Transcription
REIMBURSEMENTRESOURCE GUIDEINDICATIONSSOMATULINE DEPOT (lanreotide) Injection is a somatostatin analog indicated for: the long-term treatment of patients with acromegaly who have had an inadequateresponse to surgery and/or radiotherapy, or for whom surgery and/or radiotherapyis not an option; the goal of treatment in acromegaly is to reduce growth hormone(GH) and insulin growth factor-1 (IGF-1) levels to normal; the treatment of adult patients with unresectable, well- or moderatelydifferentiated, locally advanced or metastatic gastroenteropancreaticneuroendocrine tumors (GEP-NETs) to improve progression-free survival; and the treatment of adults with carcinoid syndrome; when used, it reduces thefrequency of short-acting somatostatin analog rescue therapy.Somatuline DepotAcquisitionSomatuline DepotBilling and CodingIPSEN CARES Reimbursementand SupportPlease see accompanying full Prescribing Information and Patient Information.1Hours: 8:00 AM - 8:00 PM ET, Monday - FridayPhone: 1-866-435-5677FAX: 1-888-525-2416www.ipsencares.com
Important NoticeThis guide was developed to provide physician practices and hospital outpatient office staff witha resource guide for Somatuline Depot support offerings and assist in understanding third-partyreimbursement for Somatuline Depot. The guide is not intended to provide recommendationson clinical practice or legal advice. Laws, regulations, and policies concerning reimbursement arecomplex and are updated frequently. Although we have made an effort to be current as of the issuedate of this document, the information may not be current or comprehensive when you view it.This document represents no statement, promise, or guarantee concerning coverage or levels ofreimbursement. Similarly, all International Classification of Diseases, 10th edition; Clinical Modification(ICD-10-CM); Current Procedural Terminology (CPT ); and Health Care Procedure Coding System(HCPCS) codes for Somatuline Depot are supplied for informational purposes. It is always thephysician's or facility's responsibility to determine and submit appropriate codes, charges, andmodifiers for services that are rendered. It is recommended that you contact your local payers withregard to local reimbursement policies and practices. Please consult your counsel or reimbursementspecialist on reimbursement or billing questions specific to your practice.For additional medical information about Somatuline Depot, please call Ipsen Medical Affairs at1-855-463-5127.Please see accompanying full Prescribing Information and Patient Information.2
SOMATULINE DEPOT ACQUISITIONSomatuline cesIf Somatuline Depot Is Covered Under the Medical BenefitPurchase Somatuline DepotDirectly (Buy and Bill)Specialty Pharmacy Assignmentof Benefit (AOB) Requires Doesan upfront financial investment Your office acquires Somatuline Depot directlyfrom a select group of Specialty Distributors Your office collects copay/coinsurance directlyfrom the patient Your office seeks reimbursement from thepatient’s payer(s) It is important to verify with each patient'sinsurance plan to determine if buy and bill isallowednot require an upfront financialinvestment Your office orders Somatuline Depot from aSpecialty Pharmacy for a specific patient Patient pays copay/coinsurance directly toSpecialty Pharmacy Specialty Pharmacy ships product directly toyour office Specialty Pharmacy seeks reimbursement fromthe patient’s payer(s) IPSEN CARES provides helpful information onselecting the appropriate Specialty Pharmacyprovider