Transcription
MINISTRY OF HEALTH OF UKRAINEZAPORIZHZHYA STATE MEDICAL UNIVERSITYBiological Chemistry DepartmentBIOCHEMISTRY OF VITAMINSTextbook for students of international facultySpeciality: 7.120 10001 «General Medicine»Zaporizhzhya - 20161
Reviewers:Kaplaushenko A.G. Head of Physical and Colloidal Chemistry Department,doctor of pharmaceutical science, associate professorVoskoboynik O. Yu. Assoc. professor of Organic and Bioorganic ChemistryDepartment, Ph. D.Authors:Aleksandrova K.V.Rudko N.P.Aleksandrova K.V.Biochemistry of vitamins. Textbook for students of international facultyspeciality: 7.120 10001 «General Medicine» / K.V. Aleksandrova, N.P. Rudko. –Zaporizhzhya : ZSMU, 2016.- 73 p.This textbook is recommended to use for students of international faculty (thesecond year of study) for independent work at home and in class. It is created asadditional manual for study of Biochemistry for students of international faculty.Александрова К.В.Біохімія вітамінів. Начально-методичний посібник для студентівміжнародного факультету спеціальності 7.120 10001 «Лікувальна справа»/К.В. Александрова, Н.П. Рудько,.- Запоріжжя : ЗДМУ, 2016. – 73 с. Aleksandrova K.V., Krisanova N.V.,Ivanchenko D.G., Rudko N.P., , 2016 Zaporizhzhya State Medical University, 20162
INTRODUCTIONSometimes it is difficult for students to find out the main important notionsfor study of biochemistry in basic literature that is recommended. Theeducational process for students of medical department requires the use not onlythe basic literature but also that one which is discussed as additional literaturesources. This is because each day we have new scientific researches inbiochemistry, later which can improve our understanding of theoretical questionsthis subject. This manual is proposed by authors as additional one for study ofwater-soluble and fat-soluble vitamins: their structure, properties, functions andmetabolism in human organism.Authors3
CONTENTINTRODUCTION .3GENERAL INFORMATION ABOUT VITAMINS 5CLASSIFICATION AND NOMENCLATURE OF THE VITAMINS.10GROUP I. FAT-SOLUBLE VITAMINS .13GROUP II. WATER-SOLUBLE VITAMINS.24GROUP III. VITAMIN-LIKE SUBSTANCES.43HEALTH EFFECTS OF VITAMINS AND ANTIVITAMINS . 45METHODS USED IN VITAMIN RESEARCH .47TEST-TASKS FOR SELF-CONTROL .60ANSWERS TO TEST-TASKS FOR SELF-CONTROL .72LITERATURE . 734
GENERAL INFORMATION ABOUT VITAMINSVitamins are a group of organic nutrients of various nature required in smallquantities for multiple biochemical reactions for the growth, survival andreproduction of the organism, and which, generally, cannot be synthesized by thebody and must therefore be supplied by the diet. The most prominent function ofthe vitamins is to serve as coenzymes (or prosthetic group) for enzymatic reactions.The discovery of the vitamins began with experiments performed byHopkins at the beginning of the twentieth century; he fed rats on a defined dietproviding the then known nutrients: fats, proteins, carbohydrates, and mineral salts.The animals failed to grow, but the addition of a small amount of milk to the dietboth permitted the animals to maintain normal growth and restored growth to theanimals that had previously been fed the defined diet. He suggested that milkcontained one or more “accessory growth factors” – essential nutrients present insmall amounts, because the addition of only a small amount of milk to the diet wassufficient to maintain normal growth and development. The first of the accessoryfood factors to be isolated and identified was found to be chemically an amine;therefore, in 1912, Funk coined the term vitamine, from the Latin vita for “life”and amine, for the prominent chemical reactive group. Although subsequentaccessory growth factors were not found to be amines, the name has been retained–with the loss of the final “-e” to avoid chemical confusion. The decision as towhether the word should correctly be pronounced “vitamin” or “veitamin” dependsin large part on which system of Latin pronunciation one learned – the OxfordEnglish Dictionary permits both. During the first half of the twentieth century,vitamin deficiency diseases were common in developed and developing countries.At the beginning of the twenty-first century, they are generally rare, althoughvitamin A deficiency is a major public health problem throughout the developingworld, and there is evidence of widespread subclinical deficiencies of vitamins B2and B6. In addition, refugee and displaced populations are at risk of multiple Bvitamin deficiencies, because the cereal foods used in emergency rations are notusually fortified with micronutrients.5
