Transcription
International journalof ofResearchandReview in inHealthSciences, July linaryResearch, January -2015sZInternational Journal of Recent Advances in Multidisciplinary ResearchVol. 02, Issue 01, pp.0182-0186, January, 2015Case ReportFLEXIBLE DENTURE FOR PARTIALLY EDENTULOUS ARCHES - CASE REPORTS*Dr.Ashish.R.JainDepartment of Prosthodontics, Tagore Dental College and Hospital, Rathinamangalam, Vandalur Post,Chennai-600127, IndiaARTICLE INFOABSTRACTArticle History:Conventional fixed partial dentures, implant supported Fixed Partial Dentures (FDPs) and removablepartial dentures are the most common treatment modalities for the aesthetic and functionalrehabilitation of partially edentulous patients. Hard and soft tissue undercuts are frequently encounteredin the fabrication of prosthesis in partially as well as completely edentulous arches. Removable castpartial dentures are used as definitive removable prostheses when indicated, but location of clasps mayaffect aesthetics. So, when patient is concerned about aesthetics, flexible partial dentures which isaesthetically superior to flipper and cast partial dentures, may be considered. This article is an effort toreview the various commercially available flexible denture base materials and highlights theirindications and special instructions in wearing and maintenance of the same.Received 27th October, 2014Received in revised form05th November, 2014Accepted 09th December, 2014Published online 31st January, 2015Keywords:Flexible Denture,Valplast, Sunflex,.Flexiplast,Undercuts,Acrylic Clasps,FlipperINTRODUCTIONUnilateral or bilateral undercuts are frequently encountered andmay complicate successful fabrication of denture prosthesis.Management of these situations conventionally includesalteration of the denture prosthesis bearing area, adaptation ofthe denture base, careful planning of the path of insertion andthe use of resilient lining material. An alternative dentureprosthesis design in which optimal flange height and thicknesscan be achieved is by using flexible denture base material. It isnylon based thermoplastic material that does not sacrificefunction and preserves aesthetics. Soft dentures are an excellentalternative to traditional hard-fitted dentures. Traditionallyrelining dentures with a soft base increases comfort at the costof chewing efficiency. To make up for the loss of chewingefficiency, denture wearers would use dentures adhesive whichcauses its own problems. A flexible material is now an optionthat does not trade off the ability to eat (Maurice, 1964; Parvizi,2004)Flexible DenturesSoft dentures are generally used when traditional denturescause discomfort to the patient that cannot be solved throughrelining. Soft dentures are not the same as a soft reline fortraditional dentures.*Corresponding author: Dr.Ashish.R.Jain,Department of Prosthodontics, Tagore Dental College and Hospital,Rathinamangalam, Vandalur Post, Chennai-600127, India.Soft relines use a soft putty-like substance to separate gumsfrom the hard acrylic in dentures. Flexible dentures use aspecial flexible resin that prevents them from chafing thegums, allows the wearer to chew properly. It also provides asoft base that prevents the gums from being rubbed. Some ofthe commercially available products are Valplast, Sunflex,Duraflex, Flexite, Proflex, Lucitone, Impak where as valplast,Sunflex and lucitone are monomer free.VALPLASTValplast is a flexible denture base resin that is ideal for partialdentures and unilateral restorations. The resin is abiocompatible nylon thermoplastic with unique physical andaesthetic properties that provides unlimited design versatilityand eliminates the concern about acrylic allergies. The ValplastFlexible Partial allows the restoration to adapt to the constantmovement and flexibility in the mouth. The flexibility,combined with strength and light weight, provides total comfortand great looks. The preparation is relatively simple. TheValplast partial is virtually invisible because there are no metalclasps and the material itself blends with the tissue in mouth.While the cost is often higher than a partial made with visiblemetal clasps. The Valplast flexible partial involves only noninvasive procedures (Parvizi, 2004 and Stafford et al., 1986).