by calling 1-866-435-5677If Somatuline Depot Is Covered Under the Pharmacy BenefitSpecialty Pharmacy Doesnot require an upfront financial investment Your office orders Somatuline Depot from a Specialty Pharmacy for a specific patient Patient pays copay/coinsurance directly to Specialty Pharmacy Specialty Pharmacy ships product directly to your office Specialty Pharmacy seeks reimbursement from the patient’s payer(s) IPSEN CARES provides helpful information on selecting the appropriate Specialty Pharmacyprovider by calling 1-866-435-5677Please see accompanying full Prescribing Information and Patient Information.3
Authorized Specialty DistributorsSpecialtyDistributorASDHealthcare Besse MedicalCardinalHealthSpecialtyPharmacyCuraScriptSD McKessonSpecialtyHealthOncologySupply /CustomerCenter/MckessonWebStore.html#PRELOGIN ductSomatuline DepotSomatuline DepotOrderTimesMon - Thu:7 am - 6:30 pm ETFri: 7:00 am - 6:00 pm ETMon - Thu:8:30 am - 7:00 pm ETFri: 8:30 am - 5:00 pm ETSat: Delivery Available byPrior ArrangementSomatuline DepotMon - Fri:8:00 am - 7:00 pm ETSomatuline DepotMon - Fri:8:30 am - 7:00 pm ETSomatuline DepotMon - Fri:8:00 am - 8:00 pm ETSomatuline DepotMon - Thu:9:00 am - 8:30 pm ETFri:9:00 am - 8:00 pm ETThe Specialty Distributors listed above are not associated with Ipsen Biopharmaceuticals, Inc. ("Ipsen") nor do theyrepresent Ipsen. These Specialty Distributors have been selected by Ipsen to distribute Somatuline Depot given theirreputation, capabilities, and customer satisfaction ratings. Our goal is to provide you with options to select the SpecialtyDistributors that will meet your needs. You are free to engage any of the above Specialty Distributors. You may also openan account with more than one of the above distributors if you wish.Please see accompanying full Prescribing Information and Patient Information.4
SOMATULINE DEPOT BILLING AND CODINGReimbursement CodingWhen completing the CMS-1500 claim form, the UB-04 claim form, or submitting a prior authorization request forSomatuline Depot, include accurate descriptions of the patient’s diagnosis, route or mode of administration, andthe drug used.Healthcare Common Procedure Coding System (HCPCS) Level II CodeA permanent HCPCS code has been assigned to report use of Somatuline Depot.Somatuline Depot HCPCS CodeDescriptionJ1930Injection, lanreotide, 1 mgNational Drug Codes (NDCs)Drug products are identified and reported using a unique, three-segment number, called the National DrugCode, which is a universal product identifier. The NDC is used primarily for pharmacy claims, but it may berequired also when billing for physician-administered drugs to ensure crosswalk accuracy. When providersare required to include an NDC on an insurance claim, it typically must be in the required 11-digit format.Single-dose Sterile Prefilled SyringeNDC120 mg*15054-1120-0390 mg15054-1090-0360 mg15054-1060-03*GEP-NET and carcinoid syndrome: dosing is 120 mg administered every 4 weeks by deep subcutaneous injection.Acromegaly: the starting dose is 90 mg once every 4 weeks. For patients with moderate or severe renal or hepatic impairment, initial dose is 60 mg once every 4 weeks.Current Procedural Terminology (CPT ) Drug Administration CodesThe following CPT code may be appropriate to report Somatuline Depot administration services.Evaluation and Management (E&M) codes for office visit services in addition to injection may beappropriate. Most payers require documentation of a separate and identifiable procedure. Some payersmay not