Vitamins are grouped together according to the following general biologicalcharacteristics:1. Vitamins are not synthesized by the body and must come from food. Anexception are vitamin B3 (PP), which active form NADH (NADPH) can besynthesized from tryptophan and vitamin D3 (cholecalciferol), synthesized from 7dehydrocholesterol in the skin. Amount of those ones and vitamins partiallysynthesized by intestinal microflora (В1, В2, В3, B5, В6, К, and others) is normallynot sufficient to cover the body's need them.2. Vitamins are not plastic material. Exception is vitamin F.3. Vitamins are not an energy source. Exception is vitamin F.4. Vitamins are essential for all vital processes and biologically activealready in small quantities.5. They influence biochemical processes in all tissues and organs, i.e. theyare not specific to organs.6. They can be used for medicinal purposes as a non-specific tools in highdoses for: diabetes mellitus - B1, B2, B6; colds and infectious diseases - vitamin C;bronchial asthma - vitamin PP; gastrointestinal ulcers - vitamin-like substance Uand nicotinic acid; in hypercholesterolemia - nicotinic acid.Since only a few vitamins can be stored (A, D, E, B12), a lack of vitaminsquickly leads to deficiency diseases (hypovitaminosis or avitaminosis). Theseoften affect the skin, blood cells, and nervous system. The causes of vitamindeficiencies can be treated by improving nutrition and by administration vitaminsin tablet form. An overdose of vitamins leads to hypervitaminosis state only, withtoxic symptoms, in the case of vitamins A and D. Normally, excess vitamins arerapidly excreted with the urine.Lack of vitamins leads to the development of pathological processes in theform of specific hypo- and avitaminosis. Widespread hidden forms of vitamindeficiency have not severe external manifestations and symptoms, but have anegative impact on performance, the overall tone of the body and its resistance tovarious adverse factors.6
Avitaminosis is a disease that develops in the absence of a particular vitamin.Currently avitaminosis are not commonly found, but hypovitaminoses are observedwith vitamin deficiency in the body. Numerous examples you can see in the table 1.Table 1. Vitamin functions and manifestations of hypo- and ridoxine,pyridoxal,pyridoxamineB7(H)BiotinB9Folic acidFunctionsFunctionalpartofcoenzyme TPP in olase;poorlydefined function in nerveconductionFunctionalpartofcoenzymes FAD, FMN zymes NAD , NADP zyme CoA (universalacyl carrier in Krebs cycle,fatty and other carboxylicacidmetabolism)andphosphopantetheine (acylcarrier protein in fatty inationanddecarboxylation of aminoacidsandglycogenphosphorylaseCoenzyme in carboxylationreactionsingluconeogenesis and fattyacid synthesisHypovitaminosis symptomesPeripheral nerve damage (polyneuritisberiberi) or central nervous system lesions(Wernicke-Korsakoff syndrome)Concentration of pyruvate is increased in thepatient's blood, the most of which is excretedwith urineEpithelial, mucosa, cutaneous, corneallesions: lesions of corner of mouth, lips, andtongue; seborrheic dermatitisPellagra: photosensitive dermatitis, glossitis(tongue inflammation), alopecia (hair loss),edema (swelling), diarrhea, depressivepsychosis, aggression, ataxia (lack ofcoordination), dementia, weaknessNumbness in the toes, burning sensation inthe feet, the defeat of mucous membranes ofinternal organs, early graying, hair loss,various disorders of the skin: thedevelopment of small cracks in the corners ofthe mouth, the appearance of white patcheson various parts of the body. There may alsobe depressed mood, fatigue.Dermatitis of the eyes, nose, and mouth.There is mental confusion, glossitis andperipheral neuropathy, convulsions (due tolack of inhibitory neurotransmitter GABA)Seborrheic dermatitis, anemia, depression,hair loss, high blood sugar levels,inflammation or pallor of the skin andmucous membranes, insomnia, loss ofappetite, muscle aches, nausea, sore tongue,dry skin, high blood cholesterolFunctionalpartof Megaloblastic anemia: red tongue, anemia,coenzyme THFA in transfer lethargy, fatigue, insomnia, anxiety, digestiveof one-carbon fragmentsdisorders, growth retardation, breathingdifficulties, memory problems.Deficiency during pregnancy is associatedwith neural tube defects7
