Transcription
MSK TS2ND QUARTER2017
TABLE OFCONTENTS1LETTER FROM THE DEPARTMENT CHAIRMAN2MSK-IMPACT LEADS THE WAY IN TUMOR SEQUENCING EFFORTS4DECODING THE GENETICS OF GYNECOLOGICAL CANCERS6MEDICAL DONATION PROGRAM ADVANCES THE STUDY OF METASTASIS6Q & A WITH CHRISTINE ENGLAND8THE 2016 FRED W. STEWART AWARDEE RALPH HRUBAN, MD10MSK’S GENITOURINARY PATHOLOGY TEAM11PATHOLOGY AT MSK INFO-GRAPHIC12HEMATOPATHOLOGY SERVICE ADDRESSES GROWING NEEDS AT MSK142016-2017 USCAP PATHOLOGY PRESENTATIONS18FELLOWS' FEATURE192016-2017 CLINICAL FELLOWS20 PROMOTIONS20 MDS WHO TWEETCover photo from left to right- Oscar, Lin, MD, PhD, Chief, Cytology Service, Ahmet Dogan, MD, PhD, Chief,Hematopathology Service, Jorge S. Reis- Filho, MD, PhD, FRCPath, Chief, Experimental Pathology Service,David Klimstra, MD, Chair, Department of Pathology, Marc Ladanyi, MD, Chief, Molecular Diagnostic Service,Meera Hameed, MD, Chief, Surgical Pathology Service, Victor Reuter, MD, Vice Chair, Department of Pathology
LETTER FROM THEDEPARTMENT CHAIRMAN"With this inaugural issue of the MSK Pathology Review, we launch a new periodical designed toprovide members of the department, alumni, and others in our academic community a snapshotof the activities ongoing in our department. The past decade has seen substantial growth inpathology – not only in the volume of specimens being reviewed and the corresponding staffrequired to diagnose them but also in the breadth of diagnostic and research activities. The adventof superspecialization more than 10 years ago required significant expansion of the diagnosticpathology faculty. Together with the Department of Laboratory Medicine, we created a new clinicalservice in hematopathology. The Molecular Diagnostics Service has grown exponentially in recentyears as the emphasis has shifted from supporting anatomic diagnosis to identifying therapeutictargets, and the technology at hand to allow systematic and deep molecular characterizationof tumors has become accessible for routine clinical use. An infusion of energy into novelresearch arenas has accompanied the growth in diagnostics. As a result, we have developednew disciplines within pathology, such as clinical bioinformatics, the research autopsy program,precision biobanking, digital and computational pathology, advanced immunomorphology, andproteomics, as well as growth and reorganization of the Experimental Pathology Division. I hopethat the information and vignettes contained in this publication will help keep us abreast of thesemany developments, and we will select a few specific topics to be highlighted in each issue. Ourdiscipline continues to evolve, and while we maintain the techniques that have remained thecornerstones of tumor diagnostics for much of our history, we are also excited about the manyopportunities to expand the impact of the diagnostic information we provide. Now more than ever,pathology is at the center of the clinical management of patients with cancer, and our departmentwill continue to lead the way in the development and assessment of novel tools to characterizethis spectrum of human disease and to define the most effective therapies for our patients. "- David S. Klimstra, MDPATHOLOGY REVIEW1
MSK-IMPACT LEADSTHE WAY IN TUMORSEQUENCING EFFORTSTo take advantage of the advances in theunderstanding of cancer genomics — andspecifically the development of targetedtherapies that exploit the molecular mutationsthat drive cancer — it is crucial to have an assaythat can detect these mutations in an accurateand efficient way. This was the impetus behindthe development of MSK-IMPACT, a powerful andever-evolving tool for sequencing patient tumors.Since 2014, pathologists in Memorial SloanKettering’s Molecular Diagnostic Service havebeen using it to analyze the tumors of nearly everyMSK patient diagnosed with an advanced cancer.The test allows doctors to detect mutationsand other genetic changes that can help guidetreatment decisions, including matching patientswith clinical trials for experimental targetedagents.The panel initially investigated 341 mutationsknown to be connected to cancer. It has since2MSKbeen expanded several times and was recentlyupdated from 410 to 468 mutations. “The genesthat we recently added might be the focus of newtrials in a few years,” says Marc Ladanyi, Chief ofMSK’s Molecular Diagnostics Service. “We alreadyhad on the panel all the genes that are targets oftrials today. We’re being forward-looking to tryto anticipate which mutations may be clinicallyessential several years from now.”Another new feature provides informationabout microsatellite instability within tumorcells, which can also guide treatment and aidin prognosis. “It’s a continually evolving andimproving assay that has become the centerpieceof the institution’s precision oncology initiatives,”he adds.MSK-IMPACT relies on next-generationsequencing and an advanced bioinformatics effort.