Transcription
THE MAGAZINE SERIES FOR ENHANCED EM LEARNINGVol. 2: Pediatric EmergenciesBY ANTON HELMAN & TARYN LLOYD
THE MAGAZINE SERIES FOR ENHANCED EM LEARNINGVol. 2: Pediatric EmergenciesBY ANTON HELMAN & TARYN LLOYD
Copyright 2016 by Medicine CasesEmergency Medicine Cases by Medicine Cases is copyrighted as “All RightsReserved.” This ebook is Creative Commons Attribution-NonCommercialNoDerivatives 3.0 Unsupported License. Upon written request, however, wemay be able to share our content with you for free in exchange for analyticdata. For permission requests, write to the publisher, addressed “Attention:Permissions Coordinator,” at the address below.Medicine Cases216 Balmoral AveToronto, ON, M4V 1J9www.emergencymedicinecases.comThis book has been authored with care to reflect generally accepted practices.As medicine is a rapidly changing field, new diagnostic and treatment modalitiesare likely to arise. It is the responsibility of the treating physician, relying onhis/her experience and the knowledge of the patient, to determine the bestmanagement plan for each patient. The authors and publisher of this bookare not responsible for errors or omissions, or for any consequences fromthe application of the information in this book, and disclaim any liability inconnection with the use of this information. This book makes no guarantee withrespect to the completeness or accuracy of the contents within.
OUR THANKS TO.EDITORS-IN-CHIEFAnton HelmanTaryn LloydPRODUCTION EDITORMichelle YeePRODUCTION MANAGERGarron HelmanCHAPTER WRITERSSean CaineLincoln FoersterAnna MacDonaldMichael MischMeeta PatelRobyn ShaferRob SimardAhmed TaherRajani VairavanathanPODCAST GUEST EXPERTSAlyssa AboSamina AliAlex ArroyoSarah CurtisAnthony CroccoJason FischerStephen FreedmanPODCAST SUMMARY EDITORSNiran ArgintaruLucas ChartierKeerat GrewalClaire HeslopMichael KilianREVIEW QUESTIONS AUTHORSDavid HomuthAreej ShahbazAnna JarvisEric LetovskySanjay MehtaAngelo MikrogianakisGina NetoJonathan PirieSarah ReidUniversity of Toronto, Faculty of MedicineEM Cases is a venture of the Schwartz/Reisman Emergency Medicine Institute.We’d like to thank our colleagues at SREMIfor their support and encouragement.Lawrence RicherJennifer RileyDennis ScolnikAdam SivitzRahim ValaniAmy Drendel
ACKNOWLEDGEMENTSI would like to thank my wife, Sasha, and my children Emma and Rowan fortheir ceaseless patience and support; my brother Garron for his dedication andadvice; my brother Wayne for the original website and logo design; my mentor,Walter Himmel, for his inspiration, friendship, and advice; the EM CasesAdvisory Board for their guidance; the EM Cases team (Lucas Chartier, TeresaChan, Justin Morgenstern, Michael Misch, Claire Heslop, Keerat Grewal, TarynLloyd, Michelle Yee, Lincoln Foerster, and Michael Kilian) for their hard work anddedication; Mike Cadogan for his inspiration to join the FOAMed community andhis unparalleled altruism; the Schwartz/Reisman Emergency Medicine Institute(Howard Ovens for his support and wisdom; Bjug Borgundvaag, Shirley Lee,and Shelley McLeod for their support and team spirit); Kuldeep Sidhu for hisleadership, support, and patience; all of the guest experts for their incredibleknowledge and wisdom; the FOAMed community for teaching me and for itsegalitarian spirit; and the EM Cases audience for your honest feedback and theinspiration to keep EM Cases growing. I feel immensely fortunate to have hadthe opportunities that have allowed to me to learn, and educate others, in aprofession that is continually blossoming.Anton Helman, MD, CCFP(EM), FCFPAssistant Professor, University of TorontoDepartment of Family & Community MedicineStaff Physician, North York General Hospital, Department of EmergencyMedicineEducation Innovation Lead, Schwartz-Reisman Emergency Medicine InstituteFounder, Editor-in-Chief, and host of Emergency Medicine CasesThanks to TREKK for its partnership in recruitingthe pediatric emergency guest experts for thepodcasts and for the needs assessment fromwhich the topics were chosen.
