Transcription
MSK ts4th Quarter 2019A Journey ofTechnologicalEvolutionin Researchand Diagnostics
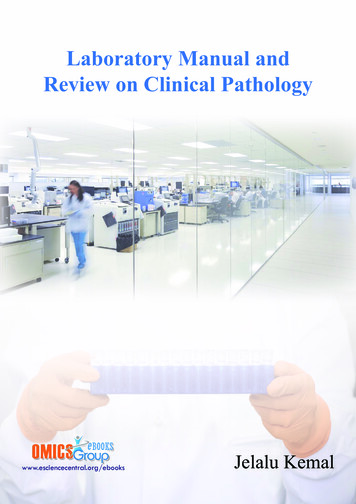
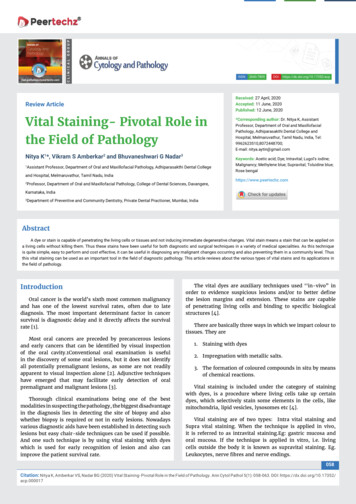
Commentary from the Department ChairCase of the QuarterCASE HISTORYWith this issue of the MSK Pathology Review,we resume the publication of our departmentalquarterly newsletter after a 6 month hiatus. The lackof intervening issues has a simple explanation. Ourtalented science writer, Hope Cristol, decided to moveon to new opportunities, and it took us quite sometime to find a replacement. Finally, we were fortunateto find Onward Publishing, Inc., a professionalwriting group that has assigned several differentwriters to assist us with our production. Meanwhile,Sarah Virgo has continued to collect material andideas for stories. The current issue is among ourmost comprehensive to date, including updates onevents over the past 6 months along with continuingour series on diagnostic teams, individual facultyinvestigators, and fellows’milestones. We introduce a“Case of the Quarter” feature and highlight the qualityimprovement efforts throughout the department.Clearly, the MSK Pathology Review is back on track,and the continuing accomplishments and innovationsfrom our department ensure we will have plentifulmaterial for many issues to come! I would like to takethis opportunity to acknowledge those who havecontributed so much to this project – Hope Cristol,Allix Mazzella, Jordana Shapiro, and of course SarahVirgo, whose investment in this effort is absolutely keyto its success. I hope you will all enjoy this new edition!59 year old woman with palpableand tender 3.5 cm right lateral breastmass and weight loss and no axillarylymphadenopathy. Of note, shepresented with a 1.6 cm right upperlobe lung mass. Both biopsies areshown here. The patient ultimatelyunderwent mastectomy due to rapidgrowth of the breast mass.Breast, biopsyThe correct diagnosis will beprovided in the next issue of the MSKPathology Review and on Twitter at@MSKPathologyScan the QR code to view digital slidesavailable on mskcc.pathpresenter.comLung, biopsyBreast, excision (10x)- David Klimstra, MDBreast, excision (100x)2MSK PATHOLOGYREVIEW4th Quarter 2019MSK PATHOLOGYREVIEW 4th Quarter 20193
Research ProfileWENBINXIAO, MDThe current World Health Organization“(WHO) classification is ‘mostly based onmorphology and history, and integratessome genetic data. For nearly half of theAML, the genetic information is still notutilized to classify disease.’”For a relatively newhematopathologist, Dr. Xiaoalready has remarkableresearch experience.By Hope Cristol4MSK PATHOLOGYREVIEW4th Quarter 2019Some MSK pathologists prefer the clinicalside of their responsibilities; others areprimarily researchers. HematopathologistWenbin Xiao prefers both. Instead of splittinghis time evenly between them, his career hasfocused primarily on either one or the otherat different times.After completing his MD/PhD training,Xiao spent six years doing bench work, firstas a postdoc and then as a research scientist.“At that time, my research was mostly focusedon signal transduction in leukemic cells,” Xiaosays. “But I was trained as a physician, so Iwanted to get involved in patient care as well.”He returned to medicine, completing hisresidency and fellowship and then joined thestaff at MSK. For a while, much of his workwas on the clinical side of pathology. But hisstrong research interest kept tugging at himand soon he was back at the bench.STUDIES ON AMLFor the past three years, Xiao has beenworking to better classify hematologicalmalignancies at the genetic level – especiallysecondary acute myeloid leukemia (AML).He cowrote a seminal review of the geneticbasis of hematologic malignancies, publishedin Blood. The current World HealthOrganization (WHO) classification is “mostlybased on morphology, history, and integratessome genetic data. For nearly half of the AML,the genetic information is still not utilized toclassify disease”, Xiao says.Several of his recently published studiesexplored the genetic underpinnings of raresubclasses of AML. Among the subclasses,core-binding factor AML tends to havea good prognosis. However, it can turninto aggressive disease if it gains genomicmutations over time. Xiao was the leadauthor of a 2017 study, published in