Transcription
Review in depth 613Echocardiographic evaluation of coronary artery diseaseYiannis S. Chatzizisisa,*, Venkatesh L. Murthyb,* and Scott D. SolomonaAlthough the availability and utilization of othernoninvasive imaging modalities for the evaluation ofcoronary artery disease have expanded over the lastdecade, echocardiography remains the most accessible,cost-effective, and lowest risk imaging choice for manyindications. The clinical utility of mature echocardiographicmethods (i.e. two-dimensional echocardiography, stressechocardiography, contrast echocardiography) acrossthe spectrum of coronary artery disease has been wellestablished by numerous clinical studies. With continuingadvancements in ultrasound technology, emergingultrasound technologies such as three-dimensionalechocardiography, tissue Doppler imaging, and speckletracking methods hold significant promise to further widenthe scope of clinical applications and improve diagnosticaccuracy. In this review, we provide an update on the roleof echocardiography in the diagnosis, management,and prognosis of coronary artery disease and introduceemerging technologies that are anticipated to furtherincrease the clinical utility of echocardiography in theevaluation of patients with coronary artery disease. Coronc 2013 Wolters Kluwer Health Artery Dis 24:613–623 Lippincott Williams & Wilkins.IntroductionChronic myocardial ischemiaDespite numerous advances over the past severaldecades, the diagnosis and management of coronaryartery disease remains challenging. Noninvasive imagingmethods have been utilized to surmount the limitationsof nonimaging techniques, such as the poor sensitivityand specificity of exercise testing and the difficulty inevaluation of ischemia in patients with impaired mobilityor left bundle branch block [1–3]. In these patients,imaging is generally required to evaluate for the presence,extent, and severity of coronary artery disease. Because ofits broad availability, lack of radiation, and relatively lowcost, echocardiography is an increasingly widely usedexamination. The clinical utility of echocardiographyacross the spectrum of coronary artery disease has beenwell established by a large number of studies (Table 1).With continuing advancements in ultrasound technology,emerging ultrasound methods such as three-dimensionalechocardiography, ultrasound contrast agents, tissueDoppler imaging, and speckle tracking methods holdsignificant promise to further widen the scope of clinicalapplications and improve diagnostic accuracy.Myocardial ischemia is the result of a regional transient imbalance between myocardial oxygen supplyand demand, most often because of inadequate myocardial perfusion as a result of atherosclerotic coronaryartery disease. Hypoperfusion initiates an ischemiccascade of intracellular changes that results in a shift incellular metabolism from glucose to fatty acids [2,4].Decreased ATP production because of decreased oxygensupply required for aerobic metabolism results in failureThe purpose of this review is (i) to provide an update onthe role of echocardiography in the diagnosis, management,and prognosis of coronary artery disease and (ii) tointroduce emerging technologies that are anticipatedto further increase the clinical utility of echocardiography in the evaluation of patients with coronary arterydisease.c 2013 Wolters Kluwer Health Lippincott Williams & Wilkins0954-6928 Coronary Artery Disease 2013, 24:613–623Keywords: contrast echocardiography, coronary artery disease, emergingechocardiography methods, stress echocardiographyaNon-Invasive Cardiovascular Imaging Program, Cardiovascular Division, Brighamand Women’s Hospital, Harvard Medical School, Boston, Massachusetts andbDivisions