Transcription
Cath Lab Essentials:Basic Hemodynamics for theCath Lab and ICUAilin Barseghian El-Farra, MD, FACCAssistant Professor, Interventional CardiologyUniversity of California, IrvineDepartment of Cardiology
Right HeartCatheterization
By Don Ramey Logan - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid 38538349
INDICATIONS Cause of shock Pulmonary hypertension Fluid management and hemodynamicmonitoring Guidance for pericardial tamponade Constrictive versus restrictivecardiomyopathy Diagnosis of left to right shunt
CONTRAINDICATIONS ABSOLUTEcontraindications:– None CAUTION:– Pulmonaryhypertension– Elderly– Left bundlebranch block
EQUIPMENT
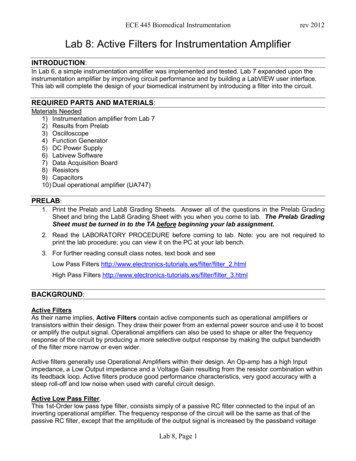
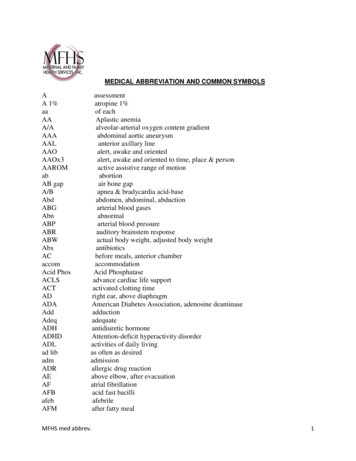
PULMONARY ARTERY CATHETEREXTRA PORTDISTAL PORTPROXIMAL PORTTHERMISTORBALLOON
TECHNIQUE
A Systematic Approach toHemodynamic Interpretation1. Establish the zero level and balance transducer.2. Confirm the scale of the recording.-40 mmHg for RHC, 200 mmHg for LHC3. Collect hemodynamics in a systematic method usingestablished protocols.4. Critically assess the pressure waveforms for properfidelity.5. Carefully time pressure events with the ECG.6. Review the tracings for common artifacts
Components of a Right HeartCatheterization1.Right atriumPulm HTN: mean– Mean (1-5 mmHg) PA pressure 25mmHg2.Right ventriclePCWP 15mmhg– Phasic (25/5 mmHg)3.Pulmonary capillary wedge– Mean (7-12 mmHg)4.Pulmonary artery– Phasic and mean (25/10 mmHg; mean 10-20mmHg)
Precautions Always record pressures at end-expiration During inspiration, pressures will be lowerdue to decrease in intrathoracic pressure Always zero and reference the system
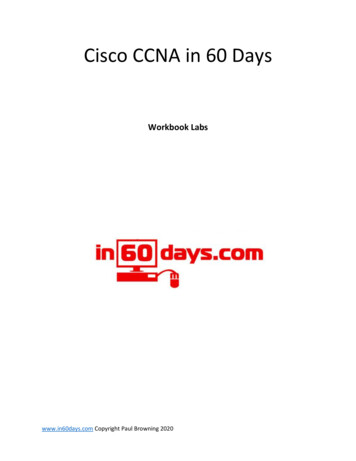
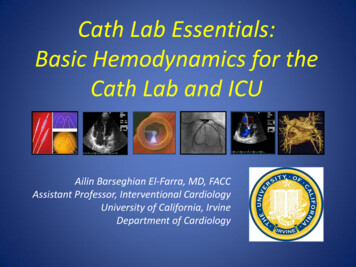
“SAT RUN”SVCSVC to RASTEP UPIf highestvalues areused, atleast 11%If average ofmultiplesamples,then 7%RA to PA STEP UPhighest or averagevalues 5%RIGHTATRIUMIVCLUNGSRA to RV STEP UPhighest values areused, at least 10%If average ofmultiple samples,then 5%(for L- R shunt)
1
SIMULTANEOUS RIGHT- and LEFT- HEART CATHETERIZATION1. Pulmonary artery (PA) catheter to pulmonary artery2. Measure cardiac output by measuring oxygen saturation in PAand AO blood samples to determine Fick output or bythermodilution (x3); screen for shunt.3. Record aortic pressures with AO catheter. Cross the AV into theventricle - Wedge the PA catheter - Measure simultaneous LVPCWP (mitral valve assessment).4. Pull back from PCWP to PA.5. Pull back from PA to right ventricle (RV) (to screen for pulmonicstenosis) and record RV.6. Record simultaneous LV-RV (constriction vs restriction).7. Pull back from RV to right atrium (RA) (to screen for tricuspidstenosis) and record RA8. Pull back from LV to AO (to screen for aortic stenosis).