ymesadenosylcobalamin(Methylmalonyl Co Amutase)andmethylcobalamin(Methionine synthase) intransfer of one-carbonfragments and metabolismof folic acidIt serves as a donor ofprotons in hydroxylationreaction for:- collagen synthesis (prolyland lysyl residues arehydroxylated by prolyl3(4)-hydroxylase and lysyl5-hydroxylase respectively;catecholaminesandsteroid hormone orption of ironRetinolFunctional part of visualpigments (rhodopsins andiodopsins) in the ation; β-carotene(provitamin A) is anantioxidantCalciferol StimulationofCa2 absorptionthroughintestinal wall, maintenanceof calcium balance andmobilizationofbonemineralTocopherols Antioxidant, especially incell membranesPhylloCoenzyme in formation ofquinone, γ-carboxyglutamatemenaresidues in structure of:quinones - factors II (prothrombin),VII, IX, X, XIV, protein S(blood coagulation system);- bone matrix proteins8Vitamin B12-deficiency anemia (in otherwords pernicious anemia or Addison–Biermer anemia) is one of many types ofmegaloblastic anemias with degeneration ofthe spinal cord, anemia, fatigue, depression,low-grade fevers, diarrhea, weight loss,neuropathic pain, glossitis (swollen, red andsmooth appearance of the tongue), angularcheilitis (sores at the corner of the mouth)Possible manifestations are also hypochromicanemia, splitting hair and loss of hair,increased nail bottling and taste alterationScurvy: general weakness, subcutaneoushemmorhages (frequent hemorrhages frominternals and mucous membranes), gingivalhemmorhages, loss of teeth, formation ofspots on the skin, spongy gums, yellow skin,fever, neuropathyMultiple hemorrages in the places of clothesfriction are possible if a person oftenexperiences acute respiratory infectionsVision impairment hemeralopia (nightblindness), xerophthalmia; keratinization ofskinRickets poor mineralization of bone;osteomalacia bone demineralizationOsteoectasia of the lower extremities anddelayed mineralization of cranial bones areonserved in infantsExtremely rare is a serious neurologicdysfunctionImpaired blood clotting, hemorrhagicdisease, osteoporosis and coronary heartdiseaseIntestinal dysbacteriosis occurs hemorrhagicsyndrome
External causes for hypovitaminosis1. Lack of the vitamin in the diet or presence of food factors hindering theabsorption of vitamin. For example, use of large amounts of raw eggs (they containprotein avidin binds vitamin H (biotin)) as a result may develop a state ofhypovitaminosis H.2. Do not take into account the need for a particular vitamin. For example, inprotein-free diet is increasing demand for vitamin PP (with normal diet it may bepartially synthesized from tryptophan). If a person consumes much protein, it canincrease the need for vitamin B6 and reduce the need for vitamin PP.3. Social reasons: urbanization, power and extremely high purity of cannedfood; antivitamin presence in food. People are not enough exposed to sunlight inlarge cities - so it can be hypovitaminosis D. In such cases, the medicine usesultraviolet radiation in the form of different physical treatments, which activate thesynthesis of vitamin D3 from 7-dehydrocholesterol in the skin cells.Internal causes of hypovitaminosis1. Physiological increased need for vitamins, for example, during pregnancy,with heavy physical labor.2. Long-term severe infectious diseases, as well as during the recoveryperiod.3. Disturbance of vitamin absorption in some diseases of the digestive tract,for example impaired absorption of fat-soluble vitamins is observed atcholelithiasis; vitamin B12 is done with atrophy of the gastric mucosa and adeficiency of Castle intrinsic factor. Another case if a person who hadn’t beenconsuming fats but had been getting enough carbohydrates and proteins for longtime revealed dermatitis, poor wound healing, vision impairment. Lack of vitaminsA, D, E, K, F (linoleic, linolenic, arachidonic acids) is probable cause of themetabolic disorder.4. Intestinal dysbacteriosis. It has the meaning as some vitamins aresynthesized by the intestinal microflora (these vitamins are B3, B6, B7 (H), B9, B12,and K).9