BloodAdvances, in which a patient with inv(16)AML achieved five complete remissionswith various chemotherapies but ultimatelydied from this aggressive and highly invasivedisease. Bone marrow biopsies performedat each relapse revealed a consistent gain incytogenetic abnormalities and a KRASG12Dmutation. Although unusual, this uniquecase highlights how acquired genomicalterations can quickly alter prognosis, evenfor a chemosensitive patient.Another study, published in Leukemiain 2018, focused on an extremely rare andaggressive subclass: acute leukemia withmegakaryocytic and erythroid differentiation(ALMED).Previous research in mice suggested acooperative role of JAK/MAP kinase pathwayactivation and TP53 mutations in thepathogenesis of ALMED. Xiao and colleagueswere the first to explore the disease’smechanisms of pathogenesis in humans andconcluded that the mechanism of pathogenesisin humans is similar to that in animals.His recent work also identified PHF6 andDNMT3A mutations in mixed phenotypeacute leukemia, a rare type of leukemiaoften challenging to diagnose. The findings,published in Blood Advances in 2019, showeda phenotype-genotype correlation betweenmutations and mixed phenotype, which canpotentially facilitate the diagnosis.More recently, Xiao reported at the ASHmeeting a subset of AML patients showingRUNX1 mutations and plasmacytoiddendritic cell differentiation, a rare cell typenormally responsible for host immunityagainst viral infection. Accurate diagnosisof this AML variant may benefit the patientsfrom appropriate targeted therapies.EVOLVING RESEARCH ROLEXiao continues to focus on secondaryAML and is adding to the evidence onmutations including PHF6 and RUNX1. “Themutations of these two molecules probablycomprise about 60% of secondary AMLcases,” he says.Xiao’s studies have relied on clinicaldata. However, he has recently moved backto the bench, joining the lab of Ross Levine,MD, the Laurence Joseph Dineen Chair inLeukemia Research and Chief of MolecularCancer Medicine with the Human Oncologyand Pathogenesis Program (HOPP). “I willapply my findings from the clinical side anduse this knowledge to make mouse models tolearn about the mechanisms of the disease,”Xiao says.Treatments for secondary AML are notadequate and disease prognosis is poor. Thisis partly because molecular targets have notyet been identified. Also, the disease usuallystrikes people later in life who “cannottolerate regular cytotoxic chemotherapy.The patient could die from complications,”Xiao says. “So we need to find better targetedtherapy, which means we need to find thosetargets.”MSK PATHOLOGYREVIEW 4th Quarter 20195
THE FOURTH ANNUALSYMPOSIUMIN TRANSLATIONALRESEARCH IN PATHOLOGYHonors William L. Gerard AwardWinner and Highlights Cutting-EdgePathology ResearchBy Julie GrishamOn March 28, Memorial Sloan Kettering’s Department ofPathology hosted its Fourth Annual Symposium in TranslationalResearch in Pathology. The event, which included the presentationof the William L. Gerald Award, was held in the Zuckerman ResearchLaboratory Auditorium.The winner of this year’s Gerald Award was Kojo ElenitobaJohnson, the Peter C. Nowell MD Professor at the Perelman Schoolof Medicine at University of Pennsylvania. Dr. Elenitoba-Johnson is aninternational leader in the fields of hematopathology, molecular andgenomic pathology, and mass spectrometry-driven proteomics. Hegave a lecture entitled “Mass Spectrometry as a Driver for Discoveryin Lymphoma Pathogenesis.”Dr. Elenitoba-Johnson is also the founding director of PennMedicine’s Center for Personalized Diagnostics and chief of theDivision of Molecular and Genomic Pathology at Penn Medicine.Attendees were welcomed to the symposium by Dr. David Klimstra,Chair of the Department of Pathology. Several other pathologists fromthe department gave presentations on a range of topics, includingsample preparation, the role of fusion genes, and assessing minimalresidual disease (see page 9 for a full lecture schedule).The Gerald Award was created to recognize the contributionsand values brought to MSK’s Department of Pathology by William L.Gerald, who died in 2008. Dr. Gerald was a pioneer in the molecularcharacterization of cancer at a time when now-commonplacemolecular techniques were still cutting-edge technology. Throughouthis career, he provided mentorship and collaboration to numeroustrainees and colleagues. The award is a tribute to his scientificcontributions and personal attributes and to the legacy of his workin the department.Past recipients of the Gerald Award include Drs. Arul Chinnaiyanof the University of Michigan Medical School, David Huntsman of theUniversity of British Columbia, Adrienne Flanagan of the UniversityCollege London Cancer Institute, and A. John Iafrate of MassachusettsGeneral Hospital and Harvard Medical School.William L. Gerald, MD PhD6MSK PATHOLOGYREVIEW4th Quarter 2019MSK PATHOLOGYREVIEW 4th Quarter 20197