of Cardiovascular Medicine, Nuclear Medicine and CardiothoracicRadiology, University of Michigan, Ann Arbor, Michigan, USACorrespondence to Scott D. Solomon, MD, Non-Invasive Cardiovascular ImagingProgram, Cardiovascular Division, Brigham and Women’s Hospital, HarvardMedical School, 75 Francis Street, Boston, MA 02115, USATel: 1 857 307 1960; fax: 1 857 307 1944;e-mail: ssolomon@rics.bwh.harvard.edu*Yiannis S. Chatzizisis and Venkatesh L. Murthy contributed equally to the writingof this article.Table 1 Role of echocardiography in the spectrum of coronaryartery diseaseCoronary artery diseasemanifestationChronic myocardial ischemiaAcute coronary syndromeComplications of myocardialinfarctionRisk stratificationMyocardial viabilityIschemic cardiomyopathyEchocardiography methodStress echocardiographyContrast-enhanced stress echocardiographyMyocardial contrast echocardiographyThree-dimensional echocardiographyDoppler tissue imagingSpeckle tracking imagingTwo-dimensional resting echocardiographyStress echocardiographyMyocardial contrast echocardiographySpeckle tracking imagingTwo-dimensional resting echocardiographyContrast-enhanced two-dimensionalechocardiographyTwo-dimensional resting echocardiographyStress echocardiographyDobutamine stress echocardiographyMyocardial contrast echocardiographyStrain imagingTwo-dimensional resting echocardiographyDOI: 10.1097/MCA.0000000000000028Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
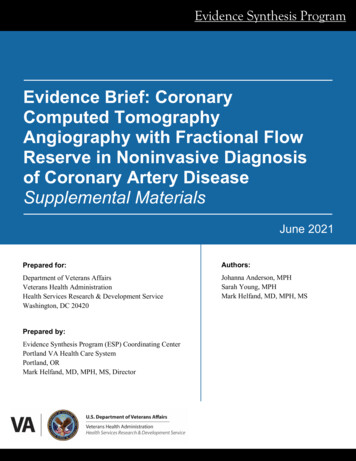
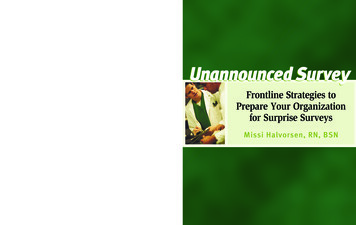
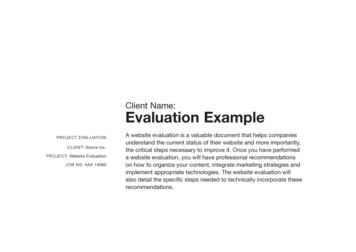
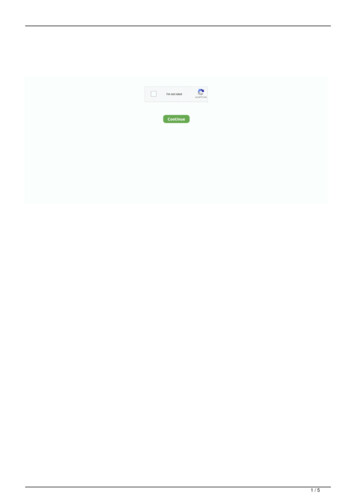
614 Coronary Artery Disease 2013, Vol 24 No 7Fig. 1BiomarkersChest painEKGSystolic dysfunctionEcho/MRIIschemiaEKG changesDiastolic dysfunctionPETMetabolic disordersPerfusion defectNuclear/EchoMRI/CTATimeIschemic cascade and the role of standard imaging modalities in the assessment of each element of the cascade. CTA, computed tomographyangiography; EKG, electrocardiography; PET, positron emission tomography.of calcium reuptake into the sarcoplasmic reticulum. As aresult, diastolic dysfunction is the initial manifestation,later followed by systolic dysfunction and repolarizationabnormalities seen as ST-segment changes on the surfaceECG. Chest pain is a late manifestation of this cascade.The severity of left ventricular dysfunction, ECG changes,and clinical presentation are dependent on the extent andseverity of hypoperfusion. Figure 1 presents the ischemiccascade and the role of standard noninvasive imagingmodalities in assessing each element of this cascade.Standard echocardiography methods can provide important information when the hypoperfusion results inischemia and systolic dysfunction before the onset ofECG changes, or clinical symptoms. The appropriate usecriteria of echocardiography in chronic myocardial ischemia are summarized in Table 2 and Fig. 2 [5].Stress echocardiographyIn severe cases of chronic myocardial hypoperfusion,myocardial ischemia may result in decreased regional orglobal systolic function [6]. More commonly, wall motionand wall thickening abnormalities are observed only whenischemia is induced by exercise or pharmacologic stress.Stress echocardiography techniquesStress echocardiography can be performed with exercise orpharmacologic agents, most commonly dobutamine [3,7].Common exercise protocols include treadmill and uprightor supine bicycle exercise. With treadmill exercise, stressechocardiography images are obtained at baseline beforethe initiation of exercise and after exercise within the firstminute after the conclusion of exercise. Rapid acquisitionof high-quality images requires careful planning and hightechnical skill levels on the part of the sonographer.Ultrasound