5. Cirrhosis. The liver is the major depot of many vitamins, particularly fatsoluble (especially high hepatic reserves of fat soluble vitamins A, D), but alsocertain water-soluble, such as B9, B12, etc. In case of vitamin consumption increaseand reducing their dietary intake, which is usually the case, for example, inalcoholism, megaloblastic anemia is developed in a short time as a characteristicsign of hypovitaminosis B9. Patients with cirrhosis may experience blurred visionin the twilight due to malabsorption of vitamin A in the intestine and its reduceddeposit in the liver.6. Genetic defects of some enzymatic systems. For example, vitamin Dresistant rickets occurs in children lack the enzymes involved in the formation ofthe active form of vitamin D - calcitriol (1, 25-dihydroxycholecalciferol).CLASSIFICATION AND NOMENCLATURE OF THE VITAMINSIn addition to systematic chemical nomenclature, the vitamins have anapparently illogical system of accepted trivial names arising from the history oftheir discovery. For several vitamins, a number of chemically related compoundsshow the same biological activity, because they are either converted to the samefinal active metabolite or have sufficient structural similarity to have the sameactivity. Different chemical compounds that show the same biological activity arecollectively known as vitamers. Where one or more compounds have biologicalactivity, in addition to individual names there is also an approved genericdescriptor to be used for all related compounds that show the same biologicalactivity.When it was realized that milk contained more than one accessory foodfactor, they were named A (which was lipid-soluble and found in the cream) and B(which was water-soluble and found in the whey). This division into fat- andwater-soluble vitamins is still used, although there is little chemical or nutritionalreason for this, apart from some similarities in dietary sources of fat-soluble orwater-soluble vitamins. Water-soluble derivatives of vitamins A and K and fat-10
soluble derivatives of several of the B vitamins and vitamin C have been developedfor therapeutic use and as food additives.As the discovery of the vitamins progressed, it was realized that “Factor B”consisted of a number of chemically and physiologically distinct compounds.Before they were identified chemically, they were given a logical series ofalphanumeric names: B1, B2, and so forth.Table 2. Classification of vitamins. Group B.Alphanumeric name ofChemical and other names of vitaminvitaminVitamin B1thiamineVitamin B2riboflavinVitamin B3niacin, niacinamide, niacin, niacinamide, RRVitamin B4cholineVitamin B5pantothenic acidVitamin B6pyridoxine, pyridoxalVitamin B7biotin, vitamin HVitamin B8inositol, myo-inositol, vitamin UVitamin B9folic acid, foliatsin, vitamin BC, MVitamin B10para-aminobenzoic acid, PABA, vitamin H1Vitamin B11L-carnitine, vitamin T, vitamin DVitamin B12cyanocobalamin, cobalaminVitamin B13orotic acidVitamin B14pyrrolo-quinoline quinone, metoksantin, coenzyme ofPQQ (Pyrroloquinoline Quinone)Vitamin B15pangamic acid, sometimes referred to as vitamin B16Vitamin B16sometimes pangamic acid - B15, and sometimescyanocobalamin - B12Vitamin B17 (misnomer)L-citral, letral, letril, amygdalin (The structure - a2glucose mandelonitrile)11
And such vitamins or vitamin similar compounds as:Vitamin C - ascorbic acid;Vitamin P - bioflavonoids: quercetin, rutin, myricetin, apigenin, hesperin,hesperidin, luteolin, catechin, eriodictyol, cyaniding and others;Vitamin N - lipoic acid;Vitamin U (ulcus - ulcer) - a derivative of methionine-methionine-methylsulfonium (pharmacology known as "metiosulfoniya chloride")As can be seen from Table 2, a number of compounds were assigned vitaminstatus, and were later shown either not to be vitamins, or to be compounds that hadalready been identified and given other names.For a compound to be considered a vitamin, it must be shown to be a dietaryessential. Its elimination