KOJO ELENITOBA-JOHNSON, MDProfessor, Perelman School of Medicine at the University of Pennsylvania,Founding Director, Penn Medicine’s Center for Personalized Diagnostics,Chief, Division of Molecular and Genomic Pathology, University of Pennsylvania,Penn Medicine’s Center for Personalized DiagnosticsBy Ahmet Dogan, MD, PhDKojo Elenitoba-Johnson is the inauguralPeter C. Nowell, MD Professor at thePerelman School of Medicine at Universityof Pennsylvania. He is also the foundingdirector of Penn Medicine’s Center forPersonalized Diagnostics, as well as thechief of the division of molecular andgenomic pathology. Dr. Elenitoba-Johnsonis an international leader in the fields ofhematopathology, molecular and genomicpathology, and mass spectrometry-drivenproteomics.8MSK PATHOLOGYREVIEW4th Quarter 2019Dr. Elenitoba-Johnson earned hismedical degree from the College of Medicineat the University of Lagos. He completed hisresidency in anatomic and clinical pathologyat the Brown University School of Medicine,where he served as Chief Resident. He thenmoved on to the National Cancer Institute tocomplete a fellowship in hematopathology,as well as to the Leadership Developmentfor Physicians in Academic HealthCenters program at the Harvard Schoolof Public Health. Before arriving at Penn,Dr. Elenitoba-Johnson was the HenryClay Bryant Professor at the Universityof Michigan and served as director of theMolecular Diagnostics Laboratory there.His research focuses on the pathogenesisof human malignant lymphomas, biomarkerdiscovery by genomic and proteomicprofiling, and cancer. Dr. Elenitoba-Johnsonhas been recognized with numerousawards, including the American Society forInvestigative Pathology Scholarship in 1993,the Outstanding Graduating Resident Awardfrom Brown University in 1995, the Societyfor Hematopathology Pathologistin-Training Award in 1998,Outstanding Teaching Awardsin Anatomic Pathology fromthe University of Utah (1999and 2003), and the Ramzi S.Cotran Young InvestigatorAward from the UnitedStates and CanadianAcademy of Pathologyin 2006. He is an elected member of theAmerican Society for Clinical Investigationand is the recipient of the 2012 OutstandingInvestigator Award from the AmericanSociety for Investigative Pathology.Dr. Elenitoba-Johnson is a member ofthe Board of Scientific Counselors for theNational Cancer Institute in the NationalInstitutes of Health. He is an associateeditor for the Journal of Hematopathologyand a member of numerous professionalsocieties, including the American Societyof Hematology, American Society forInvestigative Pathology, United Statesand Canadian Academy of Pathologists,and Association for Molecular Pathology(AMP). He served as the Chair of theHematopathology Division of the AMPfrom 2008 to 2009. He has authored or coauthored more than 170 peer-reviewedresearch publications and has contributedmore than 40 chapters to professionaltextbooks on pathology.Research PresentationsSelected Fellows and FacultyModerators: Drs. Hameed, Reis-Filho and A. DoganComprehensive Solid Tumor Microbiome ProfilingVia Analysis of Unmapped Reads in Large Panel,Hybridization Capture-Based NGS Assay DataDr. Chad VanderbiltDeveloping a Robust Sample Preparation Procedurefor Deep Fourier-Transform Mass SpectrometricProfiling of Formalin-Fixed Paraffin-EmbeddedClinical Tissue SpecimensDr. Michael RoehrlRecurrent but Not Pathognomonic Fusion Genes inMucinous Carcinomas of the BreastDr. Fresia ParejaGenomic Profiling of Mucinous AdenocarcinomaCan Assist in Determination of Site of OriginDr. Amir BoroujeniGLI1-Amplified Soft Tissue Neoplasm: A NovelEntity Showing Morphologic Overlap with Tumorswith GLI1 Gene FusionsDr. Narsi AgaramDetailed Morphologic and Genetic Features