contrast may be administered to improvevisualization of wall motion abnormalities. Hemodynamicmonitoring (heart rate and blood pressure) is also performed. Figure 3a presents the protocol used for treadmillstress echocardiography. Upright or supine bicycle exercise enables imaging at peak exercise, thereby increasingthe sensitivity of the method by reducing the possibilityof resolution of ischemia between the end of exercise andthe start of imaging.For patients who are not able to exercise or for theassessment of myocardial viability, pharmacological stressechocardiography with sympathomimetics (i.e. dobutamine) or vasodilators (i.e. dypiradamole, adenosine) ispreferred. Most commonly, increasing rates of dobutamine infusion to a peak dose of 40 mcg/kg/min may besupplemented by atropine in divided doses up to 2 mg toachieve the target heart rate (i.e. 85% of the agepredicted maximum heart rate). Dobutamine stimulatesadrenoreceptors in the myocardium, inducing positiveinotropic and chronotropic effects, thereby increasingmyocardial oxygen demand and resulting in ischemia andmyocardial systolic dysfunction in regions subtended bycoronary branches downstream of flow-limiting lesions.Figure 3b presents the commonly used protocol fordobutamine stress echocardiography.Vasodilator agents are less commonly used for pharmacologic stress echo. These agents stimulate adenosinereceptors, which causes coronary vasodilation. In thepresence of severe or extensive coronary disease, thismay result in coronary steal and subsequent systolicdysfunction. In some cases, the secondary effect ofCopyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Echocardiography and coronary artery disease Chatzizisis et al. 615Table 2Echocardiography appropriate use criteria in coronary artery disease [5]Chronic myocardial ischemiaStress echocardiographyAcute coronary syndromeMyocardial contrastechocardiographyTwo-dimensional echocardiographyStress echocardiographyComplications of myocardialinfarctionRisk stratificationMyocardial viabilityIschemic cardiomyopathyMyocardial contrastechocardiographyTwo-dimensional echocardiographyLow pretest probability of CADECG uninterpretable or unable to exerciseIntermediate pretest probability of CADECG interpretable and able to exerciseIntermediate pretest probability of CADECG uninterpretable or unable to exerciseHigh pretest probability of CADIrrespective of ECG interpretability and ability to exerciseNo current guidelinesAcute chest pain with suspected myocardial infarction and nondiagnostic ECG whena resting echocardiogram can be performed during painEvaluation of a patient without chest pain but with other features of an ischemic equivalentor laboratory markers indicative of ongoing myocardial infarctionPossible acute coronary syndromeECG: no ischemic changes or with LBBB or electronically paced ventricular rhythmLow-risk TIMI scorePeak troponin: borderline, equivocal, minimally elevatedPossible acute coronary syndromeECG: no ischemic changes or with LBBB or electronically paced ventricular rhythmHigh-risk TIMI scoreNegative troponin levelsPossible acute coronary syndromeECG: no ischemic changes or with LBBB or electronically paced ventricular rhythmHigh-risk TIMI scorePeak troponin: borderline, equivocal, minimally elevatedPossible acute coronary syndromeECG: no ischemic changes or with LBBB or electronically paced ventricular rhythmLow-risk TIMI scoreNegative troponin levelsNo current guidelinesSuspected complication of myocardial ischemia/infarction, including but not limited toacute mitral regurgitation, ventricular septal defect, free-wall rupture/tamponade, shock,right ventricular involvement, heart failure or thrombusTwo-dimensional echocardiographyInitial evaluation