Transcription
VA/DoD Clinical Practice GuidelinesVA/DoD Clinical Practice Guideline for theManagement of SubstanceUse DisordersProvider SummaryVersion 4.0 2021
VA/DoD CLINICAL PRACTICE GUIDELINEFOR THE MANAGEMENT OFSUBSTANCE USE DISORDERSDepartment of Veterans AffairsDepartment of DefenseProvider SummaryQUALIFYING STATEMENTSThe Department of Veterans Affairs and the Department of Defense guidelines are based upon the bestinformation available at the time of publication. They are designed to provide information and assistdecision making. They are not intended to define a standard of care and should not be construed as one.Neither should they be interpreted as prescribing an exclusive course of management.This Clinical Practice Guideline is based on a systematic review of both clinical and epidemiologicalevidence. Developed by a panel of multidisciplinary experts, it provides a clear explanation of the logicalrelationships between various care options and health outcomes while rating both the quality of theevidence and the strength of the recommendation.Variations in practice will inevitably and appropriately occur when clinicians take into account the needs ofindividual patients, available resources, and limitations unique to an institution or type of practice. Everyhealthcare professional making use of these guidelines is responsible for evaluating the appropriateness ofapplying them in the setting of any particular clinical situation.These guidelines are not intended to represent Department of Veterans Affairs or TRICARE policy. Further,inclusion of recommendations for specific testing and/or therapeutic interventions within these guidelinesdoes not guarantee coverage of civilian sector care. Additional information on current TRICARE benefitsmay be found at www.tricare.mil by contacting your regional TRICARE Managed Care Support Contractor.Version 4.0 – 2021
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersTable of ContentsIntroduction . 1Recommendations . 2Algorithm . 7Module A: Screening and Treatment . 8Module B: Stabilization and Withdrawal . 10Scope of the CPG . 12Highlighted Features of this Guideline . 12Methods. 13Guideline Work Group. 14Patient-centered Care . 15Shared Decision Making . 16Pharmacotherapy Considerations. 17Other Medications for AUD: Not Recommended. 25Psychosocial Intervention Considerations . 33A.Behavioral Couples Therapy . 33B.Cognitive Behavioral Therapy . 34C.Community Reinforcement Approach . 34D.Contingency Management . 34E.Individual Drug Counseling . 35F.Motivational Enhancement Therapy . 35G.12-step Facilitation . 35References . 36August 2021
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersIntroductionThe Department of Veterans Affairs (VA) and Department of Defense (DoD) Evidence-Based Practice WorkGroup (EBPWG) was established and first chartered in 2004, with a mission to advise the Health ExecutiveCommittee (HEC) “ on the use of clinical and epidemiological evidence to improve the health of thepopulation ” across the Veterans Health Administration (VHA) and Military Health System (MHS), byfacilitating the development of clinical practice guidelines (CPGs) for the VA and DoD populations.(1)Development and update of VA/DoD CPGs is funded by VA Evidence Based Practice, Office of Quality andPatient Safety. The system-wide goal of evidence-based CPGs is to improve patient health and well-being.In 2015, the VA and DoD published a CPG for the Management of Substance Use Disorders (2015 VA/DoDSUD CPG), which was based on evidence reviewed from November 2007 through January 2015. The 2015VA/DoD SUD CPG updated the 2009 VA/DoD CPG and for the first time addressed substance use disordercare in non-addiction care settings. Since the release of that CPG, a growing body of research hascontinued to inform evidence-based practices for the screening, assessment, and treatment of substanceuse disorders (SUD). a Consequently, a recommendation to update the 2015 VA/DoD SUD CPG was initiatedin 2020.This CPG provides an evidence-based framework for evaluating, treating, and managing the individualneeds of patients with SUD in the VA and DoD. It is intended for use by all VA and DoD healthcareproviders. Successful implementation of this CPG will: Assist providers in assessing the patient’s condition and collaborating with the patient, theirfamily, and their caregivers to determine optimal management of patient care Emphasize the