ofUrothelial Carcinoma in Patients with LynchSyndromeDr. Hikmat Al-AhmadieEvolving Landscape of Minimal Residual DiseaseAssessment in Hematological MalignanciesDr. Mikhail RoshalModalities and Applications for QuantitativeMultiplexed Immunostaining in Immuno-OncologyDr. Travis HollmannIntroduction, Gerald Award Presentation & SpecialLecture Mass Spectrometry as a Driver forDiscovery in Lymphoma PathogenesissDr. Kojo Elenitoba-JohnsonThe Fifth Annual Symposiumin Translational Research inPathology will take place onThursday, March 26, 2020. Dr.Sunil Lakhani of the Universityof Queensland will receive theWilliam L. Gerald Award.For additional information orto register for the course,please visit:www.mskcc.org/trs2020MSK PATHOLOGYREVIEW 4th Quarter 20199
Research Profilea microscope,” says Dr. Berger. “But the geneticanalysis that we perform can tell us about certaingenomic alterations that are characteristic ofcertain tumor types, as well as which mutations,amplifications, or rearrangements might betargetable by available drugs. This providescomplementary biological and clinicalinformation that can give a pathologist a betteridea of what type of cancer is there and how aparticular patient might respond to a particulartherapy.”Dr. Berger and his team spent yearsdeveloping, refining, and clinically validatingMSK-IMPACT , carefully selecting what genesto include in the test panel, coming up witheffective strategies to deal with lower-qualitytumor specimens, and creating a bioinformaticsplatform to provide doctors with meaningful,actionable results. “The test reaffirms theimportance of pathology not only to correctlydiagnose a patient’s cancer but to provide asmuch information as possible to oncologistsso they can improve the quality of care they aregiving each patient,” says Dr. Berger.MICHAELBERGER, PHDEXPANDING IMPACTOne of the most valuable aspects of the MSKIMPACT program is the size of the dataset thepathology department has now accumulated. Atlast count, more than 200 scientific papers havebeen published incorporating MSK-IMPACT data. “We are sharing this dataset in real timewith all of the investigators at MSK,” says Dr.Berger. “It opens up a whole new set of researchopportunities, both within pathology and inother departments. It is remarkable how thesedata continue to provide new insights into howcancer can and will be treated in the future.”In addition, Dr. Berger’s laboratory isworking to expand pathology’s genomicMichael Berger, PhD,Makes an IMPACTBy Kayt Sukel10MSK PATHOLOGYREVIEW4th Quarter 2019When Michael Berger, PhD, nowAssociate Director of the Marie-Joséeand Henry R. Kravis Center for MolecularOncology at Memorial Sloan KetteringCancer Center, joined MSK in 2010 he hadnever worked directly with pathologists.That said, he hoped to find new ways to applyhis training in genomics and computationalbiology to improve diagnosis and treatmentselection at one of the nation’s foremostcancer centers. At the time, work in cancergenomics was still largely confined to theresearch lab and it wasn’t fully clear how itmight move from the bench to the bedside.“In hindsight, it was fortunate timing,”he says. “Leading cancer centers likeMSK were trying to determine how bestto incorporate genomic technologies andanalysis into clinical care, which was exactlywhat I was excited to do. I’ve come to realizethat pathology really is at the center of ourclinical genomics efforts, offering new waysto diagnose different cancers as well as helpofferings. Since receiving New York StateDepartment of Health approval to use MSKIMPACT as a clinical test in 2014, Dr. Bergerhas made continual improvements, addingadditional analyses and the ability to sequencenew types of biological specimens in order toexpand the test’s clinical utility and its suitabilityfor additional populations of patients.“Originally, the test was used on patientswith advanced cancer who are treated by medicaloncologists and are candidates for clinical trials,”he says. “But we want to expand our program toalso test patients with earlier stage disease whoare typically treated by surgeons. In doing so, wemay be able to identify prognostic biomarkersthat could affect how aggressively patientsshould be treated or monitored for diseaserecurrence.”He and his team have also developeda complementary sequencing test calledMSK-ACCESS, or Analysis of CirculatingCell Free DNA to Evaluate Somatic Status.Sometimes referred to as a “liquid biopsy,” thisoffers clinicians a way to screen for cancer ormetastasis from a simple blood sample withoutthe need for an invasive tumor biopsy. It wasapproved for clinical use by the New York StateDepartment of Health in the summer of 2019.