International Journal of Recent Advances in Multidisciplinary ResearchSUNFLEXSunflex Partial Dentures are made from a strong biocompatiblenylon thermoplastic, and are unbreakable, yet lightweight andtranslucent which allows natural tissue to show through. Thesunflex flexible denture base materials are virtually Invisible,Unbreakable, Metal-Free, Lightweight and incrediblyComfortable. The sunflex flexible denture base materials aremore stain-resistant than other flexible acrylics, these dentureshas the perfect degree of flexibility, these can be relined andrepaired, these dentures will not warp or become brittle, theseflexible dentures stands aesthetically superior removablepartial with full functionality and comfort, these dentures areideal for patients considering a removable partial and thosewho do not want metal clasps and these dentures are perfectfor patients that are allergic to monomer (Parvizi, 2004 andYunus et al., 2005).0183 The material is exceptionally strong and flexible. Freemovement is allowed by the overall flexibility. Complete biocompatibility is achieved because the materialis free of monomer and metal, these being the principlecauses of allergic reactions in conventional denturematerials. Clinicians are able to use areas of the ridge that would notbe possible with conventional denture and partialtechniques. Patient can wear appliances that wouldnormally not be comfortable. Flexible dentures will not cause sore spots due to negativereaction to acrylic resins and will absorb small amounts ofwater to make the denture more soft tissue compatible. Flexible dentures may be used as an alternate treatmentplan in rehabilitating the anomalies such as ectodermaldysplasia.Disadvantages of flexible denturesPRO-FLEXPro-flex is the flexible denture base material which can be usedfor Full and Partial Flexible Dentures. Pickett DentalLaboratory has been offering Pro-flex full and partial flexibledentures since 1998. Pro-flex denture material be indicated insome of the Anatomical considerations enables the material toeffectively engage tooth and tissue undercuts. Also, Pro-flex ishypo-allergenic recommended for patients with known acrylicor metal sensitivities. Aesthetically the material is semitranslucent, allowing the prosthetic to better blend with thecolour of the natural gum tissue. With Pro-flex flexible partials,there are no metal clasps. Proflex full and partial flexibledentures are easily adjusted by the dentist. This material istough, durable and dense, manufactured with thousands ofpounds of pressure and vacuformed to fit the model perfectly.The final layer is a flexible resin composite that is firm enoughto hold teeth under all occlusal loads, but flexible enough toallow delivery of the dental appliance without adjusting anyundercuts. Simply warm the denture with running water tobring it up to body temperature before inserting it. Pro-flexpartial and full dentures can be repaired, and the full denturescan be relined here at the laboratory with Pro-flex Soft Linematerial. Pro-flex flexible dentures are set up with the samequality teeth used in acrylic dentures and cast partials (Parvizi,2004).BIO DENTAPLASTIt is a semi-crystalline thermoplastic material with a linearstructure characterized by high crystallinity. The materialshows good physical and chemical properties such as increasedhardness, tensile strength, and good dimensional stability. Thematerial is opaque and prevents glare colour metal. Availableshades A2, A3, B2, B3 (similar to vita shade) (Yunus et al.,2005 and Keenan et al., 2003).Advantages of flexible denturesFlexible dentures have got various advantages over thetraditional rigid denture bases. Translucency of the material picks up underlying tissuetones, making it almost impossible to detect in the mouth. No clasping is visible on tooth surfaces (when used inmanufacturing of clear clasps), improving aesthetics. Flexible dentures generally not used for long termrestorations and is intended only for provisional ortemporary applications. Flexible dentures tend to absorb the water content and willdiscolor often. Metal frame partial dentures remain the" standard" forlong-term restorations. When grinding this prosthesis, proper ventilation, masksand vacuum systems should be used and the procedure istechnique sensitive. Extreme caution is necessary when processing to avoid skincontact with the heated sleeve, cartridge, furnace, heatingbay, hot cartridge, injection insert, piston head adapter, hotflasks, and heat lamps.Indications of flexible dentures As a provisional in lieu of restorative temporaries or astandard acrylic partial As obturators with maxillectomy procedures. In single denture cases. The patient prefers not to use a fixed restoration In challenging cases including pediatric patients, cancerousmouths or cleft palates. Cosmetic veneers to mask gingival recession, splints andnesbits. When protuberant bony formations restrict the insertion ofan acrylic full denture When the patient is allergic to acrylic. A patient with systemic sclerosis and microstomia.Contraindications of flexible dentures The fabrication of flexible partial dentures iscontraindicated in patients with insufficient interarch space( 4mm space for placement of teeth), prominent residualridges where there is less space for placement of teeth. Flat flabby ridges with poor soft tissue support whichrequire more rigid prosthesis.Case Report IA 55 year old female patient reported to the Department ofProsthodontics, with a chief complaint of multiple missingteeth.
