbonneauMarie GirouxDouglas GrantJennifer HallKathrine LawrenceKaren SchultzKeith Wycliffe-JonesNancy Fowler (Chair)Kathrine LawrenceLuce Pélissier-SimardVivian RamsdenKaren SchultzKeith Wycliffe-JonesMarcel ArcandAudrée BédardJosette CastelGuillaume CharbonneauPierre FrémontMarie GirouxLucie HamelinCarol HiltonStéphanie MarsanLuce Pélissier-SimardClaude ToppingGolda TradounskyRichard WaldolfOutcomes of Training Project staffNancy Fowler (Project Lead)Michelle Mayne (Project Manager)Nadia Mangal (Project Coordinator)Roy Wyman (Project Lead, CACs)Tatjana Lozanovska (ProjectManager, CACs)Ivy Oandasan (Project Lead,Evaluation)Monica Aggarwal (ProjectResearcher)Lorelei Nardi (Project Manager,Evaluation)Cheri Nickel (Project Librarian)Gregory Nasmith (Consultant,Literature Review)Patricia Nicholson (Consultant,Report Writing)
Table of contentsIntroduction. 1Glossary of key terms. 5Residency Training Profile: Family medicine. 7Primary care in the community/office setting.7Maternal and newborn care.14Emergency care.17Home and long-term care.20Hospital y medicine Core Professional Activities at a glance.31Residency Training Profile: CAC-related enhanced skills. 33Addiction Medicine.33Care of the Elderly.36Emergency Medicine .39Enhanced Surgical Skills.45Family Practice Anesthesia.49Obstetrical Surgical Skills.52Palliative Care.56Sport and Exercise Medicine.61Enhanced skills Core Professional Activities at a glance.64Appendix 1: Procedure Skills in Family Medicine. 67References. 72
IntroductionWhat are we aiming for in familymedicine residency training?The successful end point of residency is graduatepreparedness—that is, for them to be confident,competent, and able to adapt to and apply their abilitiessuccessfully in any context. This mandate is captured inthe College of Family Physicians of Canada (CFPC)’s Stand ards of Accreditation for Residency Programs in FamilyMedicine (Red Book) as the goal of training: to trainresidents who are competent to enter and adapt tothe independent practice of comprehensive familymedicine anywhere in Canada.1The CFPC Residency Training Profile for Family Medicineand Enhanced Skills Programs Leading to Certificates ofAdded Competence (Residency Training Profile) is basedon the FMPP and elaborates on what we are aimingto achieve with family medicine residency training inCanada across all the dimensions of professional practice: A unique professional identity and value system asdescribed in the Four Principles of Family Medicine3 Family medicine competence as described in CanMEDS–Family Medicine 20174 and the Assessment Objectives forCertification in Family Medicine5 A comprehensive scope of practice enabled by a setof Core Professional Activities (CPAs)The dynamic threshold of enter and adapt reflects thefundamentally generalist nature of family medicineand recognizes that residency is just a part of thelearning journey that continues across a career. Participation in a collaborative work environmentthat enables the collective delivery of comprehensiveand continuous care, as defined by the Patient’sMedical Home vision6In 2018 the CFPC published the Family MedicineProfessional Profile (FMPP), which describes thecollective commitment of family physicians toproviding comprehensive care close to home.2The Residency Training Profile was developed toreflect our aspirations for a socially accountable familymedicine workforce in Canada. While we adhere tothe original social accountability tenets defined by theWorld Health Organization,7 in workforce and evaluationResidency Training Profile1
terms, this is often described using measures of the mix,distribution, and scope of family physicians needed tomeet the needs of everyone in Canada.We are defining CPAs as tasks considered to beessential to preparing trainees for professional practice.Collectively, the CPAs in the core family medicineResidency Training Profile define a scope of training thatenables residents to achieve the broad skill potentialnecessary for comprehensiveness, which is developedfurther in a family physician’s practice through lifelonglearning. Nobody does it all—or alone—but we arecalled upon to prepare all graduates for the diversecommunity practice needs across the country. Afterall, Certification in the College of Family Physiciansof Canada (CCFP) is a Special Designation that hasmeaning and portability across the country.This is a potential shift in thinking for some; residentsshould not require enhanced skills training simply toconsolidate the core skills needed for this scope of care.It is incumbent upon us to advocate for the resources,including the time/length of training required, thatroutinely allow residents to consolidate the skills andconfidence required for independent practice.The Residency Training Profile