Transcription
Quality DepartmentGuidelines for Clinical CareAmbulatoryPrenatal CarePrenatal Care GuidelineTeamTeam LeaderPatient population: Women of childbearing age, pregnant women, and their fetuses.Mark C. Chames, MDObstetrics / GynecologyObjectives: (1) Promote maternal and infant health.Team MembersJoanne M. Bailey, CNM,PhDObstetrics / GynecologyGrant M. Greenberg, MD,MA, MHSAFamily MedicineR. Van Harrison, PhDMedical EducationJocelyn H. Schiller, MDPediatricsConsultantChrista B. Williams, MDFamily MedicineInitial ReleaseDecember 2013Interim/Minor RevisionOctober 2015January 2019UMHS GuidelinesOversight TeamKarl T. Rew, MDR. Van Harrison, PhDLiterature search serviceTaubman Health SciencesLibraryFor more r/clinical-care-guidelines Regents of theUniversity of MichiganThese guidelines should not beconstrued as including all propermethods of care or excludingother acceptable methods of carereasonably directed to obtainingthe same results. The ultimatejudgment regarding any specificclinical procedure or treatmentmust be made by the physician inlight of the circumstancespresented by the patient.Key Points:(2) Reduce maternal mortality and morbidity and fetal loss.(3) Reduce preterm birth, intrauterine growth restriction, congenital anomalies, andfailure to thrive.Prenatal care summary. Table 1 summarizes the main aspects of prenatal care from preconceptionthrough delivery (history and examination; testing and treatment; education and planning).Fetal surveillance. Table 2 shows the common indications for antepartum fetal surveillance withnonstress testing and amniotic fluid index (AFI), the gestational ages at which to initiate testing, andthe frequency of testing.Referral. Table 3 summarizes the indications for referral.Important care aspects:Assess risk factors. For all women, perform a history and physical that includes a risk assessment with agoal of identifying risk factors for adverse pregnancy outcome [I-D]. Review the patient’s medicalhistory and any prior pregnancy and delivery records. Clearly document risk factors and add them tothe patient’s problem list.-Screen for tuberculosis in pregnant women at high risk for TB.-Refer hepatitis B carriers to hepatology due to their long term risk for cancer and cirrhosis.-Screen all patients for depression during the third trimester.-Provide contraceptive counseling during the third trimester teaching.-Review future chronic disease risks with patients during pregnancy and at the postpartum visit.Progesterone therapy. Progesterone should be offered to patients who have a history of prior spontaneouspreterm birth or who are found to have a shortened cervix on ultrasound [I-A].STI testing. Test all women for sexually transmitted infections, including HIV. Patients at risk for STIsduring pregnancy should be retested in the third trimester [I-A].Estimated date of delivery (EDD). Establish a patient’s EDD prior to 20 weeks, with consideration givento menstrual history, mode of conception, and sonographic findings using standardized criteria (seepage 14) [I-C].Tdap vaccination. Offer Tdap vaccination to all women. Administering Tdap at 27-36 weeks facilitatespassive pertussis immunization of newborns [I-D], and administering it around 32 weeks mayoptimize maternal antibody formation peaking at normal time of delivery.No non-medically-indicated delivery 39 weeks. Non-medically-indicated planned delivery before 39weeks’ gestation is contraindicated [III-B].