from the diet must result in a more-or-less clearly defineddeficiency disease, and restoration must cure or prevent that deficiency disease.Demonstrating that a compound has pharmacological actions, and possibly cures adisease, does not classify that compound as a vitamin, even if it is a naturallyoccurring compound that is found in foods. Equally, demonstrating that acompound has a physiological function as a coenzyme or hormone does notclassify that compound as a vitamin. It is necessary to demonstrate thatendogenous synthesis of the compound is inadequate to meet physiologicalrequirements in the absence of a dietary source of the compound. There is someevidence that premature infants and patients maintained on long-term totalparenteral nutrition may be unable to meet their requirements for carnitine, choline,and taurine unless they are provided in the diet, and these are sometimes regardedas “marginal compounds,” for which there is no evidence to estimate requirements.The rigorous criteria outlined here would exclude niacin and vitamin D fromthe list of vitamins, because under normal conditions endogenous synthesis doesindeed meet requirements. Nevertheless, they are considered to be vitamins, evenif only on the grounds that each was discovered as the result of investigations intoonce common deficiency diseases, pellagra and rickets.12
In addition to the marginal compounds like carnitine choline, there are anumber of compounds present in foods of plant origin that are considered to bebeneficial, in that they have actions that may prevent the development ofatherosclerosis and some cancers, although there is no evidence that they aredietary essentials, and they are not generally considered as nutrients.GROUP I. FAT-SOLUBLE VITAMINSGroup I is Fat-soluble vitamins: A (retinol), D (calciferol), E (tocopherol), K(naphthoquinone), F (polyunsaturated fatty acid: linoleic, linolenic, arachidonic).VITAMIN AVitamin A includes two vitamers: retinol and dehydroretinol but group ofvitamin A consists and their biologically active molecules retinal (retinaldehyde)and retinoic c Acid13
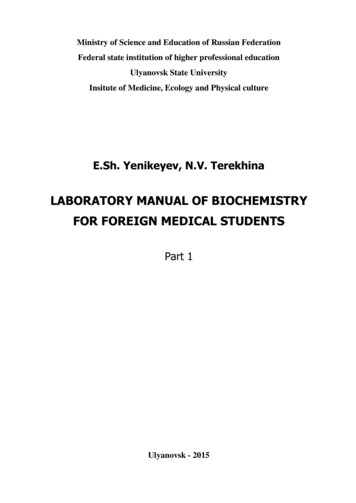
Each of these compounds are derived from the plant produced moleculecarotene (a member of a family of molecules known as carotenoids). Beta-carotenestructure:Beta-carotene, which consists of two molecules of retinal linked at theiraldehyde ends, is also referred to as the provitamin form of vitamin A.Ingested β-carotene is cleaved in the lumen of the intestine by beta-carotenedioxygenase to yield retinal. Retinal is right here reduced to retinol byretinaldehyde reductase, an NADPH requiring enzyme within the intestines.Retinol is esterified to palmitic or stearic acids and delivered to the blood viachylomicrons. The uptake of chylomicron remnants by the liver results in deliveryof retinol to this organ for storage as a lipid esters. Transport of retinol from theliver to extrahepatic tissues occurs by binding of retinol to retinol binding protein(RBP). the retinol-RBP complex is then transported to the cell surface within theGolgi and secreted. Within extrahepatic tissues retinol is bound to cellular retinolbinding protein (CRBP). Plasma transport of retinoic acid is accomplished bybinding to albumin. One protein else is capable to transport of vitamin A: it istransthyretin. Transthyretin (TTR) is a serum and cerebrospinal fluid carrier of thethyroid hormone thyroxine (T4) and retinol-binding protein bound to retinol. Thisis how transthyretin gained its name, transports thyroxine and retinol. The liversecretes transthyretin into the blood, and the choroid plexus secretes TTR into thecerebrospinal fluid.TTR was originally called prealbumin (or thyroxine-binding prealbumin)because it ran faster than albumin on electrophoresis gels.14