“The opportunity to sequence DNA froma blood sample to detect mutations is veryexciting,” says Dr. Berger. “It allows us the abilityto profile tumor DNA levels longitudinallythroughout a patient’s treatment course, evenin patients from whom we cannot obtain tumortissue. It’s exciting and continues to show howgenomics can help inform clinical treatmentdecisions to provide better outcomes for ourpatients. At the end of the day, that’s whateveryone here at MSK wants.”The test reaffirms“the importance ofpathology not onlyto correctly diagnosea patient’s cancerbut to provide asmuch informationas possible tooncologists so theycan improve thequality of care theyare giving eachpatient.”guide treatment decisions by identifying thegenetic pathways that may be dysregulatedin individual patients’ tumors.”HONING GENOME SEQUENCINGIn the years since, Dr. Berger hasworked closely with his colleagues in theDepartment of Pathology’s MolecularDiagnostics Service to develop agroundbreaking genome-sequencing testcalled MSK-IMPACT , which stands forIntegrated Mutation Profiling of ActionableCancer Targets. This unique, comprehensivetest can detect specific mutations inhundreds of genes, as well as alterations ingenetic pathways in both rare and commonforms of solid cancer tumors. With the MSKIMPACT results in hand, clinicians havetargeted information to guide them as theymatch patients to a specific therapy or to aclinical trial that may benefit them.“Typically, pathologists render adiagnosis based on looking at tissue underMSK PATHOLOGYREVIEW 4th Quarter 201911
A Journey ofTechnologicalEvolutionin Researchand DiagnosticsMSK Pathology Chairman David Klimstra, MD, shares his visionfor the future in his prestigious Maude Abbott Lecture at the 2019USCAP annual meetingBy Kayt SukelWhen David Klimstra, MD, Memorial Sloan Kettering CancerCenter’s Pathology Chairman and James Ewing Alumni Chair,received word that he had been selected to give the 2019 MaudeAbbott Lecture at the annual United States and Canadian Academyof Pathology (USCAP) meeting, his first reaction was disbelief.Since 1980, the Maude Abbott Lecture, named for the pioneeringCanadian pathologist who co-founded the International Association12MSK PATHOLOGYREVIEW4th Quarter 2019of Medical Museums (later known as the International Academy ofPathology), has been one of the greatest honors that can be conferredby the USCAP. Each year, USCAP’s executive committee puts forthfor consideration three candidates, “revered authorities” whohave contributed and continue to contribute to the advancementof pathology. Dr. Klimstra says his selection came out of the “clearblue sky.”His next reaction was anxiety at the prospect of delivering themeeting’s highly anticipated keynote lecture. “I had no inkling I hadeven been nominated. And then to be asked to give what is supposedto be the key lecture of my career — well, it was a little nerve-racking.This isn’t your standard talk where you report on specific researchfindings or give some type of didactic lecture,” says Dr. Klimstra.“In this lecture, you need to reflect on where pathology’s been andthen offer more philosophical thoughts on where it is heading in thefuture — and you give it in front of thousands of your peers. I was veryhonored. But I also knew I had a lot of work to do to get that type oftalk ready.”A LONG AND PRESTIGIOUS CAREEROf course, Dr. Klimstra is no stranger to hard work. Twenty-eightyears ago, after completing his anatomic pathology residency at YaleUniversity, he followed his mentor, Juan Rosai, MD, to MSKCC tocomplete an oncologic surgical pathology fellowship. He’s been withthe department ever since.