allow for a level one office visit and an injection code to be billed for the same date of service, andmay only allow for other levels of office visits to be billed with an appropriate modifier.CPT Code96372DescriptionTherapeutic, prophylactic, or diagnosis injection; subcutaneous or intramuscularPlease consult the patient’s specific plan or IPSEN CARES for information on other CPT codes that may be applicableand appropriate for billing the administration of Somatuline Depot.Please see accompanying full Prescribing Information and Patient Information.5
Diagnosis CodesAll claim forms should include an accurate and appropriately documented diagnosis code. Physiciansshould select the code that most closely and appropriately represents the diagnosis of the patient. Thefollowing codes below are provided as examples. Physicians should select codes that most accuratelyreflect a patient’s condition and corresponding utilization of Somatuline Depot.Diagnosis Codes for AcromegalyICD-10-CM CodeE22.0DescriptionAcromegaly and pituitary gigantismDiagnosis Codes for GEP-NETs*Note: This list is not exhaustive.ICD-10-CM CodeDescriptionC7A.01Malignant carcinoid tumors of the small intestineC7A.010Malignant carcinoid tumor of the duodenumC7A.011Malignant carcinoid tumor of the jejunumC7A.012Malignant carcinoid tumor of the ileumC7A.019Malignant carcinoid tumor of the small intestine, unspecified portionC7A.020Malignant carcinoid tumor of the appendixC7A.021Malignant carcinoid tumor of the cecum*Per CPT coding guidelines, patients with any associated multiple endocrine neoplasia syndrome diagnosis will havecodes E31.20 - E31.23 coded first and neuroendocrine diagnosis coded second.Please see accompanying full Prescribing Information and Patient Information.6
Diagnosis Codes for GEP-NETs* (Continued)ICD-10-CM CodeDescriptionC7A.023Malignant carcinoid tumor of the transverse colonC7A.024Malignant carcinoid tumor of the descending colonC7A.025Malignant carcinoid tumor of the sigmoid colonC7A.026Malignant carcinoid tumor of the rectumC7A.029Malignant carcinoid tumor of the large intestine, unspecified portionC7A.092Malignant carcinoid tumor of the stomachC7A.094Malignant carcinoid tumor of the foregut NOSC7A.095Malignant carcinoid tumor of the mid-gut NOSC7A.096Malignant carcinoid tumor of the hindgut NOSC7B.00Secondary carcinoid tumors, unspecified siteC7B.01Secondary carcinoid tumors of distant lymph nodesC7B.04Secondary carcinoid tumors of peritoneumC7B.09Secondary carcinoid tumors of other sitesC7B.8Other secondary neuroendocrine tumorsC24.1Malignant neoplasm of ampulla of VaterC25.4Malignant neoplasm of endocrine pancreasDiagnosis Code for Carcinoid SyndromeICD-10-CM CodeE34.0DescriptionCarcinoid syndrome*Per CPT coding guidelines, patients with any associated multiple endocrine neoplasia syndrome diagnosis will havecodes E31.20 - E31.23 coded first and neuroendocrine diagnosis coded second.Please see accompanying full Prescribing Information and Patient Information.7
Additional Information: Consult With Individual Payers asAppropriateAlways verify the patient's health insurance benefits prior to injecting Somatuline Depot. MedicareAdministrative Contractors (MACs) may develop coverage policies for Somatuline Depot at some point.Coverage policies from MACs are publicly available on the Centers for Medicare and Medicaid Services (CMS)website at www.cms.gov.CPT is 2017 American Medical Association (AMA). All rights reserved. No fee schedules, basic units, relativevalues, or related listings are included in CPT . The AMA assumes no liability for the data contained herein.Please see accompanying full Prescribing Information and Patient Information.8