“We have a very sophisticated bioinformaticsanalysis group that processes the data in a
consistent and state-of-the-art fashion,” Dr.Ladanyi says. Pathologists and bioinformaticianstogether review all the mutations that aredetected in individual samples and issue a finalreport.The MSK-IMPACT assay has led to thedevelopment of so-called basket trials — clinicalstudies that assign patients to receive targeteddrugs based on the mutations in their tumorsrather than the organ in which they arose inthe body. It has also led to an improvement indiagnosing cancers that had previously beencancers of unknown primary origin (CUP).Even in cases in which the primary site cannotbe determined, sequencing results can provideguidance on the best course of treatment forpatients with CUP.In early 2016, the Pathology Departmentpassed the milestone of sequencing tumors from10,000 patients. That number continues to growand now stands at more than 8,000.Results from MSK-IMPACT testing not onlyguide patient care, but they also are makingan important impact on research. MSK’s datacontribution to AACR (American Association forCancer Research) Project GENIE — a multicentereffort to aggregate tumor sequencing data andlink it to patients’ medical records — comes fromresults from MSK-IMPACT. Thanks to the assay,MSK leads the collaboration with the largestnumber of patients added to the AACR ProjectGENIE database.MSK-IMPACT was developed in MSK’sDepartment of Pathology. Dr. Ladanyi, along withgenomics researcher Michael Berger, molecularpathologist Maria Arcila and bioinformaticianDonavan Cheng, led the clinical validation andimplementation of the test.As patient tumor sequencing is not yetconsidered standard care, it is seldom covered byprivate insurance of the Centers for Medicare andMedicaid Services. MSK's Marie-Josée and HenryR. Kravis Center for Molecular Oncolongy, whichcoordinates many of MSK's molecular oncologyefforts, provides philanthropic funding to coverthe expenses.- Julie GrishamPATHOLOGY REVIEW3
DECODING THE GENETICS OFGYNECOLOGICAL CANCERSBritta Weigelt leads aresearch team in MemorialSloan Kettering’s Departmentof Pathology and acts as theDirector of the GynecologyResearch Laboratory in theDepartment of Surgery. Herwork focuses on the studyof gynecologic cancers —in particular ovarian andendometrial cancers. Bycombining pathology and stateof-the-art genomics methods,Dr. Weigelt’s team is learningmore about the genetic changesthat bring about these cancersand may lead to more effectivetreatment, especially withtargeted therapies.4MSK“My background was instudying breast cancer, and Iwas surprised when I movedinto the study of gynecologicdiseases how little we knowabout the genetics of thesetumors,” she says. “Our researchenables us to gain a much betterunderstanding of gynecologiccancers.”The laboratory is focused onthree areas of research.The first is to find raresubtypes of gynecologic cancerand to identify their geneticunderpinnings. “We use anumber of different sequencingtechnologies and molecularpathology techniques tounderstand what drives them,”Dr. Weigelt explains. “Much ofwhat we do is whole exomesequencing, and to characterizesome rare types we also dowhole genome sequencing andRNA sequencing, which allowsus to look for fusion genes andsomatic genetic alterationsaffecting regulatory elementsof cancer genes.”Another area of focus for thelab is intratumor heterogeneity.Some gynecologic tumors showmorphologic heterogeneityunder the microscope. Forexample, carcinosarcomas ofthe uterus are part sarcomaand part carcinoma: These