of ventricular function following acute coronary syndromeRe-evaluation of ventricular function following acute coronary syndrome during recoveryphase when results will guide therapyStress echocardiographySTEMI/non-ST acute coronary syndromeHemodynamically stable, no recurrent chest pain symptoms, or no signs of heart failureTo evaluate for inducible ischemiaNo previous coronary angiography since the index eventPost-PCI or bypassIncomplete revascularizationAdditional revascularization feasibleDobutamine stress echocardiography Known moderate or severe LV dysfunctionPatient eligible for revascularizationUse of dobutamine stress onlyMyocardial contrastNo current guidelinesechocardiographyTwo-dimensional echocardiographyInitial evaluation of known or suspected ischemic cardiomyopathyRe-evaluation of known ischemic cardiomyopathy with a change in clinical statusor cardiac examination or to guide therapyCAD, coronary artery disease; LBBB, left bundle branch block; LV, left ventricular; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardialinfarction; TIMI, thrombolysis in myocardial infarction.increased heart rate in response to systemic vasodilationmay also cause ischemia. When coupled with perfusionimaging methods, vasodilator agents can provide excellent sensitivity for the diagnosis of coronary arterydisease. As such, they are best suited for use withmyocardial contrast perfusion echocardiography, nuclearperfusion imaging methods, or cardiac MRI.Interpretation of stress echocardiogramsGenerally, multiple views of each segment of themyocardium are obtained at rest and stress to maximizediagnostic certainty. Standard protocols include short axisimaging at three levels: basal, mid-ventricular (usually atthe level of papillary muscles), and apex. Long-axis viewsfrom either the apical and/or the parasternal windows,as well as apical two-chamber and four-chamber viewsare obtained when possible. Depending on the clinicalquestions, additional imaging may be obtained to assessvalvular function or pulmonary pressures.The interpretation of stress echo is primarily qualitative, onthe basis of the visual comparison of systolic wall motionand thickening prestress, during stress and peak stress orimmediately after stress in case of treadmill exercise stressechocardiography. Utilization of contrast to improve endocardial delineation improves diagnostic accuracy whiledecreasing the frequency of nondiagnostic studies [8,9].Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
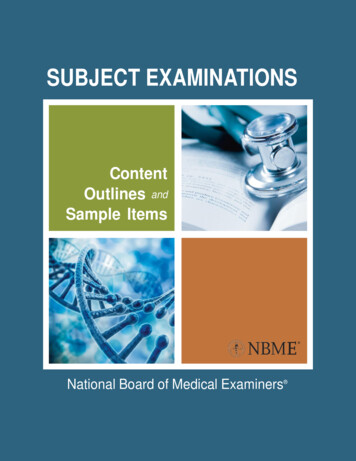
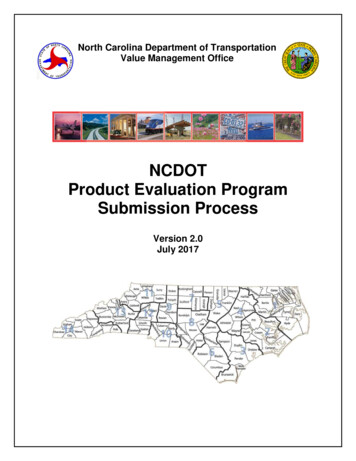
616 Coronary Artery Disease 2013, Vol 24 No 7Fig. ppropriateChest painNoroChECG interpretableand able to termeor h diateighAppropriateRole of stress echocardiography in the management of acute and chronic chest pain [5]. ACS, acute coronary syndrome.Rest and stress images are reviewed side by side over severalsuccessive cardiac cycles and compared for the development of: (i) new regional wall motion abnormalities,(ii) worsening of existing baseline wall motion abnormalities,(iii) global systolic left ventricular dysfunction, or (iv) leftventricular dilatation. A normal response to stress involvesincreased systolic wall thickening and systolic function(hyperkinesis) and decreased left ventricular size comparedwith rest. Ischemic response is characterized by new orworsening regional wall motion abnormalities (hypokinesis,akinesis, or dyskinesis) usually in at least two adjacent wallsegments. The severity of stress-induced ischemia isproportional to the site, extent, and severity of wall motionabnormalities. Stress-induced global systolic left ventriculardysfunction or left ventricular dilatation is indicative ofsevere coronary artery