use of patient-centered care Minimize preventable complications and morbidity Optimize individual health outcomes and quality of lifeThe full VA/DoD SUD CPG, as well as additional toolkit materials including a pocket card and patientsummary, can be found at: /.aIn this CPG, the term SUD encompasses alcohol use disorder (AUD), opioid use disorder (OUD), sedative hypnotic use disorder,stimulant use disorder, and cannabis use disorder.August 2021Page 1 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersRecommendationsThe following evidence-based clinical practice recommendations were made using a systematic approachconsidering four domains as per the Grading of Recommendations Assessment, Development andEvaluation (GRADE) approach (see Appendix A in the full VA/DoD SUD CPG). These domains include:confidence in the quality of the evidence, balance of desirable and undesirable outcomes (i.e., benefits andharms), patient values and preferences, and other implications (e.g., resource use, equity, acceptability).Table 1. RecommendationsSubtopica. Alcohol Use DisorderStabilization and WithdrawalTreatmentSettingScreening and Brief Alcohol InterventionTopicAugust 2021#RecommendationStrengthaCategoryb1.For patients in general medical and mental healthcare settings,we recommend screening for unhealthy alcohol use periodicallyusing the three-item Alcohol Use Disorders Identification TestConsumption (AUDIT-C) or Single Item Alcohol ScreeningQuestionnaire (SASQ).Strong forNotreviewed,Amended2.For patients without documented alcohol use disorder whoscreen positive for unhealthy alcohol use, we suggest providing asingle initial brief intervention regarding alcohol-related risks andadvising to abstain or drink within established limits for daily andweekly consumption.Weak forNotreviewed,Amended3.There is insufficient evidence to recommend for or againstscreening for drug use disorders in primary care to facilitateenrollment in treatment.Neither for Reviewed,nor against New-added4.For patients with substance use disorders, there is insufficientevidence to recommend for or against using a standardizedassessment that would determine initial intensity and setting ofsubstance use disorder care.Neither fornor againstNotreviewed,Amended5.For the treatment of moderate-severe alcohol withdrawal, werecommend using benzodiazepines with adequate monitoring.Strong forNotreviewed,Amended6.For managing mild-moderate alcohol withdrawal in patients forwhom risks of benzodiazepines outweigh benefits(e.g., inadequate monitoring available, abuse liability, orallergy/adverse reactions), we suggest consideringcarbamazepine, gabapentin, or valproic acid as an alternative.Weak forNotreviewed,NotchangedPage 2 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use Disordersc. Sedative Hypnotic UseDisorderb. Opioid Use DisorderSubtopica. Alcohol Use Disorder —PharmacotherapyTreatmentStabilization and Withdrawal (cont.)TopicAugust Notreviewed,Amended7.For patients with opioid use disorder, we recommend againstwithdrawal management, without planned ongoingpharmacotherapy treatment, due to high risk of relapse andoverdose (see Recommendations 16, 17, and 18).8.For patients with opioid use disorder for whom opioid withdrawalmanagement is indicated, we suggest using:-Buprenorphine/naloxone (in any setting); or-Methadone or buprenorphine/naloxone (in inpatient oraccredited Opioid Treatment Programs) (seeRecommendation 17).Weak forReviewed,Newreplaced9.For patients with opioid use disorder for whom withdrawalmanagement is indicated and for whom methadone andbuprenorphine are contraindicated, unacceptable, or unavailable,we suggest offering clonidine or lofexidine as a second-line agentfor opioid withdrawal management (see Recommendation 17).Weak forReviewed,Newreplaced10.For patients in need of withdrawal management forbenzodiazepines, we recommend gradually taperingbenzodiazepines.Strong forReviewed,Newreplaced11.There is insufficient evidence to recommend the use of adjunctive Neither for Reviewed,medications for the treatment of benzodiazepine withdrawal.nor against New-addedFor patients with moderate-severe alcohol use disorder, werecommend offering one of the following medications:12. Naltrexone (oral or extended-release) TopiramateStrong forNotreviewed,AmendedFor patients with moderate-severe alcohol use disorder, wesuggest offering one of the following medications:13. Acamprosate DisulfiramWeak