FOREWORDSocial media technologies are game-changers in health professions education.In the past several years, social media technologies have begun challenging howtraditional academic institutions think about education delivery and teaching.Expensive textbooks, classroom-based teaching, and siloed workshops arecompeting with the growing presence of open-access blogs, podcasts, andglobal online journal clubs for learner attention. New communities of practiceare appearing constantly, connected by the Internet.EM Cases was one of the first podcasts I noticed at the forefront of thismovement. When it launched in 2010, I was immediately impressed by the highquality content and attention to detail. I am not surprised to see that it currentlygarners an amazing 90,000 downloads per month. Its popularity is a reflectionof the how today’s busy lifelong learners consume medical knowledge. Ina word, it is—opportunistically. With so many digital distractors and anoverwhelming amount of medical information to keep abreast of in today’sworld, education delivery needs to be portable, easily accessible, and digestiblein chunks. Thus podcasts provide an appealing solution for the busy learner,who may wish to listen while driving to work or exercising.As a blogger, however, I am keenly aware that blogs and podcasts generallyprovide a rather haphazard delivery of content to learners. I am guilty of that. Ipublish what is most timely and relevant in the eyes of my editorial team. Thereis no set curriculum framing the periodic release of new materials, and generallyeach blog post is a standalone lesson. But can’t we, as educators, do better?EM Cases can. The launch of the EM Cases Digest series is a huge step towardstructuring the modern learning experience using social media technology. Thismarks the evolution of EM Cases from a podcast resource to a premiere podcastenhanced educational curriculum. While many podcast organizations have briefshow notes for their podcasts, none that I know of has created a professionallydesigned ebook, integrating podcasts into a thoughtfully organized frameworkof text- and image-based lessons with question-and-answer sections.
FOREWORD (Continued)From a pedagogical and instructional design standpoint, this innovativeapproach makes sense. It optimizes and solidifies learning based on Mayer’scognitive theory of multimedia learning. Incorporating both visual (ebook) andauditory (podcast) elements optimizes working memory and thus learning.Congratulations to Dr. Anton Helman and his EM Cases Digest team, who are atthe forefront of reimagining health professions education. I can only imaginethe ginormous effort that went into producing such a product with an eyetoward visual design, education theory, and multimedia integration. The resultis an ebook series that is fun, educational, and a joy to read. Thank you foryour dedication and pioneering vision for advancing education in emergencymedicine.Your friend and fan,MichelleMichelle Lin, MDAcademy Endowed Chair of Emergency MedicineProfessor of Emergency MedicineUniversity of California, San Francisco;Editor-in-ChiefAcademic Life in Emergency Medicine blog (http://aliem.com)@M Lin
Guide to EM Cases DigestWe hope you will find the EM Cases Digest series to be an interactive, flexible, and engaging way to enhance your emergency medicine learning journey. These ebooks areintended to be an adjunct to the EmergencyMedicineCases.com podcasts, as well as toexisting emergency medicine curricula and resources. For optimal learning, we suggestEM Cases Digest be used in conjunction with the podcasts for spaced, repetitive learning,and as an interactive workbook, through which you can explore the links, videos, andoriginal resources (links to original references can all be found on our website). We encourage you to attempt the Q&As actively, revealing expert answers only after formulating your own answers and opinions.Here’s a little descriptionto help explain all of thegraphics in this book:ClinicalPearlsAh-HasPitfallsClinical Pearls:Nuggets of wisdomPitfalls:Common regretsAh-Has:Wow momentsTools & Rules:Clinical decision toolsand rulesTools& RulesExpertOpinionCautionCaution:Warning; badness aheadExpert Opinion:What our guest expertsthink when the evidence isunclearKey References:EBM game-changersWhat would you do?:Reflect on what you woulddo in your practiceKeyReferencesYourCommentsWhat wouldyou do?1Your Comments:Go to the linked blog postto leave your comment