cancer phenotypes reflect twodifferent cell lineages in thebody. “This is a particularlyaggressive type of disease,and although these tumorshave been studied for a while,in the past they were analyzedas a whole,” Dr. Weigelt says.“We’re interested in studyingthe different areas and lookingat their genetic alterations. Wehope to eventually infer whichcame first: Did the carcinomadifferentiate into a sarcoma, orwas it the other way around?And we will compare thesetumors with their counterpartsin other anatomical sites.”The laboratory is alsostudying endometrial cancersthat have two differentmorphologies under themicroscope to determine ifthose differences are based ongenetic variations in the cells.“At this point we’re still learningabout the biology,” Dr. Weigeltexplains. “Understanding thebasis of the phenotypic diversityin these cancers will help usdefine the rules of genetic andphenotypic heterogeneity inendometrial cancers.”The third major area of studyfor the laboratory is the analysisof circulating cell-free DNA thatoriginates from tumors. This lineof work enables investigators tomonitor how cancers develop,change, and become resistantto particular therapies bycollecting a vial of blood ratherthan conducting biopsies, whichare much more invasive.Early efforts in this fieldhave focused on ovarian cancer.“Resistance to chemotherapyis a big problem for ovariancancer,” Dr. Weigelt says. “Manyof these tumors are sensitive tosystemic chemotherapy agentsin the beginning, but at somepoint they become resistant.We’re hoping we can detectresistance earlier by monitoringDNA in the blood, because oftenwhen the disease comes backit’s very hard to treat.”Unlike circulating tumor cells,which are whole cells that breakoff from the tumor and circulatethrough the bloodstream,cell-free DNA is free floating.H o w e v e r,inflammatoryprocesses can also lead to freefloating DNA; thus not all cellfree genetic material comesfrom the tumor. Investigators areable to analyze the DNA to lookfor specific genetic alterationsthat are known to be cancerrelated.Dr. Weigelt’s lab hasrecently demonstrated thepresence of BRCA1 and BRCA2reversion mutations in patientstreated with platinum-basedchemotherapy. These mutationshave been shown to constitutea mechanism of resistanceto agents targeting a type ofDNA repair that is defectivein a substantial proportion ofovarian cancer patients. Herlab is now extending the studyof cell-free DNA to includeendometrial cancers as well.“We know much less about howthis disease progresses than wedo with many other cancers,”she says, “In breast cancer we’veshown that we can monitor apatient’s response to therapyby detecting a drop in thepercentage of the DNA in theblood that has cancer-relatedmutations, and that increasesin the circulating tumor DNAin plasma predict relapses. Wehope to extend this to othercancers as well.”- Julie GrishamPATHOLOGY REVIEW5
MEDICAL DONATIONPROGRAM ADVANCESTHE STUDY OF METASTASISMuch of what we know about cancer geneticstoday comes from the study of patient tumors.But studying the genetics of metastasis has beendifficult because those tumors are usually notremoved or biopsied. Memorial Sloan Kettering’sMedical Donation Program is advancing theunderstanding of the genetics of metastasis bystudying all of patients’ tumors after they die.“There’s a strong gene discovery aspect tothis program,” says Christine Iacobuzio-Donahue,who was recruited to MSK in 2014 to head theprogram. “We sequence the primary tumors aswell as the metastases and compare them. We’vefound a lot of genes that no one has ever foundbefore, and this enables us to look for the cellularpathways that allow cells to metastasize.”Studies based on tissues collected as partof the program are already yielding importantfindings. In pancreatic cancer, which was the initialQ&AWITH CHRISTINE ENGLAND, MBAfocus, the researchers have found that pancreaticcancer does not always metastasize, and thatcomplications from the primary tumor may bethe cause of death. “That was a surprise, becauseit’s not what everybody thought,” Dr. IacobuzioDonahue says. “The thing that correlated with thiswas the genetics of the original tumor.”Specifically, the investigators found that thegene responsible for this behavior was SMAD4.“The mutation is there in the beginning anddrives the whole disease process,” she adds.