Gene Control Exerted by Retinol and Retinoic AcidWithin cells both retinol and retinoic acid bind to specific receptor proteins.Following binding, the receptor-vitamin complex interacts with specific sequencesin several genes involved in growth and differentiation and affects expression ofthese genes. In this capacity retinol and retinoic acid are considered hormones ofthe steroid/thyroid hormone superfamily of proteins. Vitamin D also acts in asimilar capacity. Several genes whose patterns of expression are altered by retinoicacid are involved in the earliest processes of embryogenesis including thedifferentiation of the three germ layers, organogenesis and limb development.Vision and the Role of Vitamin APhotoreception in the eye is the function of two specialized cell typeslocated in the retina; the rod and cone cells. Both rod and cone cells contain aphotoreceptor pigment in their membranes. The photosensitive compound of mostmammalian eyes is a protein called opsin to which is covalently coupled analdehyde of vitamin A. The opsin of rod cells is called scotopsin. Thephotoreceptor of rod cells is specifically called rhodopsin or visual purple. Thiscompound is a complex between scotopsin and the 11-cis-retinal (also called 11cis-retinene) form of vitamin A. Rhodopsin is a serpentine receptor imbedded inthe membrane of the rod cell. Coupling of 11-cis-retinal occurs at three of thetransmembrane domains of rhodopsin. Intracellularly, rhodopsin is coupled to aspecific G-protein called transducin.When the rhodopsin is exposed to light it is bleached releasing the 11-cisretinal from opsin. Absorption of photons by 11-cis-retinal triggers a series ofconformational changes on the way to conversion all-trans-retinal. One importantconformational intermediate is metarhodopsin II. The release of opsin results in aconformational change in the photoreceptor. This conformational change activatestransducin, leading to an increased GTP-binding by the α-subunit of transducin.Binding of GTP releases the α-subunit from the inhibitory β- and γ-subunits. TheGTP-activated α-subunit in turn activates an associated phosphodiesterase; an15
enzyme that hydrolyzes cGMP to GMP. cGMP is required to maintain the Na channels of the rod cell in the open conformation. The drop in cGMP concentrationresults in complete closure of the Na channels. Metarhodopsin II appears to beresponsible for initiating the closure of the channels. The closing of the channelsleads to hyperpolarization of the rod cell with concomitant propagation of nerveimpulses to the brain.Additional Role of RetinolRetinol also functions in the synthesis of certain glycoproteins andmucopolysaccharides necessary for mucous production and normal growthregulation. This is accomplished by phosphorylation of retinol to retinyl phosphatewhich then functions similarly to dolichol phosphate.Clinical Significances of Vitamin A DeficiencyVitamin A is stored in the liver and deficiency of the vitamin occurs onlyafter prolonged lack of dietary intake. The earliest symptoms of vitamin Adeficiency are night blindness. Additional early symptoms include follicularhyperkeratinosis, increased susceptibility to infection and cancer and anemiaequivalent to iron deficient anemia. Prolonged lack of vitamin A leads todeterioration of the eye tissue through progressive keratinization of the cornea, acondition known as xerophthalmia.The increased risk of cancer in vitamin deficiency is thought to be the resultof a depletion in beta-carotene. β-carotene is a very effective antioxidant and issuspected to reduce the risk of cancers known to be initiated by the production offree radicals. Of particular interest is the potential benefit of increased betacarotene intake to reduce the risk of lung cancer in smokers. However, cautionneeds to be taken when increasing the intake of any of the lipid soluble vitamins.Excess accumulation of vitamin A in the liver can lead to toxicity which manifestsas bone pain, hepatosplenomegaly, nausea and diarrhea.VITAMIN D16
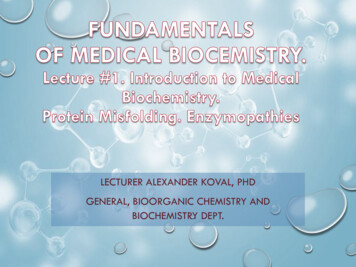
Vitamin D is a steroid hormone that functions to regulate specific geneexpression following interaction with its intracellular receptor. The biologicallyactive form of the hormone is 1,25-dihydroxy vitamin D3 (1,25-(OH)2D3, alsotermed calcitriol). Calcitriol functions primarily to regulate calcium andphosphorous homeostasis.ErgosterolVitamin D27-DehydrocholesterolVitamin D3Active calcitriol is derived from ergosterol (produced in plants) and from 7dehydrocholesterol (produced in the skin). Ergocalciferol (vitamin D2) is formedby UV (ultraviolet) irradiation of ergosterol. In the skin 7-dehydrocholesterol isconverted to cholecalciferol (vitamin D3) following UV irradiation.17