disease, including left main ormultivessel disease. Table 3 summarizes the major responsepatterns in stress echocardiography.Diagnostic role of stress echocardiographyMeta-analyses of many clinical studies have shown thatboth exercise and pharmacologic stress echo haveexcellent sensitivity and specificity for the detection ofcoronary artery disease. Overall, the sensitivity of stressechocardiography ranges from 80 to 86% and thespecificity ranges from 84 to 92% [3,7,10–12]. Of note,the sensitivity of stress echocardiography is lower inpatients with one-vessel disease (66–83%), especially leftcircumflex or right coronary artery disease, and increasesconsiderably with multivessel disease (86–90%) [7]. Themajor causes of false-positive or false-negative resultswith stress echocardiography are presented in Table 4.Safety and contraindications of stressechocardiographyBoth exercise and pharmacological stress echocardiography are considered to be safe and well-tolerated tests[3]. Major complications such as myocardial infarction,death, severe hypotension, high-grade atrioventricularblock, malignant ventricular arrhythmias, and bronchospasm occur in B1 : 1000 procedures. Minor but limitingside effects occur in less than 10% of patients withdobutamine and less than 5% of patients with dipyridamole stress. Dobutamine stress echo should be avoided inpatients with current atrial or ventricular arrhythmia andsevere hypertension. Adenosine or dipyridamole stressecho is not indicated in patients with high-grade heartblock, hypotension, active bronchospasm, and thosereceiving caffeine or theophylline. Antianginal medications (b-blockers in particular) significantly reduce thediagnostic accuracy of stress echocardiography; therefore,it is recommended whenever possible to withhold suchmedications before the test to avoid false-negativeresults [3].Strengths and weaknesses of stress echocardiographyStress echocardiography is a safe, nonionizing, versatile,and inexpensive imaging technique with adequatediagnostic and prognostic value in coronary artery disease.However, it has several weaknesses including dependence on image quality, level of achieved stress, use ofantianginal medication, relatively high interobservervariability in image interpretation, and reduced sensitivity for the assessment of ischemia in patients with restingwall motion abnormalities or multivessel disease [7].Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Echocardiography and coronary artery disease Chatzizisis et al. 617bubbles can pass through the pulmonary microcirculationand concentrate in the myocardium proportionate to therelative myocardial blood volume within the correspondingMyocardial contrast in stress echocardiographyIn addition to facilitating improved endocardial delination,advances in ultrasound contrast agents and technologyhave enabled the detection of myocardial hypoperfusion,which may exist before the development of overt regionalor global systolic dysfunction [9,13]. The evaluation ofmyocardial perfusion with echocardiography involves theintravascular injection of contrast agents that scatterultrasound waves [13]. Ultrasound contrast agents generally consist of microbubbles with a diameter of less than8 mm made of surfactant, human albumin, or natural lipidscontaining a high-molecular-weight gas (e.g. sulfurhexafluoride, perfluoropropane). Because of their smallsize, comparable with a red blood cell, these micro-Table 4 Causes of false-positive and false-negative stressechocardiogramsFalse negativesFalse positivesInadequate stressAntianginal treatment (b-blockers)Mild stenosesLeft circumflex diseasePoor image qualityDelayed images after stressOverinterpretation, interpretation biasLocalized basal inferior