Transcription
Care of a Client with Biliary DisordersUnderstanding biliary disorders, nursing management,and prevention of complications.Kechi Iheduru-Anderson DNP, RN, CNE, CWCNCare of a client with biliary disorders.www.westafricaneducatednurses.orgJanuary 18, 2016pg. 1
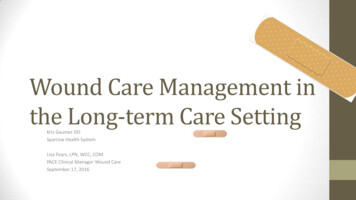
Introduction Most disorders of the biliary tract resultfrom gallstones. Gallstones in thegallbladder (Cholelithiasis) are usuallyasymptomatic. Bile flow may be blockedby gallstones in the bile ducts(choledocholithiasis) triggering biliarycolic or causing inflammation of thegallbladder (cholecystitis). Cholecystitismay be acute, developing over hours, orchronic, persisting for a long time.Gallstones can also block the flow ofdigestive enzymes from the pancreasresulting in inflammation of thepancreas (gallstone pancreatitis).Burden of gallstone diseaseGallstone disease is one of the mostcommon and costly of all digestivediseases. More than 20 million personshave gallbladder disease in the UnitedStates. The direct and indirect cost ofgallbladder disease represents aconsumption of 6.2 billion annually inthe U.S., constituting a major healthburden that has increased more than20% over the last 3 decades. With anestimated 1.8 million ambulatory carevisits each year, gallstone disease is aleading cause for hospital admissionsrelated to gastrointestinal problems. themortality rate for gallstones disease isrelatively low at 0.6%.Learning objectives Identify the common causes ofcholecystitis and cholelithiasis(gallbladder disease).Care of a client with biliary disorders. Differentiate the symptoms of acutecholecystitis from chroniccholecystitisDiscuss the management of acutecholecystitisDevelop a postoperative plan of carefor clients undergoingcholecystectomy.Structure and Functions of thebiliary tractThe biliary tract consists of smalltubes (ducts) that carry bile from theliver to the gallbladder and then to thesmall intestine. The gallbladder is asmall, pear-shaped sac located beneaththe liver.Bile has two main functions:aiding in digestion and eliminatingcertain waste products (mainlyhemoglobin and excess cholesterol)from the body. Bile salts aid in digestionby making cholesterol, fats, and fatsoluble vitamins easier to absorb fromthe intestine. The main pigment in bile,bilirubin, is a waste product that isformed from hemoglobin (the proteinthat carries oxygen in the blood) and isexcreted in bile. Hemoglobin is releasedwhen old or damaged red blood cellsare destroyed.Bile flows out of the liver throughthe left and right hepatic ducts, whichcome together to form the commonhepatic duct. This duct then joins with aduct connected to the gallbladder, calledthe cystic duct, to form the common bilewww.westafricaneducatednurses.orgJanuary 18, 2016pg. 2
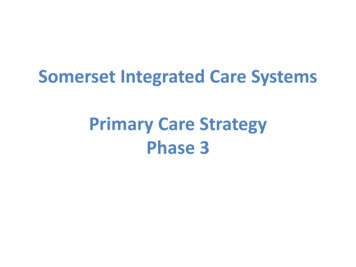
duct. The common bile duct enters thesmall intestine at the sphincter of Oddi(a ring-shaped muscle), located a fewinches below the stomach. About halfthe bile secreted between meals flowsdirectly through the common bile ductreabsorbed into the bloodstreamthrough the wall of the lower smallintestine, the rest are broken down bybacteria in the large intestine. Some arereabsorbed in the large intestine and therest excreted in stool. Bile flow can beblocked or slowed(cholestasis) bytumors. Cholestasiscan also lead toinflammation,fibrosis, andstrictures of the bileducts Figure 1: The Gallbladder.into the small intestine. The rest of thebile is diverted through the cystic ductinto the gallbladder to be stored. In thegallbladder, up to 90% of the water inbile is absorbed into the bloodstream,making the remaining bile veryconcentrated.Eating releases gut hormones andstimulates cholinergic nerves, causingthe gallbladder to contract and thesphincter of Oddi to relax. Bile thenflows from the gallbladder into thesmall intestine to mix with foodcontents and perform its digestivefunctions. About 90% of bile salts areCare of a client with biliary disorders.Cholelithiasisis the presence ofone or more calculi(gallstones) in the gallbladder.Gallstones are collections of cholesterol,bile pigment or a combination of thetwo, which can form in the gallbladderor within the bile ducts of the liver. Inthe United States, the most commontype of gallstones are made ofcholesterol.Risk factors for GallstonesFemale gender, older age, familyhistory, obesity, high blood cholesterollevels, drugs such as estrogencontaining medications, ceftriaxone, andthiazide diuretics, rapid weight loss,total parenteral nutrition or fasting, sedentarylifestyle, gallbladder diabetes andpregnancy are all risk factors forwww.westafricaneducatednurses.orgJanuary 18, 2016pg. 3