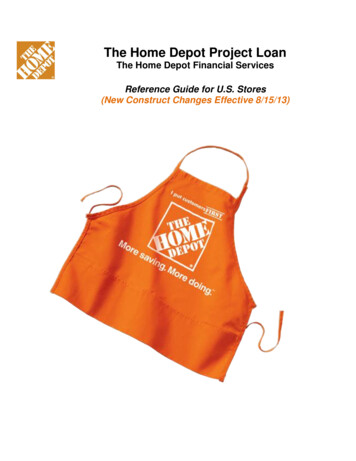
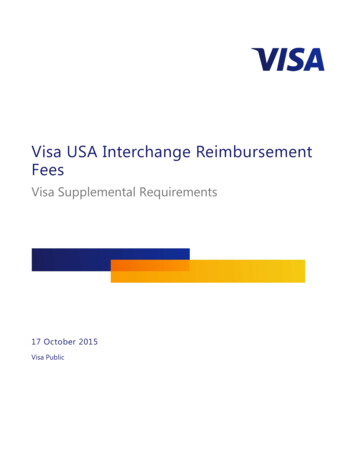
Sample CMS-1500 Claim Form for Somatuline DepotPhysician Office SettingPlease note that all codes listed on the sample forms are representative examples only. Coding must be selectedby the provider as appropriate based on diagnosis and treatment for the individual patient in each case.Sample CMS 1500Claim Form19Sample CMS 1500 Claim FormCARRIERCARRIER1500INSURANCE CLAIM FORMAPPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05HEALTH INSURANCE CLAIM caid #)(Medicaid#)CHAMPVACHAMPVAGROUPGROUPHEALTH PLANHEALTHPLAN(SSN or(SSNorID)ID)(Member(VA FileID#)#)2.2. PATIENT’S iddleMiddleInitial)Initial)3. PATIENT’SPATIENT’S )5.5. PATIENT’SADDRESS(No.,PATIENT’S .NUMBEROTHER e,FirstFirstName,Name,MiddleMiddle Initial)Initial)OTHERINSURED’SINSURED’S NAME10. EROTHER INSURED’SINSURED’S us)a.(CurrentororPrevious)b.b. OTHERINSURED’SDATEDATEOFOFBIRTHBIRTHOTHER MDDDDSEX D’SADDRESS(No.,Street)OtherOther8. PATIENTPATIENT ELEPHONE (Include((SpouseSpousec. EMPLOYER’S NAME OR SCHOOL NAME((a. INSURED’S DATE OF BIRTHSEXSEXM MFFb. EMPLOYER’S NAME OR SCHOOL NAMEb. EMPLOYER’S NAME OR SCHOOL NAMEPLACE (State)NONOc. INSURANCE PLAN NAME OR PROGRAM NAMEc. INSURANCE PLAN NAME OR PROGRAM NAMENONO10d. RESERVED FOR LOCAL USEd. INSURANCE PLAN NAME OR PROGRAM NAME))a. INSURED’S DATE OF BIRTHMM DD DDMMYY YYPLACE (State)c. OTHER ACCIDENT?YESYESd. INSURANCE PLAN NAME OR PROGRAM ER11.POLICYGROUPOR ORFECANUMBERc. OTHER ACCIDENT?c. EMPLOYER’S NAME OR SCHOOL IN ITEM1)(For PROGRAMProgram in Item1)(ID)(ID)SEXSEXM MPATIENT RELATIONSHIPRELATIONSHIPTOTOINSUREDINSURED6. PATIENTSelfSelfZIPZIPCODECODEFECAFECABLK LUNGBLKLUMG(SSN)(SSN)d. IS THERE ANOTHER HEALTH BENEFIT PLAN?d. IS THERE ANOTHER HEALTH BENEFIT PLAN?10d. RESERVED FOR LOCAL USEPATIENT AND INSURED INFORMATIONPICAPCA1.1. MEDICAREMEDICAREPATIENT AND INSURED INFORMATIONPLEASEDO NOTSTAPLEIN THISHEALTHAREAReserved for local use. This area may be usedto list the drug name.If yes,toreturnYESNOto and completeitem 9 a-d.YESNOand completeitem 9 a-d.If yes, returnREAD BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM.13. INSURED’S OR AUTHORIZED PERSON’S SIGNATURE I authorize paymentREAD PERSON’SBACK OF FORMBEFORECOMPLETING& SIGNINGTHIS FORM.OR AUTHORIZEDPERSON’SSIGNATUREI authorize12. PATIENT’S OR AUTHORIZEDSIGNATUREI authorizethe releaseof any medicalor other information necessary to 13. INSURED’Sof medical benefitsto the undersignedphysicianor supplierfor services12.processPATIENT’SOR AUTHORIZEDSIGNATUREbenefitsI authorizetheof anymedicalor otherinformationnecessarypaymentof below.medical benefits to the undersigned physician or supplier forthis claim.I also request PERSON’Spayment of governmenteithertoreleasemyself orto theparty whoacceptsassignmentbelow.describedto process this claim. I also request payment of government benefits either to myself or to the party who accepts assignmentservices described below.below.SIGNEDDATESIGNEDSIGNEDDATESIGNED14. DATE OF CURRENT:ILLNESS (First Symptom) OR15. IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS 16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATIONMM OCCUPATIONDDYYMMDDYYILLNESS(Accident)(First symptom)15.IF PATIENTHAS HAD SAMEOR DDSIMILAR YYILLNESS. 