wall abnormalitiesAbnormal septal motion (e.g. left bundlebranch block, right ventricular pacing)CardiomyopathiesHypertensive responses to stressReproduced with permission [7].Fig. 3(a)BaselineBruce protocolRecoveryTime (min)EchoEchoEchoECG & blood pressureAtropine(max. 2 mg)(b)40302010BaselineDobutamine (mcg/kg/min)0Echo36Echo9Recovery12EchoTime (min)EchoECG & blood pressureStress echocardiography protocols with exercise (a) and dobutamine (b).Table 3Response patterns in stress isAkinesisAkinesis, dyskinesisPeak stressDiagnosisHyperkinesisHypokinesis, akinesis, dyskinesis, global hypokinesisa, LV dilatationaHypokinesis, normokinesisBiphasic responsebAkinesis, dyskinesisNormal myocardiumIschemic myocardiumViable stunned myocardiumViable hibernating myocardiumNecrotic (nonviable) myocardiumLV, left ventricular.aGlobal hypokinesis or LV dilatation with stress indicate left main or three-vessel disease.bBiphasic response involves initial improvement with low-dose dobutamine and subsequent worsening with increased doses of dobutamine.Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
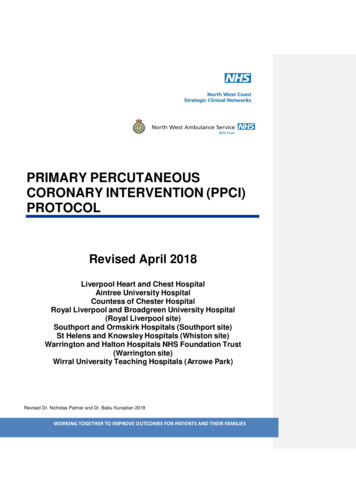
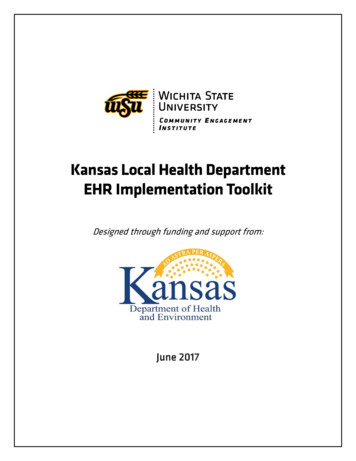
618 Coronary Artery Disease 2013, Vol 24 No 7regional myocardial microvasculature. Harmonic imagingtechniques enable longer persistence of microbubblecontrast and improved signal/noise ratios [14].Studies have proved the ability of stress myocardial contrastechocardiography to evaluate the presence and the extentof coronary artery disease during exercise or infusion ofinotropic or vasodilator agents [13,15]. Because microbubbles remain entirely intravascular, when the infusion ofa contrast agent is continuous, echocardiographic signalintensity reflects myocardial microcirculatory blood volume. During stress, the capillary blood volume decreasesdistal to flow-limiting stenoses, resulting in reduction ofmyocardial signal intensity and contractility in segmentssubtended by the diseased coronary branch (Fig. 4) [16].Diastolic stress testingIschemia-induced diastolic dysfunction can also beassessed by a stress test (i.e. ‘diastolic stress testing’).Normally, both E wave velocity in transmitral Dopplerand Ea wave velocity in tissue Doppler, which reflects thediastolic relaxation of mitral annulus, increase withexercise, thereby resulting in a stable E/Ea ratio betweenrest and exercise. Induced diastolic dysfunction inischemic myocardium leads to decreased mitral annulusrecoil and therefore reduced Ea wave velocities. As aresult, the E/Ea ratio may increase with exercisecompared with rest [17–19]. The utility of diastolicstress testing in the diagnosis of myocardial ischemiawarrants further clinical investigation.Emerging methodsThree-dimensional echocardiographyAlthough researchers have been developing methods forthree-dimensional echocardiography since the early1970s [20], recent advances have enabled real-timevolumetric acquisitions [21]. Initial methods requiredmanual rotation of the transducer to sequentially collectimages in multiple planes, which were then reconstructedoffline. Although mechanized transducers eliminated theneed for manual probe rotation, three-dimensional datasetscontinued to be reconstructed from two-dimensional dataacquired across multiple cardiac cycles. Advances inmaterial science, parallel processing electronics, and software have enabled the development of phased arraytransducers that can image large pyramidal volumes in realtime [22]. Corresponding improvements in software haveenabled both online and offline visualization of volumetricdatasets. As a result, three-dimensional imaging is now aroutine part of both transthoracic and transesophagealechocardiography protocols in many laboratories.For