“At the time, there were about 18 pathologists on the faculty, andnow we are one of the largest cancer pathology departments in theworld,” he says. “Back then, almost all of those faculty were diagnosticpathologists who practiced general cancer pathology. The samepathologists were signing out the skin biopsies, the bone marrowbiopsies, the breast biopsies, the colon resections — you name it.It was a broad general practice. But now we have become very subspecialized with most of our now 100 faculty members focused on aspecific niche, which gives us world-renowned diagnostic expertisein literally every different area of cancer pathology.”Dr. Klimstra first became interested in pathology while studyingat Yale. Like most who pursue a career in medicine, he was drivenlargely by a desire to help people. But when his pathology coursesfirst placed him in front of a microscope, he was immediately hooked.“I’ve always loved science,” he says. “But, in medical school, Ibecame really interested in understanding disease at the morphologiclevel. If I can see it under a microscope, it somehow just makes moresense to me. I really appreciate the more mechanistic aspects of how acancer develops and progresses and the ability to put all those piecestogether in a logical pattern to understand a disease.”Over the course of his career, Dr. Klimstra has put his microscopeto good use by working to better understand the pathology of tumorsof the digestive system, pancreas, liver, and neuroendocrine system.Today, he is an internationally recognized expert on the correlationsbetween the clinical, morphological, immunohistochemical, andmolecular features of both common and rare tumors that developin those areas.When asked why he gravitated toward these forms of cancerseven as early as his residency, he recounts an interesting case heencountered as a resident. That case, a pancreatic acinar cellcarcinoma, led to his first major publication. He realized that veryfew American pathologists were studying pancreatic neoplasia atthat time, and upon moving to MSKCC in 1991, it was clear there was atremendous opportunity in pancreatic pathology. It was a challengingtopic, given the aggressive behavior of most pancreas cancers, butit was also one with the potential to make a major difference incancer care. Even now, he notes, few pathologists have establishedthemselves in this discipline.MSK PATHOLOGYREVIEW 4th Quarter 201913
A WAY FORWARD FOR PANCREATICCANCERPancreatic ductal adenocarcinoma, the mostcommon type of pancreatic cancer, is an insidious andparticularly lethal form of the disease, explains Dr.Klimstra. “Its five-year survival rates are in the singledigits for the average patient. So, anything we can doto detect it earlier, even before it is radiographicallyevident, creates a greater opportunity to cure it. One ofmy interests has been in characterizing the precursorsof pancreatic cancer so we can intervene before invasivecancer develops.”And based on our current knowledge, pancreaticcancer is proving to be more heterogeneous than wefirst believed, which is another reason Dr. Klimstrafeels it’s so important that more people investigate howit develops and progresses. “There are probably fifteendifferent kinds of pancreatic cancer and each has veryspecific attributes,” he said. “But if we can understandhow the distinctive clinical, histological, and molecularfeatures fit together to result in disease, we have thebest chance to define treatments to help our patients.”To date, Dr. Klimstra has published more than400 peer-reviewed articles on tumors of the pancreas,and other organs, and co-authored four ArmedForces Institute of Pathology books, two editionseach of Tumors of the Pancreas and Tumors of theGallbladder, Extrahepatic Bile Ducts and Ampulla ofVater. He has also worked closely with the World HealthOrganization (WHO) and American Joint Commissionon Cancer (AJCC) to develop appropriate classificationand staging systems for tumors of the digestive systemand endocrine organs to aid in detection and treatmentof these conditions.In his Maude Abbott lecture, Dr. Klimstradiscussed the breadth of his research, startingin residency and continuing even now into hisDavid S. Klimstra, MD and Wendy L. Frankel, MDchairmanship, including his work to better understandless common forms of pancreatic cancer, acinar cellcarcinoma (ACC) and pancreatic neuroendocrine tumor (PanNET).progress rather slowly as compared to conventional pancreaticACC makes up only about two percent of tumors that develop in thecancer, sometimes evolving over years or even decades,” he says.organ, but Dr. Klimstra