clarifies that the principleaim of enhanced skills residency training leading toCertificates of Added Competence (CACs) is to enableadvanced practice and health systems leadership. CACholders are local and systems-level care champions,functioning as resources to their colleagues andcommunities. They support continuity and extend therole of the comprehensive family physician by providingbackup and consultation to colleagues treating patientswith challenging conditions, ideally integrated in aPatient ‘s Medical Home practice environment.Some of the CPAs covered in the enhanced skillsportion of the Residency Training Profile overlap withthose in the core family medicine portion. This simplyreflects the fact that there are natural commonalitiesin the scopes of practice for family physicians with andwithout CACs. Where overlap in the CPAs appears, thisdoes not mean that a family physician requires aCAC to conduct this activity.How is the ResidencyTraining Profile organized?The Residency Training Profile represents the expectedscope of training in family medicine encompassingboth core family medicine and CAC-related enhancedskills training.For core family medicine, the Residency Training Profileis organized into sections using the eight major areasof professional responsibility noted in the FMPP: Primary care Maternal and newborn care Home and long-term care Emergency care Hospital care Advocacy Leadership ScholarshipAll sections should be read together as an integratedwhole. The Residency Training Profile is structuredin sections for ease of reference and to correspondwith the FMPP, not to imply a division of professionalactivities. Areas of practice such as Advocacy orMaternal and newborn care are listed individuallynot because they are separate from primary care, butbecause they are activities that cut across care settingsand regulatory jurisdictions.We want to be clear with audiences outside familymedicine that the work of family physicians extendsbeyond traditional office-based primary care andincludes other dimensions of home and hospitalcare, such as intrapartum care. Similarly, Leadership,Scholarship, and Advocacy are intertwined witheach other and all the clinical domains, but they arediscussed individually here to give them their ownfocus and importance.For CAC-related enhanced skills, the Residency TrainingProfile is organized into sections using the eightResidency Training Profile2
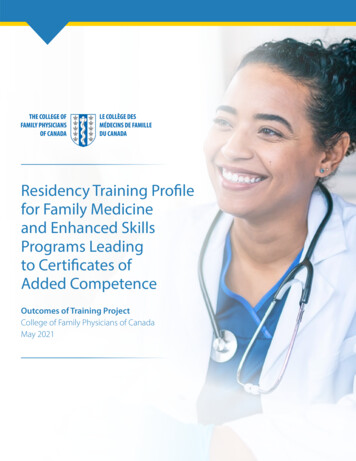
Category 1 domains of care. Category 1 domains arethose that are CFPC-defined and recognized and areaccredited nationally: Addiction Medicine Care of the Elderly Emergency Medicine Enhanced Surgical Skills Family Practice Anesthesia Obstetrical Surgical Skills Palliative Care Sport and Exercise MedicineEach section of the Residency Training Profile containsthree features:1. Practice narrative: A description, based on fieldresearch, that portrays the value, meaning, andscope of work done by family physicians in Canadaacross diverse practice settings.2. Training statement: A statement thatencapsulates where residents are expected to bein their learning journey by the end of residency,for which the CPAs provide more detail.3. Core Professional Activities (CPAs): A set ofprofessional activities or tasks for which residentswill be prepared at the completion of training.a purposive sample of family physicians, residents,medical students, professional colleagues, andmembers of the public using a structured narrativewriting exercise.8 Quotations have been includedanonymously throughout this document with thewritten consent of participants. Narrative data werethematically analyzed and organized according to theprimary responsibilities defined in the FMPP,2 resultingin the Practice narrative and CPA sections. A series ofexpert panel discussions and surveys helped furtherclarify the scope and expectations of residency training,resulting in the Training statement sections. TheResidency Training Profile builds on field research donefor the Triple C Competency-Based Curriculum9—therenewed approach to the delivery of family medicineeducation in Canada that the CFPC launched in 2011—and the assessment objectives, and it aligns with othernational frameworks and guidance documents, some ofwhich are still in development.The dynamic nature of the health care environmentand lessons learned about the evolving role of thefamily physician during the COVID-19 pandemic werealso taken into consideration.Once fully implemented, the Residency Training Profilewill be subject to regular review and revision as partof the CFPC’s Accreditation Standards ImprovementCommittee process, which will be informed by aformal and ongoing program evaluation.How was the ResidencyTraining Profile developed?How will the ResidencyTraining Profile be used?The Residency Training Profile was developed underthe direction of the CFPC’s Family Medicine SpecialtyCommittee, which is responsible for defining thediscipline of family medicine for the purpose of settingeducational standards. Independent input aboutthe work of family physicians was gathered fromWithin the standard-setting function of the CFPC, theResidency Training Profile describes the overall aimand expected scope of family medicine residencytraining. It is used in conjunction with other existingpolicy documents and frameworks of the CFPC, asoutlined in Figure 1.Residency Training Profile3