JUMP TO CHAPTER.Chapter 1: Fever Without a SourcePage 4Link to the podcast with Sarah Reid and Gina NetoChapter 2: Sepsis and Septic ShockPage 22Link to the podcast with Sarah Reid and Gina NetoChapter 3: Pain ManagementPage 35Link to the podcast with Samina Ali and Anthony CroccoChapter 4: Head InjuryPage 53Link to the podcast with Rahim Valani and Jennifer RileyChapter 5: Pediatric Procedural SedationPage 68Listen to the podcast with Amy DrendelChapter 6: Orthopedic InjuriesPage 82Link to the podcast with Sanjay Mehta and Jonathan PirieChapter 7: POCUS Nerve BlocksPage 106Link to the podcast with Jason FischerChapter 8: Abdominal Pain and AppendicitisPage 117Link to the podcast with Anna Jarvis and Stephen FreedmanChapter 9: POCUS Appendicitis and IntussusceptionPage 132Link to the podcast with Adam Sivitz and Alex ArroyoChapter 10: Gastroenteritis, Constipation and ObstructionLink to the podcast with Anna Jarvis and Stephen FreedmanPage 143
JUMP TO CHAPTER.Chapter 11: Diabetic KetoacidosisPage 168Link to the podcast with Sarah Reid and Sarah CurtisChapter 12: BronchiolitisPage 183Link to the podcast with Dennis Scolnik and Sanjay MehtaListen to the bonus podcast with Amy PlintChapter 13: AsthmaPage 197Link to the podcast with Dennis Scolnik and Sanjay MehtaChapter 14: Lung POCUSPage 212Link to the podcast with Alyssa AboChapter 15: CroupPage 221Chapter 16: Pediatric SyncopePage 230Link to the podcast with Eric Letovsky and Anna JarvisChapter 17: Pediatric SeizuresPage 250Link to the podcast with Lawrence Richer and Angelo MikrogianakisRapid Review QuestionsPage 269
EM CASES DIGEST - VOL. 2: PEDIATRIC EMERGENCIESCHAPTER 1:FEVER WITHOUT ASOURCELISTEN TO THE PODCAST WITH SARAH REID AND GINA NETO HEREObjectives1. Understand the principles of fever management2. Identify abnormal vital signs in the setting of pediatric fever3. Have an approach to the investigation of UTI in children4. Develop an approach to the child with fever without a source5. Know when to order a full septic workup versus a partial septic workup4
EM Cases Digest - Vol. 2: Pediatric EmergenciesApproximately 20% of children who present to the ED with fever will havefever without a source despite your thorough history and physical exam.A small but significant number of this 20% without an identifiable source offever will have an occult bacterial infection—UTI, bacteremia, pneumonia,or even the dreaded early bacterial meningitis. These are all defined asserious bacterial infections (SBI), with occult UTI being the most common SBI(especially in children under the age of two years).In the old days, we used to do a full septic workup including LP for all infantsunder the age of three months; thankfully, times have changed in thepost-Haemophilus and pneumoccocal vaccine age, and we aren’t quite soaggressive any more with our workups. Nonetheless, it’s still controversialas to which kids need a full septic workup, which kids need a partial septicworkup, which kids need just a urine dip, and which kids need little except toreassure the parents.5
EM Cases Digest - Vol. 2: Pediatric EmergenciesCASE 1:FEVER PRINCIPLESA 12-month-old girl is brought in to your ED with three days of fever between38.5 C and 40 C. She is previously healthy, immunizations are up to date(including Haemophilus and pneumococcal vaccines), and there has beenno recent travel. She has no cough, no difficulty breathing, no vomiting, noapparent belly pain, no rash, and no diarrhea. She’s been eating and drinkingwell at home.Q: Does this child require a rectal temperature measurement?Which children with suspected fever require a rectal temperaturemeasurement in the ED?A: As rectal temperatures are the most accurate estimation of core bodytemperature compared with axillary, oral, and ear temperatures, and missingfever in younger children may carry high morbidity, it is recommended that arectal temperature be obtained in all neonates, infants, and toddlers (youngerthan three years old) who present to the ED with suspected fever or with anundefined illness that could be the result of an infection/sepsis.Q: The parents are very concerned that the “very high fever” of their12-month-old girl might cause brain damage or represent a seriousillness. This is a common concern. How do you counsel the parents?A: Fever itself is the body’s natural response to fighting infection, and does notinherently cause harm. Children with infection as a cause of their fever almostnever mount a fever high enough to be dangerous ( 41.5 C); these very hightemperatures are typically seen only in non-infectious causes of hyperthermia.In terms of predicting bacteremia, the precise height of thefever is not as important as the duration of the fever. A feverof 39.8 C that has lasted for two days is not as concerning as afever of 38.2 C that has lasted for six days in terms of the risk ofbacteremia.6Video:Click here to seeDr. Anthony Crocco’srant on feverphobia.