says that even work on a rare disease like ACC“It’s a different type of tumor system and has different types of genetichighlights how pathology investigations have evolved over the lastaberrations that require a different kind of medical management. So,few decades and provides valuable insights that can be generalizedwe’ve been working hard to characterize what features will predict theto more common cancer types.biology of these tumors. How can you tell whether they will be more orThe theme of the lecture was the evolution of technology availableless aggressive? How do we identify which patients need immediateto pathologists to study neoplastic disease. “We started by studyingtreatment as opposed to those who just need to be observed?”the conventional pathology. How do you make the diagnosis? How doThat work, he says, has led to a new way of thinking about not onlythe tumors stain using immunohistochemistry? What happens to thepancreatic neuroendocrine tumors, but neuroendocrine tumors thatpatients over time?” he explains. “But, over the years, with the availabilityarise in other parts of the body.of conventional and then next-generation genomic sequencing, we’ve“Ultimately, the goal of pathology isn’t just to understand thediscovered more and more molecular events that contribute to thedisease process, but to use those insights to make sure our patientsdevelopment of ACC, including some potentially targetable molecularare getting the best possible treatments.”alternations that may allow us to treat patients specifically for thisdisease. We can learn a lot from unraveling the biology of tumors likeTOWARD THE FUTURE OF PATHOLOGYthis.” Data from newer technologies have enabled us to paint a muchDr. Klimstra says that advances in genomic techniques and othermore complete picture of this and other rare neoplasms.technologies are now providing pathologists with a remarkableDr. Klimstra’s lecture also touched on his work investigatingamount of new information. “Ten years ago, the primary role of thePanNETs. Though not as rare as ACCs, PanNETs have a compellingpathologist was to make the diagnosis and then provide any additionalbiology of their own. “Pancreatic neuroendocrine tumors tend toinformation that might help with prognosis,” he explains. “By and large,14MSK PATHOLOGYREVIEW4th Quarter 2019Here at MSK, we“are sitting at thecutting edge of cancerpathology. What weare learning is notonly shaping our owndiscipline but alsocancer care at a globallevel. Working in thisfield has been andcontinues to be anenormous privilege. I’mreally very lucky.”From left to right: Drs. Marcia Edelweiss, Gloria Young, Laura Tang,David S. Klimstra, Olca Basturk and Hui Chenthat was done using traditional morphologic techniques. But as geneticsequencing technology has evolved and become more affordable, we arenow generating enormous amounts of information about mutationsand other genetic alterations that may provide additional insights intohow to best diagnose and treat these cancers.”In addition to generating data on the alterations in tumor DNA,we are now analyzing gene expression, epigenetic alterations suchas methylation, and protein profiles using mass spectrometry. Thesestudies are generating an unprecedented amount of data that canhelp us better understand cancer biology. But only if they can makesense of all that data. That’s why, as Dr. Klimstra noted in his MaudeAbbott lecture, one of the greatest challenges facing pathology inthe future is how to integrate and interpret these vast amounts ofcomplex data.“To a certain extent, we are starting to do this today,” he says. “Butwe aren’t integrating all this information as well as we could be. Thefuture will require us to develop better methods for data integration,including the possibility of using machine learning and artificialintelligence to augment our abilities. We also need to consider ways topotentially automate some of that integration as well so we can makeour practice more efficient.”He adds that, with big data analytics
Pathology Review and on Twitter at @MSKPathology Scan the QR code to view digital slides available on mskcc.pathpresenter.com Case of the Quarter Breast, biopsy Lung, biopsy Breast, excision (10x) Breast, excision (100x) With this issue of the MSK Pathology Review, we resume the publicati