forNotreviewed,AmendedWeak forNotreviewed,NotchangedFor patients with moderate-severe alcohol use disorder for whom14. first-line pharmacotherapy is contraindicated or ineffective, wesuggest offering gabapentin.Page 3 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersSubtopicc. Opioid Use Disorder –Pharmacotherapyd. Opioid Use Disorder –Psychosocial Interventionse. Cannabis Use Disorder –PharmacotherapyTreatment (cont.)b. Alcohol Use Disorder –Psychosocial InterventionsTopicAugust 2021#RecommendationStrengthaCategoryb15.For patients with alcohol use disorder, we suggest one or more ofthe following interventions, considering patient preference andavailability: Behavioral couples therapy Cognitive behavioral therapy Community reinforcement approach Motivational enhancement therapy 12-step facilitationWeak forNotreviewed,Amended16.For patients with opioid use disorder, we recommend one of thefollowing strategies: Buprenorphine/naloxone in any setting; or Methadone or buprenorphine/naloxone provided through anaccredited Opioid Treatment ProgramStrong forReviewed,Amended17.For patients with opioid use disorder, we suggest offeringextended-release naltrexone (IM).Weak forReviewed,Newreplaced18.There is insufficient evidence to recommend any one of thedifferent FDA-approved formulations or routes of delivery ofbuprenorphine over another.Neither for Reviewed,nor against New-added19.There is insufficient evidence to recommend for or against oralnaltrexone for the treatment of opioid use disorder.Neither fornor againstReviewed,Notchanged20.For patients receiving medication treatment for opioid usedisorder, there is insufficient evidence to recommend for oragainst any specific psychosocial interventions in addition toaddiction-focused medical management.Neither fornor againstReviewed,Amended21.For patients with opioid use disorder for whom opioid usedisorder pharmacotherapy is contraindicated, unacceptable, orunavailable, there is insufficient evidence to recommend for oragainst any specific psychosocial interventions.Neither fornor againstNotreviewed,Amended22.There is insufficient evidence to recommend for or against theuse of pharmacotherapy in the treatment of cannabis usedisorder.Neither fornor againstReviewed,NotchangedPage 4 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersSubtopicg. Stimulant Use Disorder –Pharmacotherapyh. Stimulant Use Disorder –Psychosocial InterventionsTreatment (cont.)f. Cannabis Use Disorder –Psychosocial InterventionsTopicAugust 2021#RecommendationStrengthaCategorybWeak ere is insufficient evidence to recommend for or against the25. use of any pharmacotherapy for the treatment of cocaine usedisorder or amphetamine/methamphetamine use disorder.Neither fornor againstReviewed,AmendedFor patients with cocaine use disorder, we recommend one ormore of the following interventions as initial treatment,considering patient preference and availability: Cognitive behavioral therapy26. Recovery-focused behavioral therapy (i.e., individual drugcounseling and community reinforcement approach) Contingency management in combination with anotherbehavioral intervention considering patient preference andavailabilityStrong forNotreviewed,AmendedFor patients with amphetamine/methamphetamine use disorder,we suggest offering contingency management as initial treatment27.in combination with another behavioral intervention, consideringpatient preference and availability.Weak forNotreviewed,AmendedFor patients with cannabis use disorder, we suggest one of thefollowing interventions as initial treatment, considering patientpreference and availability:23. Cognitive behavioral therapy Motivational enhancement therapy Combined cognitive behavioral therapy/motivationalenhancement therapy24.We suggest against the use of a brief intervention (i.e., 60minutes or less) for the treatment of cannabis use disorder.Page 5 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use iesGroup Mutual Help bFor patients with alcohol use disorder in early recovery orfollowing relapse, we recommend promoting active involvementin group mutual help programs using one of the followingsystematic approaches, considering patient preference and28. availability: Peer linkage Network support 12-step facilitationStrong forReviewed,NewreplacedFor patients with drug use disorders in early recovery or followingrelapse, we suggest promoting active involvement in groupmutual help programs