EM Cases Digest - Vol. 2: Pediatric EmergenciesClinical Pearl:A parent’s assessment offever by touch has beenshown to correlate fairlywell with a true fever. Achild who is brought infor a “tactile fever” butwho is afebrile in the EDstill warrants a thoroughassessment for sourcesof fever. Be sure to askif the child received anantipyretic prior to yourassessment.Q: This child has a rectal temperature of 39 C.Do we need to treat this child’s fever in theED?A: While this temperature is not inherentlydangerous to the child, there are benefits to treatingfever. Lowering the temperature of a febrile child notonly provides comfort and minimizes dehydration,but treating the fever also allows for more accurateprognostication when the now afebrile child is reexamined. When a child changes from being irritableor lethargic to active, playful, and alert after receivingan antipyretic for their fever, you can usually beless concerned about an SBI. If the child’s vital signsand clinical picture continue to be concerning whenafebrile, then an SBI should be suspected.Q: Which is the better antipyretic:acetaminophen or ibuprofen?Expert Opinion:To avoid potentialtoxicities, our expertsrecommend no morethan three doses ofibuprofen 10 mg/kgper day and no morethan four doses ofacetaminophen 15 mg/kgper day.A: Studies show that ibuprofen is superior at treatingboth fever and pain in children.Caution! Combining ibuprofen andacetaminophen may be a more effectivestrategy than either alone (based on adult literature),however, there is a real risk of toxicity due to dosingerrors in children. If advising this strategy, a handouton dosing methods can help parents keep track of adosing schedule.FOAMed link: Click here for a great blog postreviewing the literature on the treatment of pediatricfever by The Skeptics’ Guide to EM.7
EM Cases Digest - Vol. 2: Pediatric EmergenciesCase continued: On exam of this 12-month-old female, she appears tiredbut non-toxic. Her vital signs are: a rectal temperature of 39.0 C, heartrate of 125, and respiratory rate of 25. A thorough head-to-toe examreveals an erythematous and bulging left tympanic membrane.Q: What is the normal change in heart rate and respiratory rate inresponse to a fever?A:Respiratory rate:Increases by fiveHeart rate:Increases by 10breaths per minutebeats per minuteFor every degree of fever above 38 CSo, in our 12-month-old girl: Corrected HR 125 – (10 x 1) 115 Corrected RR 25 – (5 x 1) 20Normal Pediatric Vital Signs by AgeVital SignHeart RateResp Rate(breaths permin)Infant (0-12 mths)Child (1 -11 years)Pre-teen/Teen (12 yrs )100 to 160 bpm70 to 120 bpm60 to 100 bpm0 to 6 months30 to 60 bpm1 to 5 years20 to 30 bpm12 to 18 bpm6 to 12 months24 to 30 bpm6 to 11 years12 to 20 bpm0 to 6 months65 to 90 systolic/45 to 65 mm Hg90 to 110 systolic /55 to 75 diastolicmmHgBlood Pressure6 to 12 months80 to 100 systolic/55 to 65 mm Hg8110 to 135 systolic/65 to 85 diastolicmmHg
EM Cases Digest - Vol. 2: Pediatric EmergenciesRectal TemperatureAll ages36.6 C to 38 C (97.9 F to 100.4 F)Tympanic Temperature35.8 C to 38 C (96.4 F to 100.4 F)Oral Temperature35.5 C to 37.5 C (95.9 F to 99.5 F)Axillary Temperature34.7 C to 37.3 C (94.5 F to 99.1 F)Case resolution: The child is observed in the ED and is treated withibuprofen 10 mg/kg po. She continues to look well, normal vital signs arerecorded, and she is tolerating oral fluids. You diagnose her with otitismedia and give the parents a prescription for amoxicillin. You give themclear discharge instructions and advise them to follow up with theirprimary-care physician.Clinical Pearl:If the child has abnormal vital signs after correcting for fever, have a highdegree of suspicion for dehydration, early compensated shock, or earlysepsis. Make sure you assess for perfusion and mentation, and ask abouturine output.9