“This finding is starting to change the paradigmof how patients are treated. Depending on whatpatient’s cancer care team. It is so importantfor our patients to receive a timely, precisediagnosis to ensure they receive an appropriatetreatment plan. At MSK, we are in a uniqueposition to provide the most accurate diagnosisfor our patients through our world-recognizedsubspecialty pathologists and our advanceddiagnostic technologies.Q: What is most exciting about pathology rightnow?Administrator, Department of PathologyI’m so thankful to work at an institution thatfosters innovation and encourages us to alwayslook for ways to do things better. We haveinvested in many new technologies in recentyears and it is exciting to see recent innovationsbeing incorporated into clinical practice, such asdigital pathology, telepathology, and advanceddiagnostic tests.Q: Why is pathology such a vital piece of thecancer treatment process?Q: Why do you enjoy being apart of the MSKCCteam?All of our staff in the Pathology Department areamong the most important members of an MSK6MSKThe people! We have the best staff who trulygo above and beyond every single day. I am
mutations the tumors have, there may be a needfor more intensive local therapy, such as anexpanded role for radiation therapy.”The team has also found that neoplasticchanges may exist in the pancreas for as longas two decades before growing or spreading,offering clues for early diagnosis and screeningof the disease. “This shows us there’s a longwindow for early detection of the disease, and haschanged the view that it can’t be caught in theearly stage,” Dr. Iacobuzio-Donahue says. “Nowwe need to find out the best way to screen for it.”Since it was created, the Medical DonationProgram has expanded to include other types ofcancer, including myeloma, melanoma, and breastcancer. “So far our sample sizes have been verysmall, but we’re already seeing that the geneticpatterns by which these tumors grow, evolve, andspread is very different based on where the tumororiginates,” she explains.One of the major goals of the program is tofind alterations in cellular pathways that could betargeted with drugs. “We’re also looking at thefeatures of the microenvironment in the tumorthat might give the cancer cells the tools tosurvive after they spread to secondary sites inthe body,” she adds.Dr. Iacobuzio-Donahue says that the programcan provide comfort to patients who are dyingof cancer, knowing that they will be able tomake a contribution to the understanding ofthe disease. “It gives them the sense of leavinga legacy and contributing to something biggerthan themselves,” she notes. She adds that theprogram can also provide consolation to familiesof patients. MSK’s pathologists make an effort toshare the results of studies with patients’ familymembers and often receive letters of gratitude.The program does not require that patientsdie at Memorial Hospital. Arrangements can bemade in advance to collect the remains fromhome or a hospice facility. The tissues may beused in Dr. Iacobuzio-Donahue’s own researchor — if patients consent — by investigators inother laboratories at MSK, or even beyond. Pleasecontact Chelsea Michael, Clinical Coordinator atmichaec1@mskcc.org for additional information.motivated to give 110% each day by feeding offthe energy, hard work, and dedication that I seefrom all of our team members.science, I had the incorrect assumption that youhad to become a doctor or a nurse to enter themedical field. One of my goals for 2017 is to workon our outreach and education to high schoolsand colleges to make such bright, young mindsaware of the opportunities that we have in all ofour labs and in hospital administration. I love thatsome of our administrative staff are consideringbeing trained in histology to make the transitionto a laboratory based career by leveraging theresources we have in our department (exceptionalmanagers and mentors) and MSK (tuitionreimbursement).Q: What exactly is an administrator responsiblefor?An administrator is responsible for high levelstrategic planning for the department andpartnering with our chair, Dr. Klimstra, and hospitaladministration to ensure that our departmentmeets overall hospital goals and expectations.It’s my job to argue for and justify any resourcerequests that we need to get our jobs done asefficiently as possible. I also need to be involvedin all areas of our operations and finances froma