Figure 1. An integrated picture of what we are aiming for in family medicine residency trainingThe Residency Training Profile is a guidance documentthat can be used by multiple audiences and applied tovarious scenarios: The CFPC: The Residency Training Profile informsaccreditation and certification standards. It servesas a scoping definition of comprehensiveness forstandard-setting along with national evaluation andresearch purposes. Residency program leadership: The practicenarratives bring to life the Four Principles of FamilyMedicine and may be an aid to learners in thedevelopment of their professional identities. TheResidency Training Profile can be used as a guidefor curriculum/assessment mapping and periodicreview with residents. Family medicine teachers: The practice narrativesbring to life the Four Principles of Family Medicineand may help learners develop their professionalidentities. The CPAs may be used to focus teachingon particular activities of practice combined withthe CanMEDS-FM competency objectives of alearning experience. Residents and medical students: The ResidencyTraining Profile offers a rich description of familymedicine as a career. It describes the learningjourney and outlines the expected thresholdof preparedness for practice. It can be used tomonitor and reflect on a trainee’s own learning andprofessional identity formation. Medical regulatory authorities and other healthauthorities: The Residency Training Profile clarifiesthe scope of residency training in family medicine. Itcan be used to inform credentialling decisions andprocesses. Colleagues/public: The Residency Training Profileexplains the scope of family medicine residencytraining, provides a rich description of the careprovided by family physicians, and expresses ourvalues and philosophy of care. It can be used toeducate and advocate with the public and otherson the important roles that family physicians play inthe health care system.Residency Training Profile4
Glossary of key termsclinical coach: A teacher who provides role modelling,teaching, feedback, and assessment arising from thecare of patients.10continuity of care: Is a core value of family medicinethat improves physicians’ and patients’ satisfactionand patient outcomes.11 The concept of continuity ofcare in family medicine originally had four domains:chronological, geographical, interdisciplinary, andinterpersonal.12 It has subsequently been describedas a combination of informational, relational, andmanagement continuity. For further details seeglossary terms for informational, management, andrelational continuity.Core Professional Activity (CPA): The CFPC defines aCPA as a task or group of tasks considered to be essentialin preparing residents for professional practice.cultural humility: A process of self-reflection tounderstand personal and systemic biases and to developand maintain respectful processes and relationshipsbased on mutual trust. Cultural humility involveshumbly acknowledging oneself as a learner when itcomes to understanding another’s experiences.13cultural safety: An “outcome based on respectfulengagement that recognizes and strives to addresspower imbalances inherent in the health caresystem. It results in an environment free of racism anddiscrimination, where people feel safe when receivinghealth care.”14entrustable professional activity: A unit ofprofessional practice (a task or group of tasks) thatcan be fully entrusted to a trainee once they havedemonstrated the necessary competence to executethis activity unsupervised.15health care equity: All people, regardless of socioeconomic status, gender, sexual orientation, race,ethnicity, or other social factors are able to receive highquality, appropriate health care and achieve optimalhealth and length of life. Health equity may require thatsome people use a greater proportion of health careresources than others and necessitates the eliminationof gaps in and barriers to optimal care for all.16informational continuity: The capacity of thatinformation to travel with the patient and throughoutthe health system, between providers and over time,to facilitate a continuous care experience.17management