using one of the following systematic29. approaches, considering patient preference and availability: Peer linkage 12-step facilitationWeak forReviewed,Newreplaced30.There is insufficient evidence to recommend for or againstmindfulness-based therapies for the treatment of substance usedisorders.31.We suggest using technology-based interventions (e.g.,automated text/voice messaging, smartphone apps), in additionto usual care, for alcohol use disorder.32.There is insufficient evidence to recommend for or against usingtechnology-based interventions (e.g., automated text/voicemessaging, smartphone apps), in addition to usual care, forsubstance use disorders other than alcohol use disorder.33.We suggest the use of structured telephone-based care as anadjunct to usual care for substance use disorders.34.There is insufficient evidence to recommend for or against theuse of telemedicine-delivered treatment for substance usedisorders.Neither for Reviewed,nor against New-added35.There is insufficient evidence to recommend for or against theuse of computer-delivered behavioral treatments, either alone orin combination with usual care, for substance use disorders.Neither for Reviewed,nor against New-addedNeither for Reviewed,nor against New-addedWeak forReviewed,New-addedNeither for Reviewed,nor against New-addedWeak forReviewed,New-addedFor additional information, see Grading Recommendations in the full VA/DoD SUD CPG.For additional information, see Recommendation Categorization and Appendix D in the full VA/DoD SUD CPG.August 2021Page 6 of 37
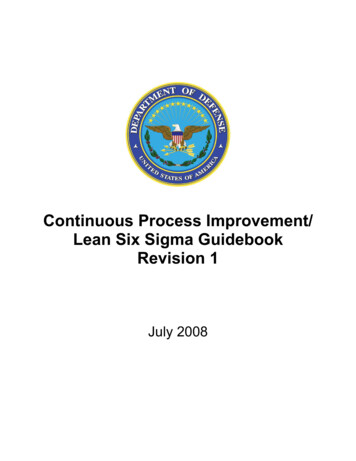
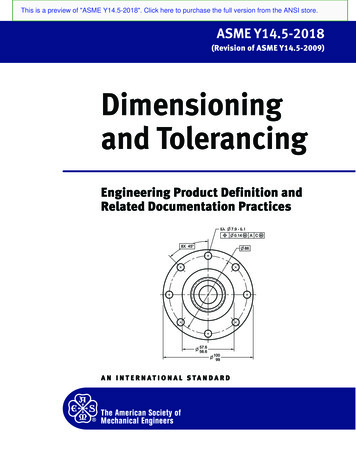
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersAlgorithmThis CPG’s algorithm is designed to facilitate understanding of the clinical pathway and decision makingprocess used in managing patients with SUD. This algorithm format represents a simplified flow of themanagement of patients with SUD and helps foster efficient decision making by providers. It includes: An ordered sequence of steps of care Decisions to be considered Recommended decision criteria Actions to be takenThe algorithm is a step-by-step decision tree. Standardized symbols are used to display each step, andarrows connect the numbered boxes indicating the order in which the steps should be followed.(2)Sidebars provide more detailed information to assist in defining and interpreting elements in the boxes.ShapeDescriptionRounded rectangles represent a clinical state or conditionHexagons represent a decision point in the process of care, formulated as a question thatcan be answered “Yes” or “No”Rectangles represent an action in the process of careOvals represent a link to another section within the algorithmFor alternative text descriptions of the algorithm, please refer to Appendix G in the full VA/DoD SUD CPG.August 2021Page 7 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersModule A: Screening and Treatment* DoD active duty: Referral to specialty SUD care is required in any incident in which substance use is suspected to be acontributing factor. For refusal, contact Command to discuss administrative and clinical options.** For patients with tobacco use disorder, see guidance on tobacco smoking cessation in adults from the U.S. Preventive ServicesTask Force (USPSTF) and-pregnant-women-counseling-and-interventions) and the Treating Tobacco Use and Dependence: 2008 Update – ClinicalPractice Guideline from the Agency for Healthcare Research and Quality tobacco/clinicians/index.html).*** Specific to specialty care settingAbbreviations: AUD: alcohol use disorder; AUDIT-C: Alcohol Use Disorders Identification Test – Consumption; CPG: clinical practiceguideline; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th edition; DoD: Department of Defense; OUD: opioid usedisorder; SUD: substance use disorders; VA: Department of Veterans AffairsAugust 2021Page 8 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersSidebar 1: Recommended Limits for Alcohol ConsumptionaMen age 65 or below: 2 standard drinks per day on average; 4 drinks on any one day; 14 drinks per weekMen over age 65 and all women: 1 standard drink per day on average; 3 drinks on any one day; 7 drinks perweekPatients with contraindications including potential drug-drug interactions: 0 standard drinks per dayaFor more information on recommended limits for alcohol consumption, please iew-alcohol-consumption/moderate-binge-drinking 