high level. If we have any turn over in staff, itis my job to step in and step up to ensure ouroperations are continuous and not affected.Q: What advice would you give to a personseeking a career in pathology?There are so many career options in ourdepartment that I had no idea about beforeworking at MSK. As a student interested in- Julie GrishamQ: Why is MSK the place for you?I believe that a job well done does not maintainthe status quo. MSK can sometimes be a toughplace to work but overall the organization is fair,supports its employees, and challenges eachemployee to work at a higher level. I have workedat MSK for 12 years now and I have had five verydifferent job opportunities and never a boringday. I’m grateful to work in place with so manyunique opportunities.PATHOLOGY REVIEW7
THE 2016 FRED W.STEWART AWARDEERALPH HRUBAN, MDDr. Ralph Hruban is therecipient of the 2016 FredWaldorf Stewart Award,bestowed annually by theDepartment of Pathology atMemorial Sloan Kettering CancerCenter on an individual who hasmade outstanding contributionsto our understanding of humanneoplastic disease.Dr. Hruban is a worldrenowned pancreatic cancerpathology expert who hasdevoted his academic careerto the study of pancreaticneoplasms. He has madesignificant contributions toour understanding of all typesof pancreas tumors – ductal,acinar and neuroendocrine.8MSKImportantly, his work on PanINsand IPMNs, the precursorlesions that give rise to invasivepancreas cancer, has had aparticularly significant impactboth in the field of pancreasresearch and with regard to howpatients with this disease areprognosticated and managed.Dr. Hruban obtained hisundergraduate degree fromthe University of Chicago andhis medical degree from theJohns Hopkins University Schoolof Medicine. His pathologytraining consisted of residencyin anatomic pathology at JohnsHopkins and fellowship inoncologic surgical pathologyat Memorial Sloan KetteringCancer Center. In 1990, uponcompletion of his fellowship,Dr. Hruban returned to JohnsHopkins to join the facultyand has remained there eversince. Quickly rising throughthe academic ranks to becomeprofessor of both Pathologyand Oncology, Dr. Hruban hasserved multiple important rolesover the years at Johns Hopkinsand is currently Director of theSol Goldman Pancreas CancerResearch Center, Director of theDivision of Gastrointestinal andLiver Pathology, and Director ofthe Department of Pathology.Dr. Hruban joined the questto conquer pancreas cancerearly on. In the 1990s, at a timewhen the world of biomedicalresearch was in one of its morevisible transformations fromtraditional analyses to newerand more complex technologies,and the focus on the origins ofcancer was converging at themolecular level largely as aconsequence of studies donewith the newer technologies.Young Dr. Hruban and hiscolleagues took to techniquessuch as “mutant-enrichedpolymerase chain reactionanalysis” in combination with“allele-specific oligonucleotidehybridization”, and revealedthat KRAS mutations (nowknown to represent one of thefew big “mountains” in pancreascancer’s genomic landscape)were important events inpancreatic cancer. Dr. Hrubanenvisioned presciently thatspecific molecular alterationsof this type would not onlyallow a better understandingof the genetic drivers forpancreas cancer development,but they would also have thepotential to serve as markersfor the detection of this deadlydisease at an early stage duringwhich intervention might stillsave lives. In the same spirit ofapplying innovative approachesto the study of cancer, and stillin the early 90’s, Dr. Hruban alsoco-founded the National FamilialPancreas Tumor Registry atJohns Hopkins, a patient registrythat would later serve as aninvaluable resource for the studyof pancreas tumors.During the 2 decadesfollowing these initial efforts,Dr. Hruban dove deeperinto the field of pancreasneoplasia and maintained afocus on understanding thenoninvasive precursor lesionsfrom which invasive cancersdevelop (PanINs and IPMNs),the familial aggregation ofsome pancreatic cancers, andthe pathologic ramificationsof genetic alterations in thepancreas. At Hopkins and with