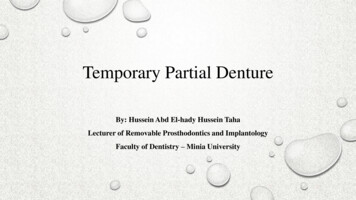
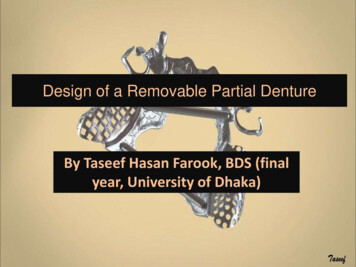
International Journal of Recent Advances in Multidisciplinary Research0184The patient presented with partially edentulous arche withbilaterally missing posterior teeth in maxilla (Kennedy classIII, Modification I) as shown in Fig .1. Some of the remainingteeth had carious lesions, cervical abrasions and cariousexposures. Carious and cervically abraded teeth were restoredand root canal treatment of carious, exposed teeth was done.Flexible partial denture was fabricated for replacing maxillaryposterior teeth, because clasps placed on canines with flexiblematerial are aesthetically good and more retentive because oftheir extensions into undercuts which present lateral tomaxillary tuberosity. Fig. 2.3.Figure 4. Kennedys class IV modification I partial archFigure 1. Kennedys class III modification I partial arcFigure 5. Fabrication of sunflex partial dentureMaxillary anterior missing teeth were restored with flexiblepartial dentures Fig. 4.5.6. And he was very much satisfiedwith aesthetics as well as with function of the prosthesis.Figure 2. Sunflex flexible partial dentureFigure 6. Insertion of flexible partial denture-frontal viewFigure 3. Insertion of flexible partial denture-frontal viewCase report 2The second patient (35yrs male) presented with MultipleMaxillary anterior missing teeth (Kennedys class IV,modification I) Fig .2. He was very much apprehensive aboutthe appearance of metal clasp and did not want any metalprosthesis in his mouth.Figure 7. Kennedys class II modification I partial arch
International Journal of Recent Advances in Multidisciplinary Research0185 Dentures were tried in patient’s mouth and after approvalby patient dentures were processed in injection system. Dentures were finished, polished and inserted. Occlusionwas evaluated and adjusted. Posto perative instructions on how to insert the prosthesesand with instruction on adequate oral hygiene maintenance.The two years follow up of all the three patients showed mildyellow staining of the prostheses due to improper care of theprostheses.Figure 8: Kennedys class IV partial archFigure 9. Insertion of sunflex partial dentures-occlusal andfrontal viewCase report 3The third patient (22yrs female) presented with multipleanterior missing teeth in both maxilla (Kennedys class IImodification I) and mandible (Kennedys class IV). Her primeconcern was esthetics and economic status, as she was notprepared to afford for fixed prosthesis. Fig. 7.8.9.Procedure Diagnostic casts were prepared using alginate impressions. Cast were mounted on surveyor and were analyzed on thebasis of present undercut. The diagnostic casts were articulated (semi adjustablearticulator) using centric relation record and face bowtransfer to evaluate inter arch space. Final Impressions were made using polyvinyl siloxane lightbody material of both the arches. In case of distal extensions cases Primary impressions weremade with alginate and primary casts were made andspecial tray prepared with self cure acrylic resin. Definitiveimpressions were made using custom trays bordermoulding was done with low fusing compound and finalimpressions were made using polyvinylsiloxane light bodymaterial. Final casts were made with Type III dental stone Maxillomandibular relationships were recorded with checkbite method Definitive casts were mounted on semi adjustablearticulator. Shade selection was done and artificial acrylic resin teethwere arranged.DISCUSSIONRemovable partial denture is commonly used for treating thepatients who are not good candidates for conventional fixedpartial dentures and implant supported prosthesis. Theseprostheses can be fabricated from metal alloy, acrylic resin andthermoplastic resins. The removable cast partial denture is adefinitive prosthesis which has been in use in dental professionsince decades for rehabilitation of partially edentulous patients.It consists of a metal base (made up of base metal alloys,commonly with cobalt-chromium alloy), with acrylic teethattached to it. Metal retentive clasp holds the cast partialdenture in place. The metallic appearances of the clasp may berestrictive, treating the patient who are very much concernedabout the aesthetics. When maxillary posterior teeth aremissing and only anterior teeth are present, placement ofmetallic clasps on canines may not be acceptable to fewpatients (Naylor et al., 1983). The second type of removablepartial denture is all acrylic resin prosthesis, which is alsoknown as temporary, interim removable partial