0-2025-dietary-guidelines-online-materials. Please note the above limits areadapted from these sources.Sidebar 2: Brief Intervention Overview1.2.3.4.Express concernAdvise (abstain or decrease drinking)Provide feedback linking alcohol use and healthOffer referral to addiction treatment if appropriateSidebar 3: PharmacotherapyAlcohol Use DisorderRecommended: naltrexone, topiramateSuggested: acamprosate, disulfiramSuggested as second line: gabapentinOpioid Use DisorderRecommended: buprenorphine/naloxone, methadoneSuggested: extended-release naltrexoneSidebar 4: Components of Addiction-focused Medical Management Monitoring adherence, response to treatment, and adverse effectsEducation about AUD/OUD, health consequences, and treatmentsEncouragement to abstain from illicit opioids and other addictive substancesEncouragement to attend and referral to community supports for recoveryEncouragement to make lifestyle changes that support recoveryAbbreviations: AUD: alcohol use disorder; OUD: opioid use disorderSidebar 5: SUD and Co-occurring Conditions Refer to corresponding section of CPG on SUD and co-occurring conditions Consult other VA/DoD CPGs (e.g., Asthma, Chronic Insomnia Disorder and Obstructive Sleep Apnea, CKD, CMI,COPD, Diabetes Mellitus, Headache, Hypertension, LBP, MDD, mTBI, PTSD, Opioid Therapy for Chronic Pain,Osteoarthritis, Stroke, and Suicide)Abbreviations: CKD: Chronic Kidney Disease; CMI: Chronic Multisymptom Illness; COPD: Chronic Obstructive Pulmonary Disease;CPG: clinical practice guideline; DoD: Department of Defense; LBP: Low Back Pain; MDD: Major Depressive Disorder; mTBI: MildTraumatic Brain Injury; PTSD: Posttraumatic Stress Disorder; SUD: substance use disorders; VA: Department of Veterans AffairsAugust 2021Page 9 of 37
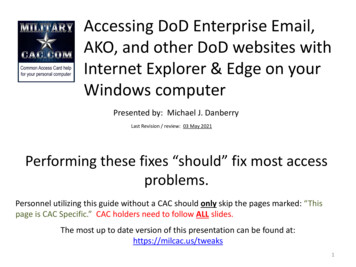
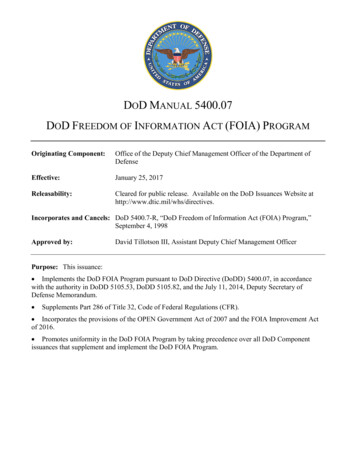
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersModule B: Stabilization and WithdrawalAbbreviations: CIWA-Ar: Clinical Institute Withdrawal Assessment for Alcohol-Revised; COWS: Clinical Opiate Withdrawal Scale;DoD: Department of Defense; OUD: opioid use disorder; SUD: substance use disordersAugust 2021Page 10 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersSidebar 6: Treatment Setting for Alcohol WithdrawalInpatient medically supervised alcohol withdrawal management is strongly supported by expert consensus forpatients with symptoms of severe alcohol withdrawal (i.e., CIWA-Ar score 20) or patients with: History of delirium tremens or withdrawal seizuresInability to tolerate oral medicationCo-occurring medical conditions that would pose serious risk for ambulatory withdrawal managementRisk of withdrawal from other substances in addition to alcohol (e.g., sedative hypnotics)Moderate alcohol withdrawal (i.e., CIWA-Ar score 10) and any of the following: Recurrent unsuccessful attempts at ambulatory withdrawal management Reasonable likelihood that the patient will not complete ambulatory withdrawal management (e.g., due tohomelessness) Active psychosis or severe cognitive impairmentAbbreviations: CIWA-Ar: Clinical Institute Withdrawal Assessment for Alcohol-RevisedSidebar 7: Pharmacologic TreatmentAlcohol WithdrawalFor managing moderate-severe alcohol withdrawal: BenzodiazepinesFor patients without severe alcohol withdrawal for whom risks of benzodiazepines outweigh benefits: Carbamazepine Gabapentin Valproic acidOpioid WithdrawalFor patients with OUD for whom maintenance agonist treatment is contraindicated, unacceptable, or unavailable,we recommend a taper using: Buprenorphine Methadone in inpatient or OTP onlyFor patients with OUD for whom methadone and/or buprenorphine are contraindicated, unacceptable,unavailable, or for whom extended-release injectable naltrexone is planned: Lofexidine or clonidineAbbreviations: OTP: Opioid Treatment Program; OUD: opioid use disorderSidebar 8: Tapering StrategiesAlcohol Withdrawal (use one of the following) A predetermined fixed medication tapering schedule with additional medication as needed Symptom-triggered therapy where patients are given medication only when signs or symptoms of withdrawaloccur (e.g., PRN dosing)Opioid Withdrawal Use structured taper for methadone and buprenorphineAbbreviations: PRN: as neededAugust 2021Page 11 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use DisordersScope of the CPGThis CPG is based on published clinical evidence and related information