multi-institutional collaborativegroups mostly led by him, Dr.Hruban produced during thistime meritorious scientific workthat served both to advancepancreas cancer research, andto facilitate diagnosis, detection,prevention, prognosis, andtreatment. As a testamentto such achievements, Dr.Hruban has over 700 scientificpapers and is credited by the“Essential Science Indicators”as the most cited pancreascancer scientist in the world(for those who believe in the“H-index”, Dr. Hruban’s H-indexis above 150!). Numerous awardshave been bestowed on him inrecognition of his achievements,including (but far from beinglimited to) the Arthur PurdyStout Prize and the RamziCotran Award from USCAP,the PanCAN Medical VisionaryAward, the Ruth C. BrufskyAward of Excellence in ClinicalResearch for Pancreatic Cancer,and election to the GermanNational Academy of SciencesLeopoldina. Most recently, ridingon the wave of next generationsequencing, Dr. Hruban and agroup of distinguished pancreasscientists including our own Drs.David S. Klimstra and ChristineIacobuzio-Donahue discovereda new cancer pathway and newfamilial pancreatic cancer genes,defined the time course for thedevelopment of pancreaticneoplasia, and showed thateach of the four cystic tumorsof the pancreas has a uniquemutational profile. Once again,these efforts have significantlyimproved our understandingof the fundamental geneticchanges that characterizepancreatic neoplasms, andimportantly, bear immediateclinical implications. It is onlyfitting that Dr. Hruban and hiscolleagues were recognized fortheir efforts as recipients of theprestigious Team Science Awardfrom the American Associationfor Cancer Research.Dr. Hruban is also a superbsurgical pathologist andan ardent educator. He hasdedicated time and effort tothe teaching of pathology,particularly GI and pancreaspathology, to trainees andpracticing pathologists aswell as patients worldwide.He disseminates knowledgethrough lectures, courses,books, and digital media. Dr.Hruban has written more than150 book chapters and reviewsand authored or coauthored6 books, including the AFIPFascicle on Tumors of thePancreas and the World HealthOrganization “blue book” ontumors of the digestive tract.With a deep appreciation ofvisual arts, Dr. Hruban frequentlyutilizes creative images for theteaching of pathology and hasdeveloped unique iPad andiPhone applications that arevaluable resources for medicalprofessionals and patientsalike. An award-winning iPadapplication created by him hastaught pancreas pathology tomany; another patient-orientediPad and iPhone app that hecreated and is free to all hasserved as a valuable educationalguide for patients and caregiversfacing a diagnosis of pancreaticcancer.It should come as nosurprise that Dr. Hruban’sachievements also extend intoother realms. In addition tohis many accomplishmentsin scientific research, patientcare, and medical education,Dr. Hruban has also made hismark in additional fields. Hisinspirational biographies ofinfluential historical figures arebut one example; history buffs– and I am very certain nonhistorian enthusiasts, too – willfind Dr. Hruban’s award-winningdocumentary on WilliamStewart Halsted, M.D. (http://HalstedTheDocumentary.org)and a series of “Osler Minutes”on the philosophy of WilliamOsler, M.D. (http://pathology.jhu.edu /department/ about/history/osler-minutes.cfm) mostenjoyable, and, like his otherscientific works, intriguinglyinsightful.Today, as we celebrate thememory of Dr. Fred WaldorfStewart, a man who madesignificant contributions to thecare of cancer patients throughthe practice of conventionalpathology, it is most fittingthat the medal in his name bebestowed on an individual whoextended Stewart’s traditionthrough innovative integrationof conventional pathologywith cutting-edge molecularand digital technologies. Wecongratulate Dr. Hruban on thiswell-deserved Stewart Award.- Jinru Shia, MDRECENT FRED W. STEWARTAWARD RECIPIENTSJUAN ROSAI, M.D., 2006PETER C. BURGER, M.D., 2007PAUL PETER ROSEN, M.D., 2008ROBERT J. KURMAN, M.D., 2009JULIA A. BRIDGE, M.D., 2010STANLEY R. HAMILTON, M.D., 2011E. LEON BARNES, M.D., 2012RICHARD KEMPSON, M.D., 2013THOMAS M. ULBRIGHT, M.D., 2014ROBERT H. YOUNG, M.D., 2015PATHOLOGY REVIEW9