the evaluation of coronary artery disease, there are severalimportant advantages for three-dimensional volumetricimaging over two-dimensional echocardiography. All ofthe standard two-dimensional views can be reconstructedfrom a small number of three-dimensional acquisitions [23]. Volumetric datasets also allow more reliableand accurate quantification of chamber volume and mass(Fig. 5) [24,25]. The ability to rapidly and simultaneousacquire multiple views may simplify stress echocardiography [26] and may improve diagnostic accuracy [27].Tissue Doppler imaging and speckle tracking methodsQualitative and quantitative evaluations of systolicfunction with traditional measures, such as left ventricular ejection fraction, may be insensitive for theidentification of subclinical decreases in systolic function,which may be signs of incipient coronary disease.Furthermore, traditional measures of systolic functiondo not reflect abnormalities in diastolic function, whichmay be important markers of disease. Two methods holdpromise in this area: tissue Doppler imaging and speckletracking. As in traditional pulse Doppler imaging, tissueDoppler imaging measures the velocities in a region ofinterest. However, in contrast to traditional pulseDoppler imaging, a low-pass filter is applied to exclude high-velocity signals from moving blood, enablingmeasurement of myocardial tissue velocities [28,29].From the myocardial tissue velocities, strain and strainrates can be computed. Speckle tracking methods usecomputer algorithms to evaluate changes in distanceFig. 4RestStressSpectAngioRepresentative myocardial contrast echocardiogram showing a myocardial perfusion defect in the anteroseptal and apical segments of the leftventricle (black arrows) during adenosine stress imaging. The corresponding coronary angiogram shows the presence of significant coronary arterydisease in the left anterior descending artery (grey arrows). Reprinted with permission from Xie et al. [16].Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Echocardiography and coronary artery disease Chatzizisis et al. 619Fig. 5EDV 153.15 mlESV 66.39 mlSV 86.76 mlEF 56.65 %Three-dimensional echocardiography. The two-dimensional image data can be contoured semiautomatically to generate three-dimensionalrepresentations of the left ventricle and allow precise estimates of chamber volumes and ejection fraction. EDV, end-diastolic volume;ESV, end-systolic volume; SV, stroke volume; EF, ejection fraction.between ‘speckles’ observed in normal myocardium tocompute the strain and the strain rate [30] (Fig. 6).Both tissue Doppler imaging and speckle trackingmethods have been used for assessment of systolic anddiastolic dysfunction in the setting of coronary arterydisease [28,31]. Tissue Doppler imaging is routinely usedto quantify early and late mitral annual relaxation velocity,an important measure of diastolic function. Althoughused less often, mitral annual systolic velocity may be asensitive measure for early abnormalities in systolicfunction [32]. Tissue Doppler imaging and speckletracking can be used to quantify myocardial strain andstrain rate, which may be abnormal even in the setting ofthe overall normal ejection fraction. Both these methodshave been applied to stress testing to improve diagnosticperformance in coronary artery disease [33].Currently, most echocardiography systems include capabilities for acquiring and analyzing tissue Dopplerimaging images. Software for speckle tracking is availablefrom multiple vendors both for offline and for real-timeanalysis. However, because speckle tracking analysis istime consuming, few laboratories have integrated it intoroutine workflows.Acute myocardial ischemiaResting two-dimensional