EM Cases Digest - Vol. 2: Pediatric EmergenciesCASE 2:URINARY TRACT INFECTIONAn 18-month-old male is brought to your ED with four days of fever athome between 38.0 C and 38.8 C. His parents say he has been fussierthan usual. He has no significant past medical history, his immunizationsare up to date, and there is no history of recent travel. He has beendrinking well at home. No infectious source is identified on history. Onexam, he is alert and non-toxic. Vital signs are normal except for anoral temp of 38.2 C. On a thorough head-to-toe exam you do not find asource of infection.Q: This child has no source of infection that is readilyidentifiable on history or physical. What is the differencebetween fever without a source and fever of unknown origin?A: Fever without a source: There is no identifiable source of fever after acomplete history and physical.Fever of unknown origin: At least two to three weeks of fever without anidentifiable source after initial investigations. The most likely cause remainsinfectious but other causes, such as malignancy and rheumatologic causes,need to be considered.Q: For children who present to the ED with fever without asource, how likely are they to be suffering from an occult seriousbacterial infection?A: A small proportion of these infants and young children will havean occult bacterial infection, such as an occult urinary tract infection,pneumonia, bacteremia or even early bacterial meningitis. These aredefined as SBIs, and occult UTI is the most common SBI, especially in thefirst two years of life.10
EM Cases Digest - Vol. 2: Pediatric EmergenciesQ: Does immunizing children help prevent SBIs?A: There is a very low rate of bacteremia in children with two or more dosesof the Haemophilus influenzae type b and pneumococcal conjugate vaccine.In Canada, the Haemophilus vaccine is given at two, four, six, and 18 months,and the pneumococcal vaccine is given at two, four, and12 months.Ah-Ha!For the child with a fever without a source, be sure to take a complete historyand to undress the child completely when performing a thorough physical exam.Pay particular attention to the following points on history and physical exam:History: Duration of fever Recent surgeries Underlying medicalco-morbidities Previous infections Immunization statusPhysical exam: A careful assessment of the vital signs Behaviour and mental status Meningeal signs and fontanelles If the child is at an ambulatory stageof development, watch the child walkand look for a limp A careful abdominal exam A careful skin exam A careful joint examQ: What are the five most common sources of fever in a childwithout an obvious source for their fever after initial assessment?A: These are defined by the LUCAS mnemonic: Lungs Urine CNS Abdomen Skin11
EM Cases Digest - Vol. 2: Pediatric EmergenciesPediatric Assessment of AppearanceElementExplanationToneIs he/she moving around or resisting examinationvigorously and spontaneously? Is there good muscle tone?InteractabilityHow alert is he/she? How readily does a person, object, orsound distract or draw attention? Will he/she reach out,grasp, and play with a toy or new object, such as a penlightor tongue depressor?ConsolabilityCan he/she be consoled or comforted by the caregiver orby the clinician?Look/gazeCan he/she fix her gaze on the clinician’s or caregiver’sface, or is there a “nobody home,” glassy-eyed stare?Speech/cryIs his/her speech/cry strong, and spontaneous, or weak,muffled, or hoarse?Q: Is this 18-month-old male with a fourday history of fever at risk for a UTI?What are the risk factors for UTI in thepediatric population?A: Yes, he is at risk. The following are risk factorsfor UTI: Females 24 months All males six months Uncircumcised males 24 months Fever for more than two days Fever 39 C History of previous UTI12
EM Cases Digest - Vol. 2: Pediatric EmergenciesQ: Does this 18-month-old male with a four-day history of fever needtesting for a UTI? How do you decide which children with fever totest for a UTI?A: Yes, this child does require testing for a UTI as he has multiple risk factors. Three months:Get a urine samplefor all babies withfever without asourceThree to 24months:Check all girls; checkuncircumcised boys if one risk factor andcircumcised boys if two risk factors 24 months:Check all girls; checkall symptomaticuncircumcised boys andcircumcised boys withseveral symptoms of UTIQ: You tell the parents you would like to get a urine sample, andthey immediately express