continuity: The extent to whichservices delivered by different providers are timelyand complementary such that care is experienced asconnected and coherent.18practice improvement: Uses quality improvement,practice-level data, and research to continuouslyimprove care, the patient experience, health systemefficiency, and the work experience of health careproviders.19 Practice improvement aims to build aculture in health care that recognizes how everyone“has two jobs when they come to work every day: todo their work and to improve it.”20 Thus, it requiresbeing reflective and curious about one’s own practiceand behaviour while focusing on improving patientoutcomes and experiences.21Residency Training Profile Glossary5
psychological safety: The degree to which peopleview their environment as conducive to interpersonallyrisky behaviours such as speaking up or asking for help.When psychologically safe, one holds the belief thatthey will not be punished or humiliated for speakingup with ideas, questions, concerns, or mistakes.22relational continuity: The ongoing relationshipbetween a patient and health care provider(s) thatallows knowledge of past health events and care,as well as the anticipated future provision of care, toinform and influence current care. This should resultin care that is well suited to the patient’s needs andpreferences.23social accountability: The direction of education,research, and service activities toward addressingthe prioritized health concerns of the community,region, and/or country. Priority health concerns areto be identified jointly by governments, health careorganizations, health professionals, and the public.7systemic or institutional racism: Consists of “patternsof behaviour, policies or practices that are part of thesocial or administrative structures of an organization,and which create or perpetuate a position of relativedisadvantage for racialized persons.”24 According tothe Ontario Human Rights Commission, these may“appear neutral on the surface but, nevertheless, havean exclusionary impact on racialized persons.”25trauma-informed care: This approach recognizeshow common trauma is and how it can affect allaspects of people’s lives, including their interactionswith service providers. For family physicians, taking atrauma-informed care approach involves creating asafe space for patients and acknowledging how theirlived experiences can affect the social determinantsof health. Rather than causing patients to relive orreflect on traumatic experiences, this approach to careemphasizes the strengths developed from survivingtrauma and how that resiliency can foster healing.With Indigenous patients, this includes understandinghow colonization continues to affect both Indigenousindividuals and communities in Canada. By not takinga trauma-informed care approach, care providers mayinadvertently cause patients to be re-traumatized andfeel unsupported or blamed. This may discourage themfrom seeking health care and related services in thefuture.26underserved: Individuals and communities who donot have the opportunity to reach and obtain accessto appropriate health care services based on theirperceived need for care.27Residency Training Profile Glossary6
Residency Training Profile: Family medicinePrimary care in thecommunity/office settingPractice narrativeHaving a practice—that is, caring for a group of patientsover time with all that this entails—is the essenceof being a family physician, and it is the professionalhome base for other activities. Accompanying patientson their care journeys over time, getting to knowthem personally, and understanding what mattersin the context of their lives are core to the work andprofessional identity of family physicians.“Primary care includes the day-today clinical in-office practice of familyphysicians. However, this is not limitedonly to dealing with point-in-time careof patients presenting with concerns/conditions. While comprehensive andcontinuous care sound like buzzwords,they are fundamental to effective primarycare; knowing a patient in the context ofthat patient’s circumstances and history(health and social) is essential in mostaccurately diagnosing and appropriatelytreating patients.”Family physicians are the often their patients’first and mainpoint of contact with the health care system, providingflexible access through coverage arrangements as partof a commitment to comprehensive care. They have anoverarching responsibility for the total care of patientsand family practices are the hub of care coordinationand medical documentation in an electronic medicalrecord that also serves as a source of data for practiceimprovement activities.The clinical case mix on any given day is highly varied,requiring versatility. Family physicians typically seeup to five patients per hour, in 10- to 30-minuteappointments, depending on the nature of theencounters. A high degree of continuity enablesmultiple issues to be dealt with in a single visit. Thereare many behind-the-scenes patient care and practiceresponsibilities, integrated across multiple settings.