developing cholesterol gallstones.Disorders that lead to the destruction ofred blood cells such as sickle cell anemiaare associated with the development ofpigmented or bilirubin stones. Theoccurrence of gallstones varies widelyamong different ethnic groups.quadrant abdominal pain, nauseaor vomiting occur.The location, duration and“character” (stabbing, gnawing,cramping) of the pain help todetermine the likelihood ofgallstoneThere are no laboratorydisease.tests specific forAbdominalgallbladder disease.tendernessElavated serum levels ofandalkaline phosphatase,abnormallyaspartateaminotransferase (AST),high liverand lactatefunctiondehydrogenase (LDH)blood testsindicates abnormalitiesmay bein liverpresent.An abdominal ultrasound is mostoften used as a quick, sensitive,and relatively inexpensivemethod of detecting gallstones inthe gallbladder or common bileduct.Calcified gallstones are easilyvisualized on abdominal x-rayexamination.Endoscopic retrogradecholangiopancreatography(ERCP).Symptoms GallstonesGallstones in the gallbladder areusually asymptomatic and requires notreatment. The most common symptomis biliary colic. Symptoms arise when agallstone blocks the flow of bile out ofthe gallbladder or through the bileducts. Choledocholithiasis (gallstone inthe common bile duct) may causeintermittent or constant discomfort.Pain localized in the upperabdomen, which may radiate to theright shoulder, may last from 30minutes to hours.May be associated with sweating,nausea, vomiting.Gallstone attacks can produce chestpain that may feel like a heart attack.Gallstones do not cause dyspepsiaor fatty food intolerance.An inflamed gallbladder(cholecystitis), infected materialtrapped within the common bileduct (cholangitis), or gallstonepancreatitis can result in fever, chills,severe abdominal pain or jaundice.DiagnosisTreatmentNonsurgical Management. Gallstones is suspected whensymptoms of right upperCare of a client with biliary matic stones are usuallymanaged conservatively with nomedical or surgical intervention.Acute pain occurs when thegallstones partially or totallyobstruct the cystic or common bileduct.January 18, 2016pg. 4
Measures aimed at resting theinflamed gallbladder are the same asthose discussed for cholecystitisbelow.Diet Therapyo The client must adhere to alow-fat diet to prevent furtherpain of biliary colic.o Replacement of fat-solublevitamins (such as vitamins A,D, E, and K) and theadministration of bile salts tofacilitate digestion andvitamin absorption may beordered if gallstone is causingobstruction of bile flow.o NPO for nausea andvomiting.Endoscopic retrogradecholangiopancreatography (ERCP) orsurgery is used for the treatment ofcholedocholithiasis.Pain management: Meperidine hydrochloride (Demerol)IV is usually given for biliary colic.Antispasmodic or anticholinergicdrugs, such as dicyclominehydrochloride (Bentyl), may begiven to relax smooth muscles anddecrease ductal tone and spasm.Antiemetics to control nausea andOlder clients should not be given Demerol, since itcan cause acute confusion and nausea. vomiting.Bile acid therapy dissolvinggall-stones, depending on the type ofstones.Care of a client with biliary disorders. o This treatment is generallyreserved for older adults whohave mild or asymptomaticgallstone disease and thosewho are poor surgical risks.May take up to 2 years todissolve gallstones.Adherence to therapy may bea problem for patients.Severe pruritus doe to jaundice maybe treated with Cholestyramine resin(Questran) binds with bile acids inthe intestine, forming an insolublecompound that is excreted in thefeces.o Instruct client to mix thepowder form of the drug withfruit juices or milk. It shouldbe taken before meals and atbedtime.Extracorporeal Shock WaveLithotripsy.Extracorporeal shockExtracorporealwave lithotripsy isshock wave lithotripsycontraindicated inis a noninvasiveclientswith liver orproce-dure that is usedpancreatic disease,for ambulatoryclients withtreatment of clientspacemakers andwith gall-stones inpregnant women.some settings. Amachine-a lithotriptor-generatespowerful shock waves to shatter thegallstones.IV conscious sedation withfentanyl citrate (Alfenta, Sublimaze) ormidazolam hydrochloride (Versed) maybe used to minimize pain and help theclient tolerate the procedure better.www.westafricaneducatednurses.orgJanuary 18, 2016pg. 5