echocardiographyTable 2 and Fig. 2 summarize the appropriate use criteriaof echocardiography in acute coronary syndromes [5].Resting two-dimensional echocardiography is a usefuland inexpensive tool for the assessment of acute chestpain. Normal overall left ventricular systolic contractilefunction without regional wall motion abnormalitiesduring acute chest pain excludes large regions ofmyocardial ischemia or infarction, whereas the development of new regional wall motion abnormalities in thesetting of acute chest pain is of major concern for ongoingmyocardial ischemia or infarction. Contrast-enhancedimaging appears to further aid the assessment of regionalwall motion abnormalities [9]. Because of limitations inspatial resolution, inadequate acoustic windows in manypatients, and the fact that early or mild hypoperfusionmay exist without overt systolic dysfunction, resting twodimensional echocardiography is generally consideredinadequate to rule out the presence of functionallysignificant coronary artery disease, especially in theabsence of ongoing chest pain or ECG signs of ischemia[17,34]. Nonetheless, this method can be very helpful inthe acute setting to rule out alternative cardiac andnoncardiac causes of acute chest pain, including pericardial effusion, pulmonary embolism, or aortic dissection.Stress echocardiographyStress echocardiography provides invaluable diagnosticinformation in acute chest pain patients with no ischemicchanges or with left bundle branch lock or pacedventricular rhythm and negative or minimally elevatedtroponin levels (Table 2 and Fig. 2) [5].Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
620 Coronary Artery Disease 2013, Vol 24 No 7Fig. 6VelocityDisplacementStrainStrain rate(Accuracy 4.324)Radial strain (endo)0968 ms.67.00053.600(a)(b)40.20026.80010.242 18813.4000.000 13.400 26.800 40.200% 53.600 67.000ms.130260390120.000dV/dt650780(Accuracy 3.055)Longitudinal strain (endo)EF 83% edlvm 139.85 g eslvm 96.89 g0968 ms.Volume5200968 000.00057.600 97.20047.200 194.40036.800 291.60026.400 388.8000.000 9.800 19.600 29.40016.000ms.130260390520650780910 486.000% 49.000ms.130260390520650780910ml/sml. 39.200Speckle tracking imaging. After tracing the myocardium in the apical four-chamber view (a), radial (b) and longitudinal (c) strain measures for eachsegment can be plotted as a function of time across the cardiac cycle and presented as a maps.Myocardial contrast echocardiographyMyocardial contrast echocardiography can assess directlyboth the myocardial tissue perfusion and wall motion atthe bedside, playing a unique role in the diagnosis andprognosis of acute coronary syndromes [35,36]. Of note,because the use of ultrasound contrast for this applicationhas not received regulatory approval in the USA, althoughmany laboratories have gained considerable experiencewith research and clinical examinations, it has yet togarner widespread clinical acceptance.Emerging methodsSpeckle tracking imaging and diastolic relaxation ofischemic regions have also been used for the diagnosisof acute myocardial ischemia mostly in research applications [25]. Although these methods hold promise forimproved diagnostic accuracy and decreased inter-readervariability, they are not yet widely applicable and furtherinvestigation of their clinical utility is required.Complications of acute myocardial infarctionResting two-dimensional echocardiography with Dopplerimaging is the first-line imaging method for the diagnosis
echocardiography, ultrasound contrast agents, tissue Doppler imaging, and speckle tracking methods hold significant promise to further widen the scope of clinical applications and improve diagnostic accuracy. The purpose of this review is (i) to provide an update on the role of