available through June 30, 2020.It is intended to provide general guidance on best evidence-based practices (see Appendix A in the fullVA/DoD SUD CPG for additional information on the evidence review methodology). This CPG is notintended to serve as a standard of care.This CPG is designed to assist providers (e.g., physicians, physician assistants, nurse practitioners, nurses,psychologists, social workers, pharmacists, addiction counselors, chaplains, nutritionists, dieticians,emergency care providers, behavioral health providers) in screening, assessing, and treating patients withalcohol and substance misuse and SUD. This guideline seeks to inform providers with practical evidencebased recommendations for the most common scenarios involving patients with alcohol and substancemisuse and SUD.The patient population of interest for this CPG is Veterans, active duty Service Members, or non-activeduty Service Members 18 years old, as well as other adults 18 years old who are eligible for care in theVA and/or DoD healthcare delivery systems, who have symptoms and/or a diagnosis of SUD, includingAUD, OUD, sedative hypnotic use disorder, stimulant use disorder, or cannabis use disorder. This CPG doesnot specifically address tobacco use disorder.For management of tobacco use disorder, see guidance on tobacco smoking cessation in adults from theU.S. Preventive Services Task Force tions) and the Treating Tobacco Use andDependence: 2008 Update – Clinical Practice Guideline from the Agency for Healthcare Research andQuality (AHRQ) o/clinicians/index.html).Highlighted Features of this GuidelineThe current document is an update to the 2015 VA/DoD SUD CPG. The following significant updates makeit important that providers review this version of the guideline: More rigorous application of GRADE methodology Updated algorithm for screening and treatment of SUD Updated algorithm for management of alcohol and opioid withdrawal syndromes Better definition of first- and second-line pharmacologic therapy for AUD and OUD Evaluated evidence regarding mindfulness-based approaches for the treatment of SUD Inclusion of recommendations on technology-based interventions, telephone-based care,telemedicine-delivered treatment, and computer-delivered behavioral treatmentsThe 2021 VA/DoD SUD CPG used stricter methodology than previous iterations. For additional informationon GRADE and CPG methodology, see Appendix A in the full VA/DoD SUD CPG.The 2021 VA/DoD SUD CPG is the 4th update to this CPG. It provides clinical practice recommendationsfor the care of patients with SUD (see Recommendations). In addition, the Algorithm incorporates theAugust 2021Page 12 of 37
VA/DoD Clinical Practice Guideline for the Management of Substance Use Disordersrecommendations in the context of the flow of patient care. The CPG also includes research prioritiesthat identify areas needing additional research (see the Research Priorities section in the full VA/DoDSUD CPG).MethodsThe methodology used in developing this CPG follows the Guideline for Guidelines, an internal documentof the VA and DoD EBPWG updated in January 2019 that outlines procedures for developing andsubmitting VA/DoD CPGs.(3) The Guideline for Guidelines is available . This CPG also aligns with the National Academy ofMedicine’s (NAM) principles of trustworthy CPGs (e.g., explanation of evidence quality and strength, themanagement of conflicts of interest [COI], interdisciplinary stakeholder involvement, use of systematicreview, and external review).(4) Appendix A in the full VA/DoD SUD CPG provides a detailed description ofthe CPG development methodology.The Work Group used the Grading of Recommendations Assessment, Development and Evaluation(GRADE) approach to craft each recommendation and determine its strength. Per GRADE approach,recommendations must be evidence-based and cannot be made based on expert opinion alone. TheGRADE approach uses the following four domains to inform the strength of each recommendation:confidence in the quality of the evidence, balance of desirable and undesirable outcomes, patient valuesand preferences, other considerations as appropriate (e.g., resource use, equity) (see GradingRecommendations in the ful
A. Behavioral Couples Therapy 33 . B. Cognitive Behavioral Therapy 34 . C. Community Reinforcement Approach 34 . D. Contingency Management 34 . E. Individual Drug Counseling 35 . F. Motivational Enhancement Therapy