* Strength of recommendation:I generally should be performed; II may be reasonable to perform; III generally should not be performed.Level of evidence supporting a diagnostic method or an intervention:A randomized controlled trials; B controlled trials, no randomization; C observational trials; D opinion of expert panelClinical BackgroundManagement IssuesWomen who receive prenatal care during the first (1) Early and continuing risk assessmenttrimester have better pregnancy outcomes than (2) Health promotionwomen who have little or no prenatal care. Expert (3) Medical and psychosocial interventions andfollow-uppanels on the content of prenatal care haveEachofthese three components is reflected in thisidentified the following three basic components:guideline. (Continued on page 5)1
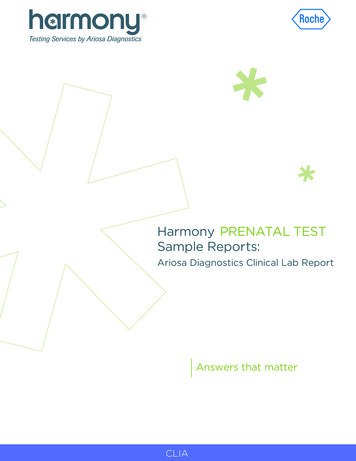
Table 1. Guidelines for Prenatal Care*GestationalAgeHistory and ExaminationPreconception Medical history including menstrual,sexual, immunization, infectious- 12 weeksexposure and riskObstetrical historyFamily and genetic historyPsychosocial history includingtobacco, alcohol, drugs,employment, and nutritionDepression screenIntimate partner violence (IPV)screenCurrent pregnancy symptomsComplete physical exam includingheight, weight, BMI, bloodpressure, and pelvic examination †Testing and TreatmentEducation and PlanningBlood type and Antibody ScreenHemoglobin / Hematocrit / PlateletcountRubella titer (vaccinate beforeconception †)Hepatitis B Surface AntigenHIVSTI screening (Gonorrhea,Chlamydia, Syphilis)Urine culture at first prenatal visitCervical cancer screening †Cystic fibrosis (CF) carrierscreeningScreening for spinal muscularatrophy (SMA)Hemoglobin electrophoresis †Other genetic screening (TaySachs, etc.) †Diabetes testing †Varicella titer (vaccinate beforeconception) †Hepatitis C testing †Tuberculosis testing †Aneuploidy screening†Influenza vaccination †Counsel on significant positivefindings elicited by history,physical, or test resultsReview test results if availableReview dating criteria †Screen for aneuploidyDiscuss:-Nutrition in pregnancy (includingrecommendations for folate andcalcium, and cautions regardingmercury in fish and pathogens inuncooked or unpasteurized foods)-Weight gain in pregnancy-Work related exposures or risks-Recent or planned travel withregard to Zika and other infectiousdisease risks or exposures-Breastfeeding-VBAC/TOLAC †Provide obesity counseling †Refer for genetic counseling †Refer to a high-risk provider †12-16 weeksCurrent pregnancy symptomsInterim medical, psychosocial, andnutritional evaluationWeight and blood pressureFetal heart rateAneuploidy screen †Diabetes screening at 12 weeks †Influenza vaccination †Review test resultsDiscuss:-Physical changes-Safe sex and sexuality duringpregnancy-Exercise and fitness duringpregnancy-Managing work during pregnancy-Seatbelt use in pregnancy16-22 weeksCurrent pregnancy symptomsInterim medical, psychosocial, andnutritional evaluationWeight and blood pressureFetal assessment including fetal heartrate and growthUltrasoundProgesterone for prevention ofrecurrent preterm birth †Influenza vaccination †Review test resultsReview dating criteriaDiscuss-Signs of complications, includingpreterm labor and preeclampsia-Childbirth classes-Common discomforts inpregnancy-Emotional changes in pregnancy-Trauma protocol in pregnancyProvide directions to the BirthCenter2UMHS Prenatal Care Guideline, September 2018
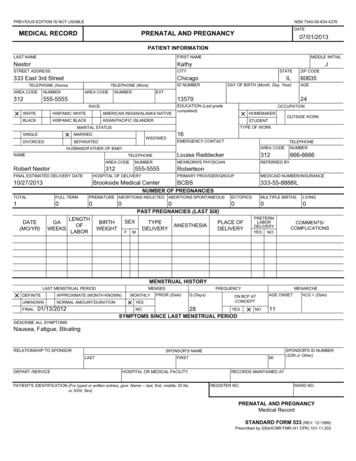