16. DATES PATIENTUNABLETOWORK IN CURRENT14. MMDATE OF DDCURRENT:YYOR ORGIVEFIRST ORGIVEFIRSTDATEPREGNANCY (LMP)FROMMMTO:FROMTOPREGNANCY(LMP)17a. I.D. NUMBER OF REFERRING PHYSICIAN18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES18. HOSPITALIZATIONDATES RELATEDTO CURRENT SERVICESMMMMDD DDYYYYMMMM DD DD YY YYFROMFROMTO TO17a.17b. NPIYESYESMM.DATE(S) OF SERVICEAFromToDATE(S) OF SERVICEDDYYMM ToDDFrom24AMMDDYYMMDD3. 3.24D2E E.DIAGNOSISPOINTERDIAGNOSISCODEF.F CHARGES CHARGES24EG.GDAYSORDAYSUNITSORUNITSH. HI.EPSDTID.FamilyEPSDTPlan QUAL.FamilyPlanJ.KRENDERINGPROVIDERID. #RESERVEDFORLOCAL USECOBIJ24GEMGNPINPI3NPI4NPI5NPI6NPI25. FEDERAL TAX I.D. NUMBER25. FEDERAL TAX I.D. NUMBERSSN EINSSNEIN31. SIGNATURE OF PHYSICIAN OR SUPPLIERINCLUDING DEGREES OR CREDENTIALS31. SIGNATURE OF PHYSICIAN OR SUPPLIER(I certify that the statements on the reverseINCLUDING DEGREES OR CREDENTIALSapply to this bill and are made a part thereof.)(I certify that the statements on the reverseapply to this bill and are made a part thereof.)SIGNEDDATESIGNED26. PATIENT’S ACCOUNT NO.27. ACCEPT ASSIGNMENT?(Forgovt. claims, see back)27. ACCEPT ASSIGNMENT?26. PATIENT’S ACCOUNT NO.YES(Forgovt. claims,NOsee back)32. SERVICE FACILITY LOCATION INFORMATIONYESNO32. NAME AND ADDRESS OF FACILITY WHERE SERVICESWERE RENDERED (if other than home or office)NPIa.DATEb.PLEASE PRINT OR TYPE03Doe, John22X63XMA61701239 555-555529. AMOUNT PAID 30. BALANCE DUE29. AMOUNT PAID33. BILLING PROVIDER INFO & PH #() 30. BALANCE DUEPIN #NPIInput the authorization number if obtainedfrom the insurance company.24A24DCPT /HCPCS code: Enter the appropriateCPT /HCPCS code. For Somatuline Depotuse J1930, Injection, lanreotide, 1 mg.Include the appropriate CPT codes to reportadministration procedures, (e.g., 96372,therapeutic, prophylactic, or diagnosticinjection, specify substance, or drug;subcutaneous or intramuscular). 33. PHYSICIANS, SUPPLIER’S BILLING NAME, ADDRESS, ZIP CODE& PHONE #b.GRP #APPROVED OMB-093-0999 FORM CMS-1500 (08/05)APPROVED OMB-0938-0008 FORM CMS-1500 (12-90), FORM RRB-1500.APPROVED OMB-1215-0055 FORM OWCP-1500, APPROVED OMB-0720-0001 (CHAMPUS)123 Any StreetCambridge28. TOTAL CHARGEa.PLEASE PRINT OR TYPENUCC Instruction Manual available at: www.nucc.org(APPROVED BY AMA COUNCIL ON MEDICAL SERVICE 8/88)28. TOTAL CHARGE23In the nonshaded area, list the date of ZATIONNUMBER4. 4.D. PROCEDURES,D SERVICES, OR SUPPLIES(Explain Unusual Circumstances)PROCEDURES, SERVICES, OR SUPPLIESCPT/HCPCSMODIFIER(Explain Unusual Circumstances)YY SERVICE SERVICECPT/HCPCSMODIFIERC.CB B.PLACE OFPLACETYPEYY OFSERVICE EMGOFPHYSICIAN OR SUPPLIER INFORMATION2. 2.24. A.24.121.Code to the highest level of specificity. ICD10-CM diagnosis codes contain 3-7 digits. Itis recommended that providers verify eachpayer’s specific coding requirements prior toinjecting.Example: N41504112003MG120.00 (Note:some payers may request the NDC number belisted in box 19). CHARGES teItems1,2,3TO ITEM24EBY DIAGNOSISDIAGNOSIS ORORORINJURY(RelateItems1, 2,3 orOR4 to4Item24E byLine)1. 1.2320.OUTSIDEOUTSIDELAB?20.LAB?PHYSICIAN OR SUPPLIER INFORMATION17. NAME OF REFERRING PROVIDER OR OTHER SOURCE19.FORLOCALLOCALUSEUSE19.RESERVEDRESERVED FOREnter the appropriate ICD-10-CM diagnosiscode, (e.g., C7A.092, malignant carcinoidtumor of the stomach).In the shaded area, list the N4 qualifier, the11-digit drug NDC#, the unit of measurementqualifier, and dosage.1917. NAME OF REFERRING PHYSICIAN OR OTHER SOURCE2124EFor each code, insert the reference numbercorresponding to the appropriate diagnosiscode in box 21.24GReport the appropriate number of units forthe procedure and the appropriate number