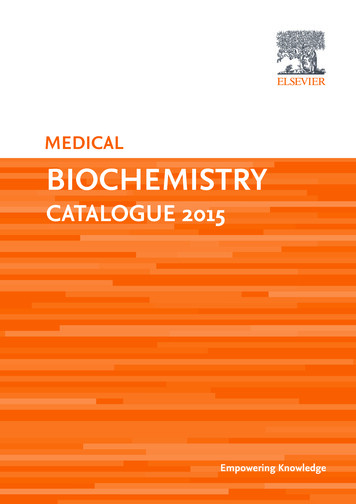
Vitamin D2 and D3 are processed to D2-calcitriol and D3-calcitriol,respectively, by the same enzymatic pathways in the body. Cholecalciferol (orergocalciferol) are absorbed from the intestine and transported to the liver bound toa specific vitamin D-binding protein. In the liver cholecalciferol is hydroxylated atthe 25 position by a specific D3-25-hydroxylase generating 25-hydroxy-D3 [25(OH)D3] which is the major circulating form of vitamin D. Conversion of 25(OH)D3 to its biologically active form, calcitriol, occurs through the activity of aspecific D3-1-hydroxylase present in the proximal convoluted tubules of thekidneys, and in bone and placenta. 25-(OH)D3 can also be hydroxylated at the 24position by a specific D3-24-hydroxylase in the kidneys, intestine, placenta andcartilage.25-hydroxyvitamin D31,25-dihydroxyvitamin D3Calcitriol functions in concert with parathyroid hormone (PTH) andcalcitonin to regulate serum calcium and phosphorous levels. PTH is released inresponse to low serum calcium and induces the production of calcitriol. In contrast,reduced levels of PTH stimulate synthesis of the inactive 24,25-(OH)2D3. In theintestinal epithelium, calcitriol functions as a steroid hormone in inducing theexpression of calbindinD28K, a protein involved in intestinal calcium absorption.The increased absorption of calcium ions requires concomitant absorption of anegatively charged counter ion to maintain electrical neutrality. The predominantcounter ion is Pi. When plasma calcium levels fall the major sites of action of18
calcitriol and PTH are bone where they stimulate bone resorption and the kidneyswhere they inhibit calcium excretion by stimulating reabsorption by the distaltubules. The role of calcitonin in calcium homeostasis is to decrease elevatedserum calcium levels by inhibiting bone resorption.Clinical Significance of Vitamin D DeficiencyAs a result of the addition of vitamin D to milk, deficiencies in this vitaminare rare in this country. The main symptom of vitamin D deficiency in children isrickets and in adults is osteomalacia. Rickets is characterized impropermineralization during the development of the bones resulting in soft bones.Osteomalacia is characterized by demineralization of previously formed boneleading to increased softness and susceptibility to fracture.VITAMIN EVitamin E is a mixture of several related compounds known as tocopherols.The α-tocopherol molecule is the most potent of the tocopherols.α-Tocopherolα-Tocopherol is the main source found in supplements and in the Europeandiet, where the main dietary sources are olive and sunflower oils, while γtocopherol is the most common form in the American diet due to a higher intake ofsoybean and corn oil.Tocotrienols, which are related compounds, also have vitamin E activity. Allof these various derivatives with vitamin activity may correctly be referred to as19
"vitamin E". Tocopherols and tocotrienols are fat-soluble antioxidants but alsoseem to have many other functions in the body.Vitamin E is absorbed from the intestines packaged in chylomicrons. It isdelivered to the tissues via chylomicron transport and then to the liver throughchylomicron remnant uptake. The liver can export vitamin E in VLDLs. Due to itslipophilic nature, vitamin E accumulates in cellular membranes, fat deposits andother circulating lipoproteins. The major site of vitamin E storage is in adiposetissue.The major function of vitamin E is to act as a natural antioxidant byscavenging free radicals and molecular oxygen. In particular vitamin E isimportant for preventing peroxidation of polyunsaturated membrane fatty acids.The vitamins E and C are interrelated in their antioxidant capabilities. Active αtocopherol can be regenerated by interaction with vitamin C following scavenge ofa peroxy free r
Biochemistry of vitamins. Textbook for students of international faculty speciality: 7.120 10001 «General Medicine» / K.V. Aleksandrova, N.P. Rudko. – Zaporizhzhya : ZSMU, 2016.- 73 p. This textbook is recommended to use for students of international faculty (the second year of study) fo