“I spend a lot of time outside of thepatient encounters reviewing test results,writing consultation letters, filling outforms, and making phone calls. I spendtime advocating for system changeswhen I can see that patients’ needs arenot being met. Sometimes I will travel toa nursing home, a patient’s home, or thehospital to see patients in those settings.In addition, I must spend time figuringout the billing system so I can get paidfor the work. I need to manage staff inour office and mange glitches with thecomputers, printers breaking down, orrunning out of toner. I have needed tolearn how to use an EMR system.”There is a great deal of variability in practicearrangements, but increasingly family physiciansparticipate in group and interprofessional teampractices where comprehensiveness is achievedas a shared responsibility with practice colleaguesand referrals are made to other medical specialistswhen necessary. The point at which a referral is madeis individual, and over time family physicians oftendevelop niche areas of expertise that they share withcolleagues as part of peer education or as informalconsultations. Case conferences and clinical teammeetings support collaborative patient care, and familyphysicians also work virtually to monitor and supportResidency Training Profile Family Medicine Primary care in the community/office setting7
patients with other colleagues in a rapidly evolvingclinical and technological environment. Clinical work isintegrated across care settings and is combined withadministrative, leadership, and teaching activities tomake for a busy and layered work schedule.“My main activities include directpatient care or patient care by mylearners under my supervision. Myteaching roles include undergraduatelearners, postgraduate family medicinelearners, and faculty. I see all patients! Mypractice is quite varied in that regard. Ihave patients of all ages, genders, and pregnant patients.”Compassion and social justice are strong valuesmotivating outreach and community engagement toensure care is inclusive and health equity is promoted.Family physicians think and work at both theindividual patient and population health levels andseek to assess and integrate their practices in the localcontext and in the broader health care community.They are community champions and resources forhealth promotion and public education.Training statementAll graduates can take responsibility for a practiceand provide comprehensive primary care andcontinuity to a defined group of patients, inpartnership with other health care colleagues.Care is provided in and outside the office settingto achieve continuity and comprehensiveness.They provide patient-centred, culturally safe,and trauma-informed care to all patients,contributing to health equity. They are preparedfor the following CPAs.Core Professional ActivitiesManage the practiceCPA 1. Provide first-contact access and relational continuity of care as part of an overall systemof care to the practiceThis involves a range of related activities:a. Maintain a regular schedule that provides first-contact access and relational continuity for a broad range ofpatient care needsb. Provide in-person care as an essential part of patient-centred carec. Provide virtual care to enhance first-contact access and relational continuity for patientsd. Plan access and outreach for patients who are unable to attend the officee. Participate in on-call coverage, providing medical care on evenings, weekends, or public holidays as part ofa group commitment to access for the practiceResidency Training Profile Family Medicine Primary care in the community/office setting8
CPA 2. Manage the total care of patients to provide informational and management continuityThis involves a range of related activities:a. Maintain an electronic medical record for each patient/encounter as part of a longitudinal patient recordb. Support and coordinate patient care across settings and care transitionsc. Follow up on patient encounters, monitoring the results of investigations, consultations, etc., and notifyingpatients with results, as appropriated. Complete medical forms and documentation to support patient care and repor
ards of Accreditation for Residency Programs in Family Medicine (Red Book) as the goal of training: to train residents who are competent to enter and adapt to the independent practice of comprehensive family medicine anywhere in Canada .1 The dynamic threshold of enter and adapt reflects the fundamenta