ofmilligrams for Somatuline Depot J1930 (120mg, 90 mg, or 60 mg).NoteFor Somatuline Depot obtained through a Specialty Pharmacy, no charges for the drug should be billed by theprovider. However, inclusion of the HCPCS code (J1930) is recommended to designate the drug administeredand number of milligrams administered. Consult with the individual payer to determine the appropriate methodof documenting and billing for drugs obtained through a Specialty Pharmacy.Signature on filePlease see accompanying full Prescribing Information and Patient Information.Name of MD715916PIN Number
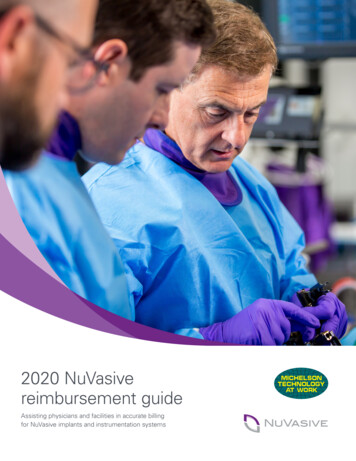
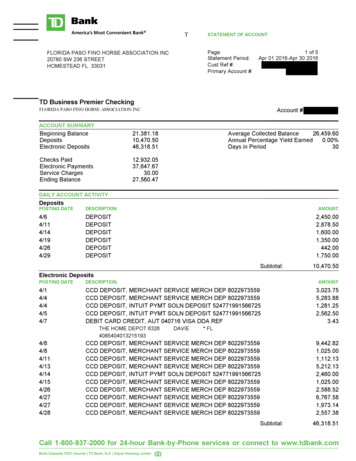
Sample CMS-1450 (UB-04) Claim Form for Somatuline DepotHospital Outpatient AdministrationPlease note that all codes listed on the sample forms are representative examples only. Coding must be selectedby the provider as appropriate based on diagnosis and treatment for the individual patient in each case.43a PAT.CNTL #b. MED.REC. #2165 FED. TAX NO.8 PATIENT NAME9 PATIENT ADDRESSa10 BIRTHDATE11 SEX12DATEacADMISSION13 HR 14 TYPE 15 SRC 16 DHR 17 34OCCURRENCECODEDATE33OCCURRENCEDATECODERevenue Code: Enter the appropriate numeric codeto identify specific accommodations and/or ancillaryservice in ascending numeric order by date of serviceif applicable.TYPEOF BILL7STATEMENT COVERS PERIODFROMTHROUGHbb42CONDITION CODES2422232135CODE38252636CODEOCCURRENCE SPANFROMTHROUGH39CODE40CODEVALUE CODESAMOUNT27d28For Somatuline Depot, the most commonly usedrevenue code is 0636. Use revenue code 0250,General Pharmacy, for payers who do not recognizethe 0636 revenue code.e29 ACDT 30STATE37OCCURRENCE SPANFROMTHROUGH41CODEVALUE CODESAMOUNTFor the administration, list the revenue code for thecost center where services were performed (e.g.,0510, clinic, 500, outpatient services, etc.).VALUE CODESAMOUNTabcd42 REV. CD.44 HCPCS / RATE / HIPPS CODE43 DESCRIPTION45 SERV. DATE46 SERV. UNITS47 TOTAL CHARGES48 NON-COVERED CHARGES491122334456424345 19202021212222PAGE23OFTOTALSCREATION DATE50 PAYER NAME52 REL.INFO51 HEALTH PLAN ID53 ASG.BEN.2355 EST. AMOUNT DUE54 PRIOR PAYMENTSA56 NPI57ABOTHERBCPRV IDC58 INSURED’S NAME62 INSURANCE GROUP NO.61 GROUP NAME59 P. REL 60 INSURED’S UNIQUE IDAABBCC63 TREATMENT AUTHORIZATION CODES67AB65 EMPLOYER NAME64 DOCUMENT CONTROL NUMBERABC43Revenue Description: Enter the narrative descriptionof the related room and board and/or ancillarycategories shown in box 42. For payers that require adetailed drug description, a drug description can beinserted. The N4 indicator is listed first, the 11-digitNDC number is listed second, a code describing theunit of measurement qualifier is listed third, and theunit quantity is listed at the end.44CPT /HCPCS Code: Enter the appropriate CPT /HCPCS code.For Somatuline Depot use J1930, Injection,lanreotide, 1 mg.For the administration use the CPT coderepresenting the administration route, (e.g., 96372,therapeutic, prophylactic, or diagnostic injection,specify substance, or drug; subcutaneous orintramuscular).45Service Date: Enter the date on which the service wasperformed using a MMDDYY format.C66DX67IAJ69 ADMIT70 PATIENTDXREASON DXPRINCIPAL PROCEDUREa.74CODEDATEBKabCLOTHER PROCEDURECODEDATEb.OTHER PROCEDURECODEDATEe.cDM71 PPSCODEOTHER PROCEDURECODEDATEEN7572ECIFO76 ATTENDINGGPNPILASTc.OTHER PROCEDURECODEDATEd.OTHER PROCEDURECODEDATE77 OPERATINGbcdUB-04 CMS-1450APPROVED OMB NO.78 OTHERLAST46Service Units: Enter the total number of units ofservice as appropriate and the appropriate number