MSK’SGENITOURINARYPATHOLOGYTEAMThe Genitourinary teamwithinMemorialSloanKettering’s Department ofPathology focuses on a numberof cancers of the genitourinarytract, including those arisingin the prostate, kidney, urinarybladder and testis.Members of this groupexamine thousands of biopsiesand resections from patients’tumors every year in order toestablish the correct diagnosisand determine the extent ofthese tumors. Members ofthe team are also involved inresearch on the molecular andgenetic abnormalities of thesetumors to identify markersthat can help with diagnosisand prognosis and may alsoultimately lead to new treatmentstrategies with targetedtherapies.One particular area of studyis certain rare but aggressivesubtypes of bladder cancer.Pathologist Hikmat Al-Ahmadie10MSKis studying many of thesetumors. “Bladder cancer didn’tget much attention for a longtime, so there haven’t been manyadvances in our understandingof it until very recently,” Dr. AlAhmadie explains. “But in thepast few years, we’ve learned alot about the genetic drivers ofthese cancers.”One type of cancer thatDr. Al-Ahmadie has studiedextensively is plasmacytoidurothelial carcinoma, anaggressive form of bladdercancer that rarely responds tochemotherapy and developsresistance to those drugs evenif it does initially respond.Based on the genomic analysisof patients’ tumor samples, Dr.Al-Ahmadie’s team was able toidentify a unique genetic eventthat is responsible for the vastmajority of these tumors andthereby establish a moleculardefinition for this type of cancer.Specifically, they found that aloss-of-function mutation in theCDH1 gene is pathognomonicfor this subtype.Another area of Dr. AlAhmadie’s work is focusedon exceptional responders(also called extraordinaryresponders). These are patientswhosecancersrespondespecially well to treatment withtargeted therapies even whilethe majority of patients withseemingly similar tumors do notrespond at all. Genomic analysisof tumors from these exceptionalresponders can reveal geneticabnormalities that illustratehow these patients are different.Once these abnormalities areidentified, additional patientswith the same abnormalitiescan be identified for clinicaltrials known as basket trials.This enriches the populationof patients who are most likelyto benefit from a particulartreatment.Dr. Al-Ahmadie is alsostudying the molecular eventsthat lead to heterogeneityin bladder tumors. “Bladdercancer is very heterogeneous,and these varied regions maybe associated with the failure torespond to a particular treatmentor with a worse prognosis,” hesays. “A major part of my workis to identify the molecularbasis for this heterogeneityand to find specific geneticabnormalities that may explainthe morphologic differencesthat are seen in different partsof the tumor.”To do this, his groupp e r fo r m swholeexo m esequencing as well as targetedsequencing in different areas ofthe same tumor. “We are findingthat these different areas haveshared alterations, but eachmorphologically distinct regionalso has its own set of alterations
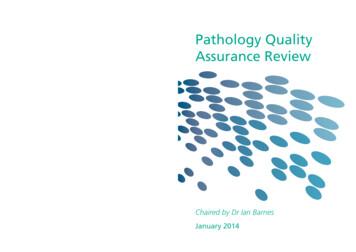
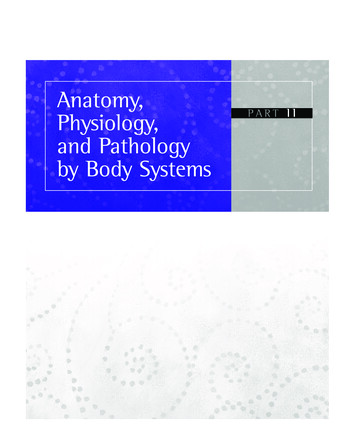
that are different from the otherregions,” he adds.On a wider scale, Dr. AlAhmadie has also been involvedin the bladder cancer studiesthat are part of The CancerGenome Atlas (TCGA), agovernment-funded, multicenterinitiative that collects, processes,and characterizes the largest setof tumor samples to date usingstate-of-the-art genomic andmolecular techniques.Along with members of theBladder Cancer Oncogenometeam, he is also beginning tofocus on the study of cell-freeDNA in patients with bladdercancer.“The immediate effect ofall of these different areas ofresearch is that we can betterunderstand genitourinarycancers,” Dr. Al-Ahmadie says.“In the longer term, we hopeto characterize more molecularchanges that may be targetsfor treatment as well as identifyadditional genetic events thatmay be diagnostically andprognostically important forpatients.”- Julie GrishamPATHOLOGY AT MSKNUMBER OF CASES SEEN IN 2016NUMBER Of 201641,982 Surgical and biopsy cases25,584 Submitted slide cases4,565 Personal consult cases32,530 Cytology cases10,132 Frozen cases8,621 Hematopathology cases41,491 Molecular cases74 ATTENDINGSacross 5 services& 1
pathology is at the center of the clinical management of patients with cancer, and our department will continue to lead the way in the development and assessment of novel tools to characterize this spectrum of human disease and to define the most effective therapies for our patients. "- David S. Klimstr