concern that they don’t want their childto have a catheter placed. How do you get a urine sample in thissituation?A: Your investigation of this child could begin with a urine bag specimen. Ingeneral, the following principles apply when getting a urine sample. Two months:Obtain urine sampleby catheterization andsend every samplefor a culture (as theurinalysis may benormal with a trueinfection)From two monthsuntil toilet trained:Bag urine is acceptableto screen by microscopy;if positive (i.e., 10–20WBCs/hpf), a cathetersample is necessary.13Toilet trained:Obtain a midstream urinesample afteradequatecleaning of thegenitals
EM Cases Digest - Vol. 2: Pediatric EmergenciesClinical Pearl:One study describes a safe, quick, and effective technique to obtaining amidstream urine sample. Twenty-five minutes after feeding, simply hold thebaby upright, gently tap on the bladder for 30 seconds, then massage thesacrum for 30 seconds. Both stimulation manoeuvres are repeated untilmicturition starts.Q: In what way can the urine dipstick be deceptive in childrenwho aren’t toilet trained?A: The urine dipstick relies on leukocyte esterase and nitrites as an indirectmeasure of pyruria and bacteriuria. The urine needs to be “incubating” inthe bladder for about four hours to become positive on the dipstick. So, thechild who isn’t toilet trained is urinating too often (more frequently thanevery four hours) for the dipstick to become positive when an infection ispresent.Case continued: Let’s go back to our case of the 18-month-olduncircumcised male. We end up getting a urine bag specimen. There are40–50 WBCs/hpf, so we proceed to get a urine sample by catheterizationand send it for a urinalysis. The results come back with 30–40 WBCs/hpf, suggestive of a UTI. As you are looking up the appropriate antibioticdose, you wonder about the child’s disposition.Q: Which children with UTI need to be admitted to hospital?A:In general, children two months of age with a UTI should be admittedto hospital. Well-appearing children two months old can usually bedischarged home on antibiotics with good follow-up, provided they do notshow any evidence of dehydration and have reliable caregivers.14
EM Cases Digest - Vol. 2: Pediatric EmergenciesQ: The parents ask whether their child has a problem with hiskidneys or bladder that predisposed him to a UTI. What sort offollow-up should this 18-month-old male with a first-time UTIhave?A: All children two years of age with a first-time UTI should have anoutpatient ultrasound to look for vesico-ureteral reflux and structuralanomalies. A voiding cysto-urethrogram (VCUG) is no longer recommendedfor children with a first-time UTI.Q: What antibiotic options do you have for treating this childwith a UTI?A: Treatment of pediatric UTI: Antibiotic options depend on localantibiotic resistance patterns, however, in our experts’ catchment area(Ottawa) In hospital: IV ampicillin and gentamicin Outpatient: Cephalexin for most, or cefixime for infants two to sixmonths old, or for those you are worried have a complicated UTI orurinary tract abnormalitiesClinical Tools:Click here for the CanadianPaediatric SocietyGuidelines on UTI inchildren15
EM Cases Digest - Vol. 2: Pediatric EmergenciesCASE 3:PNEUMONIA STRIKESYou are seeing a four-year-old female with a six-day history of a runnynose, cough, and fatigue. She was brought to your ED because shehas had a fever for the past three days. She is otherwise healthy. Onexamination, she appears tired but non-toxic. She has a temperature of40.0 C, a respiratory rate of 30, a heart rate of 130, and a blood pressureof 110/70. She has mild increased work of breathing.Q: You are considering a diagnosis of pneumonia. What are thefactors on history, physical examination, and blood work thatmake this diagnosis more likely?A: History: Upper respiratory infectionfor several days followedby onset of fever Fever for five days Cough for 10 days Temperature 40 CPhysical Exam: Increased work of breathing TachypneaInvestigations: WBC count 20,000Clinical Pearl:Carefully examine the patient for “quiet tachypnea.” Children with quiettachypnea will remain tachypneic after correcting the respiratory rate for thefever (as described above)—this may indicate an underlying pneumonia.16