ofmilligrams for Somatuline Depot (120 mg, 90 mg, or60 mg).QUALQUALFIRSTNPILAST79 OTHER6873FIRSTNPILAST81CCa80 REMARKSHQQUALFIRSTNPIQUALFIRSTTHE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF.NUBC National UniformBilling CommitteeLIC921325767Enter the complete ICD-10-CM diagnosis code, (e.g.,C7A.092, malignant carcinoid tumor of the stomach).Code to the highest level of specificity. ICD-10CM diagnosis codes contain 3 to 7 digits. It isrecommended that providers verify each payer’sspecific coding requirements prior to injecting.Please see accompanying full Prescribing Information and Patient Information.10
Product InformationNDC*DescriptionDispensing/SalePack Quantity15054-1060-0315054-1090-0315054-1120-0360 mg/0.2 mL sterile, prefilled syringe90 mg/0.3 mL sterile, prefilled syringe120 mg/0.5 mL sterile, prefilled syringe111*Please note that for billing purposes, the NDC number requires 11 digits. Therefore, a zero must be entered into the 10thposition (e.g., “15054-1120-03”). This is consistent with Red Book and First DataBank listings.HCPCS Code for Somatuline DepotJ1930, Injection, lanreotide, 1 mg.Somatuline Depot Pack DimensionsApproximate Dimensions – UnitDepth: 3.5”, Height: 0.8”, Width: 12”Storage and Handling InformationStore Somatuline Depot in the refrigerator at 2 C to 8 C (36 F to 46 F). Protect from light. Store in the originalpackage.Sales Unit to TradeOne dispensing pack.Product ExpirationThe expiration date is printed on each dispensing pack and syringe label.Special Shipping RequirementSomatuline Depot is labeled with specific transportation and storage requirements. Care should be takento ensure that temperature control at 2 C to 8 C (36 F to 46 F) is maintained during these activities. Whenshipping Somatuline Depot, a foam or gel refrigerant ice that has been frozen hard at -18 C (0 F) for aminimum of 24 hours should be used. Somatuline Depot should never be exposed to dry ice. Ipsen will shipSomatuline Depot in a manner that maintains its temperature to meet the requirements stated above duringtransport from Ipsen to the product destination. Specialty Distributors and Specialty Pharmacies should alsopackage and ship Somatuline Depot in a manner that maintains this same environment.Customers should call 1-855-463-5127 if they have any questions pertaining to proper shipping.Product ReturnsCredit for returns is subject to Ipsen’s current Return Goods Policy. Please contact Returns.USA@Ipsen.com formore information or to receive a Return Goods Authorization.Please see accompanying full Prescribing Information and Patient Information.11
Payer CoverageContacting the payer directly is the best way to determine how the physician may obtain reimbursement forSomatuline Depot. This may be done as part of an insurance benefit verification effort. Benefit verificationprovides the physician with important reimbursement information, such as benefit structure and coverage, andis typically performed prior to treatment. To ensure accuracy, benefit verifications should be conducted on apatient-specific basis.Contact IPSEN CARES or your Ipsen Field Reimbursement Manager for more information regarding codingcoverage and reimbursement, including local medical policies.MedicareMedicare may cover Somatuline Depot (lanreotide) Injection under the Part B benefit when provided andadministered by a healthcare provider and under the Part D benefit when dispensed in an outpatient setting.When covered as a Part B benefit, claims for Somatuline Depot are billed to Medicare