CARDIAC CYCLE
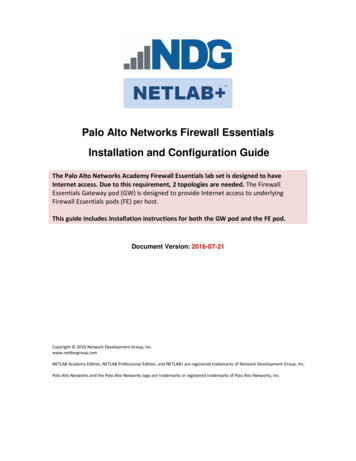
PHASES1: Atrial Contraction2: Isovolumic Contraction(TV/MV closure to PV/AV opening)3: Rapid Ejection4: Reduced Ejection(PV/AV opening to PV/AV closure)5: Isovolumic Relaxation(PV/AV closure to TV/MV opening)6: Rapid Ventricular Filling7: Reduced Ventricular Filling(TV/MV opening to TV/MV closure)
PRESSURE WAVE INTERPRETATION
LEFT HEART CATHETERIZATION
PITFALLS
ARTIFACTS
CARDIAC OUTPUT
Cardiac Output Thermodilution Fick Method
Thermodilution Bolus injection ofsaline into theproximal port Change intemperature ismeasured bythermistor in thedistal portion ofthe catheter
Fick Principle Described in 1870 Assumes rate of O2 consumption is a function of rate ofblood flow times the rate of O2 pick up by the RBCOxygen consumption1. Direct Fick:-Directly measured2. Indirect Fick:--3 ml O2/kgX 10
LimitationsThermodilutionFick Not accurate in tricuspidregurgitation Overestimated cardiacoutput at low outputstates Oxygen consumption isoften estimated by bodyweight (indirect method)rather than measureddirectly Large errors possible withsmall differences insaturations and hemoglobin. Measurements on room air
THANK YOU
Normal PressuresSiteNormal Value Mean(mmHg)Pressure(mmHg)0-5Right Atrium(or CVP)Right Ventricle 0Saturation75%75%10-2075%95-100%95-100%95-100%
Normal ValuesSiteValueSv020.60-0.75Stroke Volume60-100 ml/beatStroke Index33-47 ml/beat/m2Cardiac Output4-8 L/minCardiac Index2.5-4.0 L/min/m2SVR800-1200 dynes sec/-cm5PVR 250 dynes sec/-cm5MAP70-110 mmHg
References Bangalore and Bhatt. Right heart catheterization,coronary angiography and percutaneouscoronary intervention. Circulation, 2011; 124:e428-e433. Kern, Morton J. The Cardiac CatheterizationHandbook. Philadelphia, PA: Saunders Elsevier,2011. Print. Ragosta, Michael. Textbook of ClinicalHemodynamics. Philadelphia, PA:Saunders/Elsevier, 2008. Print.
2. Confirm the scale of the recording. -40 mmHg for RHC, 200 mmHg for LHC 3. Collect hemodynamics in a systematic method using established protocols. 4. Critically assess the pressure waveforms for proper fidelity. 5. Carefully time pressure events with the ECG. 6.