Percutaneous Transhepatic BiliaryCatheter InsertionMay be done under fluoroscopicguidance. This procedure decompressesobstructed extrahepatic ducts so thatbile can flow.usually due to obstruction of the cysticduct by a gallstone. Acute cholecystitisis the most common complication ofcholelithiasis.Pathophysiology of Acute cholecystitisWhen a gallstone becomesSurgical managementimpacted in the cystic duct andpersistently obstructs it, acuteCholecystectomy: Symptomaticinflammation results. Bile stasis triggersclients require treatment, andrelease of inflammatory enzymes Bilelaparoscopic cholecystectomy is thestasis triggers release of inflammatoryaccepted first-line therapy (discussedenzymes. The damaged mucosa secretesbelow).more fluid into the gallbladder lumenthan it absorbs.CholecystitisIn the elderly, symptoms ofThe resultingcholecystitis may beInflammation of the gallbladder wall.distention furthernonspecific(eg, anorexia,May be acute or chronic.releasesvomiting, malaise,inflammatoryEtiologyweakness), and fever maymediators (e.g.be absent.The exact etiology of cholecystitisprostaglandins),is unknown. In addition to theworsening mucosal damage andformation of gallbladder calculi, causescausing ischemia, all of whichof acute cholecystitis include severeperpetuate inflammation. Bacterialacute illness and tumor.infection can supervene. The viciouscircle of fluid secretion andRisk factors include:inflammation, when unchecked, leads to Being femalenecrosis and perforation. If acute Pregnancyinflammation resolves then Hormone therapycontinues to recur, theAcute acalculous cholecystitis is Older agegallbladder becomescholecystitis without stones. It Obesityaccounts for 5 to 10% of allfibrotic and contracted and Rapid weight losscholecystitis. Commonly seen indoes not concentrate bile oror gaincritically ill patients or long termempty normally—features DiabetesTPN therapy. Symptoms areof chronic cholecystitis.Acute Cholecystitissimilar to those of acutecholecystitisAcutecholecystitis is inflammation of thegallbladder that develops over hours,Care of a client with biliary disorders.Symptoms of gJanuary 18, 2016pg. 6
Symptoms include; right upperquadrant pain and tenderness, (Painmay radiate to the right shoulder orback) sometimes accompanied by fever,chills, nausea, and vomiting. With rightsubcostal palpation, pain increases withdeep inspiration (Murphy's sign). Paintriggered by high fat or high volumemeal. There are no laboratory tests specificfor gallbladder disease. Acutecholecystitis is suspected based onsymptoms and signs.Abdominal ultrasonography detectsthe gallstone and sometimes theassociated inflammation. It is safe,accurate, and painless.Abdominal CT identifiescomplications such as gallbladderperforation or pancreatitis.Elevated lipase suggest bile ductobstruction.Elevated WBC indicateinflammation.Direct (conjugated) and indirect(unconjugated) serum bilirubinlevels are elevated if an obstructiveprocess is present. Serum and urine amylase levels areelevated if there is pancreaticinvolvementTreatment and InterventionsNonsurgical treatment measuresprescribed during the acute phase ofcholecystitis are directed at resting theinflamed gall-bladder in an effort toreduce the inflammatory process andIn chronic cholecystitis, clientsrelieve the pain. Acute cholecystitis ismay have insidious symptoms and maygenerally managed surgically because ofnot seek medical treatmentthe risk of sepsis anduntil late symptoms suchMorphine is generally not given inperforation. Acutethe management of cholecystitisas jaundice, clay-coloredcholecystitis begins topain, because it can cause spasmsstools, and dark urinesubside in 2 to 3 days andof the sphincter of Oddi andre-sult from anincrease pain.resolves within 1 wk. inobstructive process.85% of patients evenwithout treatment.Diagnosis Care of a client with biliary disorders. www.westafricaneducatednurses.orgWithholding food and fluids ormodifying the diet by avoiding highfat or high-volume meals. Thesedietary measures decreasestimulation of the gallbladder andhelp prevent pain, nausea, andvomiting.A nasogastric tube is inserted toempty the stomach contents inpatients with severe nausea andvomiting.Antiemetics such astrimethobenzamide hydrochloride(Tigan), to relieve nausea andvomiting.IV fluids,antibiotics, and analgesics;Cholecystectomy is done whenpatients are stable.January 18, 2016pg. 7
Pain management: severe painopioid analgesics, such asmeperidine hydrochloride(Demerol), to relieve abdominal painand spasm.Antispasmodic agents, such asanticholinergics (e.g., dicyclominehydrochloride [Bentyl, Lomine ),may be used to relax the smoothmuscles, preventing biliarycontraction.Cholecystectomy: The usual surgicaltreatment of clients with acute andchronic cholecystitis ischolecystectomy, the removal of thegallbladder.Complications
of chronic cholecystitis. cholecystitis Symptoms of Acute Cholecystitis In the elderly, symptoms of cholecystitis may be nonspecific (eg, anorexia, vomiting, malaise, weakness), and fever may be absent. Acute acalculous cholecystitis is cholecystitis without stones. It accounts for 5 to 10% of all cholecystitis. Commonly seen in