AdministrativeContractors (MACs).Local Medicare Administrative Contractors manage Medicare Part A/B Benefits. MACs may make specificcoverage decisions for Somatuline Depot through Local Coverage Decisions (LCDs) and may issue othercoverage instructions through articles and bulletins. The absence of a published coverage policy does notmean that there is no coverage for Somatuline Depot.The Part D drug benefit provides beneficiaries with coverage for outpatient prescription drugs. The PartD benefit is administered by private health plans, such as stand-alone prescription drug plans (PDPs) orMedicare Advantage prescription drug (MA-PD) plans. The standard benefit design for Medicare Part Dcoverage includes an annual deductible.MedicaidMost state Medicaid programs cover and reimburse Somatuline Depot.1 Medicaid coverage and payment forSomatuline Depot varies from state to state. Providers should check with the state program or may contactIPSEN CARES for more specific coverage information.Private PayersPrivate payers vary in the payment methods they use to reimburse the sites of service where Somatuline Depot is administered. Some private payers may require that physicians obtain Somatuline Depotthrough a Specialty Pharmacy. Specialty Pharmacies may bill the payer through the medical or pharmacybenefit, depending on the payer’s requirements.1Fingertip Formulary Customized Report. January 2016.Please see accompanying full Prescribing Information and Patient Information.12
IPSEN CARES REIMBURSEMENT AND SUPPORTPersonal Support at Your Patients’ FingertipsThe IPSEN CARES team is fully dedicated to: Facilitating eligible patients’ access to the Ipsen medications that are important to their care Providing information and support for the interactions between your office, your patients, and your patients’ insurancecompanyIPSEN CARES provides a single point of contact for you, your staff, and your patients.Ipsen is proud of our patient support program, IPSEN CARES , which is available for your patients and your practice.PHONE OR FAX1-866-435-5677Fax: 1-888-525-2416HOURSMonday through Friday8:00 AM to 8:00 PM ETWEBSITEwww.ipsencares.comReimbursement AssistanceFinancial Support Benefits Verification – verifies patients’ coverage, Copayment Assistance – offers copayment assistancerestrictions (if applicable), and copayment/coinsurance amounts. Prior Authorization (PA) – provides information ondocumentation required by payers on PA specificsand recommendations for next steps based on payerpolicy. Appeals Information – provides information on theto eligible* patients. This includes referring to theSomatuline Depot Commercial Copay Program orreferring to an independent non-profit organization ifavailable. Patient Assistance Program (PAP) – determinespatients’ eligibility for PAP and dispenses freeproduct to eligible patients.payer-specific processes required to submit a level Ior a level II appeal, as well as provides guidance asneeded through the process.Product DistributionPatient Support Specialty Distributor Network – provides contact Communication – conducts calls to both health-information to various distributors that can supplySomatuline Depot directly to your facility. Specialty Pharmacy Network – determines whichcare
Always verify the patient's health insurance benefits prior to injecting Somatuline Depot. Medicare Administrative Contractors (MACs) may develop coverage policies for Somatuline Depot at some point. Coverage policies from MACs are publicly available on the Centers for Med