Table 1. Guidelines for Prenatal Care* (Continued)GestationalAgeHistory and ExaminationTesting and TreatmentPlanning and Education22-28 weeksCurrent pregnancy symptomsInterim medical, psychosocial, andnutritional evaluationWeight and blood pressureFetal assessment including fetal heartrate and growthDiabetes screening at 24-28 weeksHemoglobin / Hematocrit / Plateletcount at 24-28 weeks †Antibody Screen at 24-28 weeks inRh negative women †Influenza vaccination †Review test resultsDiscuss:-Signs of complications includingpreterm labor and preeclampsia-Parenting, infant classes-Breastfeeding classes-Contraception and familyplanning-Family adjustment-Work plans-Diet and nutrition in pregnancy-VBAC/TOLAC †28-34 weeksCurrent pregnancy symptomsInterim medical, psychosocial, andnutritional evaluationDepression screenIPV screenWeight and blood pressureFetal assessment including fetal heartrate and growthTdap vaccination at 27-36 weeksRhoD Immune Globulin (Rhogam)given at 28-29 weeks in Rhnegative women †Influenza vaccination †Nonstress testing after 32 weeks †Review test resultsDiscuss fetal movement monitoringProvide anticipatory guidanceregarding labor and deliveryDiscuss contraception and familyplanningIdentify a newborn care providerProvide car seat information34-38 weeksCurrent pregnancy symptomsInterim medical, psychosocial, andnutritional evaluationWeight and blood pressureFetal assessment including fetal heartrate, growth, and lie (use ofultrasound to document lie isindicated if uncertain by Leopold'smaneuvers or sterile vaginal exam)Anogenital culture for Group BStreptococcus (GBS) at 35-37weeks (unless already GBSpositive in urine during currentpregnancy or prior history of aGBS-affected infant)Nonstress testing †HIV and STI screening(Gonorrhea, Chlamydia,Syphilis) repeated in high-riskpatients †Acyclovir for women with HSV †Influenza vaccination †Review test resultsReview signs of laborDiscuss:-Infant safety after birth-Caring for self and infant afterdelivery-Parenting issues including returnto work, breastmilk collection andstorage, childcare38 weeks deliveryCurrent pregnancy symptomsInterim medical, psychosocial, andnutritional evaluationWeight and blood pressureFetal assessment including fetal heartrate, growth, and lieOffer membrane sweepingDelivery by 41-42 weeks (electivedelivery prior to 39 weeks iscontraindicated)Nonstress testing †Influenza vaccination †Review test resultsReview dating criteriaReview signs of laborInfluenza vaccination †MMR and varicella vaccinations †Cervical cancer screening †Diabetes test †Discuss:-Contraceptive initiation-Future pregnancy planning†-Future chronic disease risk†-Healthy lifestylePostpartum Blood pressureDepression screenvisit (at 4to 8 weeks) IPV screenBreastfeedingBleedingLaceration healingPelvic floor recovery* The items listed comprise a broad list of general topics to be covered, and may be based on evidence of varying quality, includingexpert opinion. Some topics may not be relevant for some individuals, while some clinical scenarios may prompt additional evaluationor education that is not listed here. Emphasize items that are most relevant for your patient.† These items should be performed when indicated by the clinical scenario.3UMHS Prenatal Care Guideline, September 2018
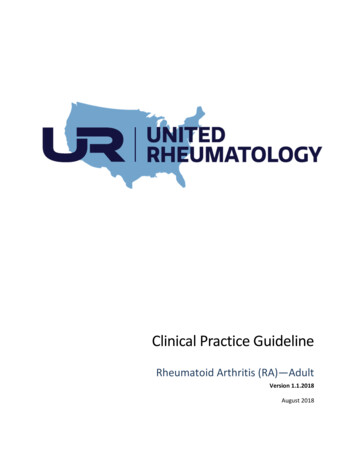
Table 2. Common Indications for Fetal Surveillance with Nonstress Test and Amniotic Fluid IndexDiagnosisAdvanced maternal age ( 35 years at delivery)Amniotic fluid volume and amniotic fluid index (AFI)Mildly decreased (AFI 8 cm)Oligohydramnios (AFI 5 cm)Cholestasis of PregnancyDiabetesGestational, diet controlledGestational, requiring medicationPregestationalFetal Growth RestrictionFetal weight 6th to 10th percentile, normal DopplerstudiesFetal weight 5th percentile or abnormal DopplerstudiesHypertensionChronic, not requiring