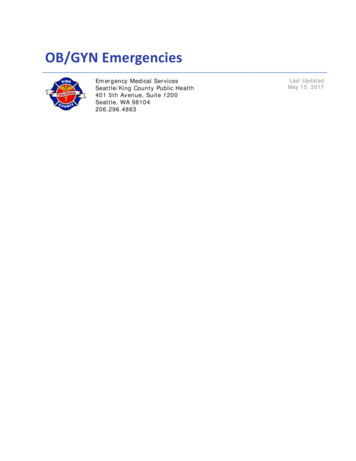
EM Cases Digest - Vol. 2: Pediatric EmergenciesQ: Other than the mild increased work of breathing, the rest of yourphysical exam is normal. Does this four-year old girl warrant a chestX-ray?A: Yes, she should have a chest X-ray (see below) because she has multiple factorsthat make the diagnosis of pneumonia more likely. Despite the fact that mostpediatric pneumonias are viral in origin, we are unable to accurately differentiatebetween viral and bacterial causes based on the X-ray appearance alone. It istherefore prudent to start antibiotics in all children who have an infiltrate on chestX-ray that is consistent with pneumonia.Q: Does this child require blood work and/or blood cultures? What are theindications for blood work and blood cultures in pediatric fever without asource?A: A well-appearing, immunized child with a fever typically does not need blood workor cultures. While C-reactive protein (CRP) and pro-calcitonin may be helpful in riskstratifying patients with fever without a source, this hasn’t become a standard ofpractice, and the availability of pro-calcitonin in limited.17
EM Cases Digest - Vol. 2: Pediatric EmergenciesCASE 4:THE FEBRILE NEONATEA two-week-old female born at term is brought into your ED with a 24hour history of fever. No source can be identified on history or physicalexam. The child is alert but has a rectal temperature of 39.1 C.Q: What sort of workup does this infant need?A: This patient needs a full septic workup. Infants in the first month of lifehave the highest rate of SBI out of any time in childhood, and thereforethey represent a high-risk group.A full septic workup includes: CBC Blood cultures Urinalysis collected by catheter Urine culture CSF sampling (send for: cell count, culture, Gram stain, protein, glucose,and viral studies)Q: This infant is started on IV antibiotics. Your resident asks youwhether the child requires acyclovir, in case the child has herpessimplex encephalitis (HSV). What do you tell your resident?A: If you suspect meningitis based on physical exam or lumbar punctureresults, start acyclovir. This is especially important in children 14 days ofage, as the rate of HSV meningitis is highest in this age group. HSV can alsocause hepatitis and pneumonitis, so check for these if you are suspicious ofHSV meningitis.18
EM Cases Digest - Vol. 2: Pediatric EmergenciesCASE 5:THE PARTIAL SEPTIC WORKUPA two-month-old male born at 36 weeks is brought in with a 12-hourhistory of fever. He is unvaccinated and he is circumcised. No focus isidentified on history or physical exam. He appears non-toxic and has arectal temperature of 38.6 C, and the rest of the vitals are normal.Q: How do you correct for age when it comes to prematureinfants who present with fever to the ED?A: When calculating age for the purposes of infection, you should use thechronological age; however, premature babies with a complex medicalhistory should be thought of as high risk.Q: What sort of work-up does this two-month-old boy require?A: This child will require at least a partial septic workup and thenbe assessed regarding low-risk criteria to determine if any furtherinvestigations are needed.For children between 29–90 days of age, there are many criteria for thework-up of fever without a source. Our experts recommend using the lowrisk criteria from the American Academy of Pediatrics. If these criteria aremet, the child has an approximate risk of 1.5% of developing an SBI. Thesechildren may be safely discharged home if they have reliable parents andfollow-up is available within 24 hours.Low-risk criteria (American Academy of Pediatrics): No obvious source of infection No complex past medical history WBC count between 5–15,00
2. Identify abnormal vital signs in the setting of pediatric fever 3. Have an approach to the investigation of UTI in children 4. Develop an approach to the child with fever without a source 5. Know when to order a full septic workup versus a partial septic workup 4 EM CASES DIGEST - VOL. 2: PEDIATR