denture or a‘’FLIPPER’’. It acts as a space maintainer and is usually usedto restore the function during the treatment until the definitiveprosthesis is fabricated.Flexible denture material is available in the form of granules incartridges of varying sizes. It was first introduced by the nameof valplast and flexiplast to dentistry in 1956. These aresuperpolyamides which belong to nylon family. Nylon is aresin derived from dicarboxylic acid, diamine, amino acid andlactams. Injection-molding technique is used for fabrication offlexible denture base prosthesis. The prosthesis fabricated fromthese materials requires minimum /no mouth preparation, itprovides a good retention, it is comfortable for patient (thin andlightweight), it is resistant to fractures and is aesthetically goodbecause translucent and pink shade matches that of naturaltissues. Acrylic resin teeth do not bond chemically with flexibledenture base resin. They are mechanically retained by makingT shaped holes into which denture base resin flows to retainteeth mechanically.The clasps of flexible removable partial dentures are extensionsof denture base into undercut areas, which can be adjusted bydipping the clasp area in boiling water and then bending withthe plier in or out to increase or decrease the retention. Flexibleprosthesis is difficult to reline and rebase with soft tissuedenture liners, acrylic resin and even with the other flexibledenture base materials. It is difficult to repair and is prone tostaining by various ingredients of food, tea and coffee if it isnot polished properly and cleaned by the patient regularly. Thepatient should be instructed to practice good oral hygiene andclean prosthesis regularly after every meal, in order to maintainappearance and cleanliness of the prosthesis. The prosthesisshould be removed during the brushing of the natural teeth, to
International Journal of Recent Advances in Multidisciplinary Researchavoid the scratching of the prosthesis (Naylor et al., 1983;Antonelli and Hottel, 2001 and Lowe, 2004).ConclusionThe fabrication of the optimum restoration is depending on theclinicians skills in selection of the type of the restorationswhich is required for the patient. The fabrication of prosthesisfor the partially edentulous arches encountered a specialchallenge where many interferences, various path ofplacement, tilted teeth and deranged occlusion will complicatethe treatment plan. Flexible partial dentures can be a goodoption for the replacement of missing teeth when patient isconcerned about aesthetics. Flexible dentures will stand in asuperior position in fulfilling the various patients demand formore retentive and aesthetic treatment needs, but the propercare of prosthesis is required, in order to minimize the stainingof the prosthesis, which otherwise affects the aesthetics of theprosthesis later on. Flexible dentures were previously selectedby few patients and the clinician but now a days it has becomean elective treatment option.REFERENCES0186Keenan, P.L., Radford, D.R. and Clark, R.K. 2003.Dimensional change in complete dentures fabricated byinjection molding and microwave processing. J. Prosthet.Dent., Jan; 89(1):37-4.Lowe, L.G. 2004. Flexible denture flanges for patientsexhibiting undercut tuberosities and reduced width of thebuccal vestibule: a clinical report. J. Prosthet Dent., Aug;92(2):12831.Maurice, N., Stern, 1964. Valplast flexible partial dentures.New York State Journal. Feb. 30: 123 -36.Naylor, W.P. and Manor, R.C. 1983. Fabrication of a flexibleprosthesis for the edentulous scleroderma patient withmicrostomia. J. Prosthet Dent., Oct; 50(4):536-8.Parvizi, A. et al. 2004. Comparison of dimensional accuracy ofinjection-molded denture base materials to that ofconventional pressure-pack acrylic resin. J. Prosthodont.,13:83-9Stafford, G.D., Hugget, T.R., Macgrego, R.A.R. and Graham,J. 1986. The use of nylon as denture base material. Journalof Dentistry, 14: 18–22.Yunus, N., Rashid, A.A., Azmi, L.L. and Abu Hassan, M.I.2005. Some flexural. Properties of a nylon denture basepolymer. J Oral Rehabil, 32:65-71.Antonelli, J.R. and Hottel, T.L 2001. The "flexible augmentedflange technique" for fabricating complete denture recordbases. Quintessence Int. May; 32(5):361-4.*******
Figure 5. Fabrication of sunflex partial denture Maxillary anterior missing teeth were restored with flexible partial dentures Fig. 4.5.6. And he was very much satisfied with aesthetics as well as with function of the prosthesis. Figure 6. Insertion of flexible partial denture-frontal view Figure 7. Kenne