medicationChronic, requiring medicationGestationalPreeclampsiaObesity, BMI 40Post-dates (past 40 weeks) pregnancyPrevious Intrauterine Fetal Demise (IUFD)Gestational Age toInitiate Testing36 weeksFrequency of Testing(NST and AFI)Once a weekTime of diagnosisTime of diagnosis32 weeksOnce a weekPer high-risk providerTwice a week (AFI once a week)40 weeks32 weeks32 weeksOnce a weekTwice a week (AFI once a week)Twice a week (AFI once a week)Time of diagnosisOnce a weekTime of diagnosisPer high-risk provider32 weeks32 weeksTime of diagnosisTime of diagnosis36 weeksOnce a weekTwice a week (AFI once a week)Twice a week (AFI once a week)Twice a week (AFI once a week)Once a week41 weeks42 weeksTwo weeks prior toearliest IUFDTwice a weekEvery other dayTwice a week (AFI once a week)Note: These guidelines may be based on data of variable quality, and in some cases represent expert opinion. This list isnot intended to be comprehensive, as numerous other indications for testing are accepted in complicated pregnancies.4UMHS Prenatal Care Guideline, September 2018
Table 3. Selected Indications for Consultation and/or Referral to High-Risk Pregnancy CareMedical ComplicationsCarcinomaGestational diabetes mellitus requiring medicationPregestational diabetes mellitus (with or without need for medication)Severe chronic medical diseaseThrombocytopenia, moderate or severePast OB/Gyn HistoryPrevious fetal or neonatal demise with continuing causePrevious major operations to the uterus and cervix, including classical (vertical incision) cesarean delivery,cerclage, resection of uterine septum, fibroid removal or myomectomy (but not including LTCS)Prior preterm birth 34 weeksRecurrent spontaneous abortion (3 or more)Current Pregnancy ComplicationsDocumented serious fetal anomaly (eg, diaphragmatic hernia)Hyperemesis unresponsive to outpatient therapyAlloimmunizationMultiple gestationSecond- or third-trimester fetal demisePreeclampsia with severe features or eclampsiaShortened cervix 20 mm identified on ultrasoundThird trimester bleeding due to placenta previa or placental abruptionVasa previaRationale for Recommendations Cultural sensitivityPreconception CareWhen to Deliver CarePreconception VisitEvidence is limited as to what represents an adequate numberof prenatal care visits. Studies have shown that some prenatalcare is better than no prenatal care, and that a visit during thefirst trimester is especially important. This guideline presentsa chronological sequence of prenatal care that is based onscientific evidence, recommendations of the US PublicHealth Service, clinical judgment regarding effectiveness ofidentifying and modifying risk, and the success of medicaland psychosocial interventions.A preconception visit is recommended for all womenplanning to become pregnant in order to minimize risk beforepregnancy. Elements of care are summarized in Table 1 anddetailed below. When a patient expresses a desire forpregnancy, consider the following: History: Perform and document maternal medical historyand risk assessment. Physical exam: Perform and document a completephysical examination. Laboratory tests: Assess infectious disease risk and immunizationstatus for rubella, tuberculosis, HIV, h
01.01.2008 · Current pregnancy symptoms ; Interim medical, psychosocial, and nutritional evaluation . Weight and blood pressure . Fetal heart rate . Aneuploidy screen † Diabetes screening at 12 weeks † Influenza vaccination † Review test results . Discuss: -Physical changes -Safe sex and sexuality during pregnancy -Exercise and fitness during pregnancy -Managing work during pregnancy -Seatbelt use