Transcription
Tomi St. Mars,MSN, RN, CEN, FAENPediatric PreparedEmergency Care/ InjuryPrevention
Performance Measures #71 The percentage of prehospital provider agencies in thestate/territory that have online pediatric medical direction.#72 The percentage of prehospital provider agencies in thestate/territory that have offline pediatric medical direction.#73 The percentage of patient care units in the state/territory thathave essential pediatric equipment and supplies.#74 The percentage of hospitals with an emergency department(ED) recognized through a statewide, territorial, or regionalstandardized system that are able to stabilize and/or managepediatric medical emergencies.#75 The percentage of hospitals with an ED recognized through astatewide, territorial, or regional standardized system that are able tostabilize and/or manage pediatric traumatic emergencies.
#76 The percentage of hospitals with an ED in the state/territory thathave written interfacility transfer guidelines that cover pediatricpatients and that contain the following components of transfer: defined process for initiation of transfer, including the roles andresponsibilities of the referring facility and referral center (includingresponsibilities for requesting transfer and communication); process for selecting the appropriate care facility; process for selecting the appropriately staffed transport service to matchthe patient’s acuity level (level of care required by patient, equipmentneeded in transport, etc.); process for patient transfer (including obtaining informed consent); and plan for transfer of patient information (e.g. medical record, copy ofsigned transport consent), personal belongings of the patient, andprovision of directions and referral institution information to family. #77 The percentage of hospitals with an ED in the state/territory thathave written interfacility transfer agreements that cover pediatricpatients.
#78 The adoption of requirements by the state/territory for pediatricemergency education for the license/certification renewal of BLSand ALS providers.#79 The degree to which the state/territory has establishedpermanence of EMSC in the state/territory EMS system. The establishment of an EMSC Advisory Committee within thestate/territory that meets at least four times per year. The incorporation of pediatric representation on the state/territoryEMS Board. The establishment of a state/territory, federal, and/or otherfunded full-time EMSC manager that is dedicated solely to theEMSC Program.#80 The degree to which the state/territory has establishedpermanence of EMSC in the state/territory EMS system byintegrating EMSC priorities into statutes/regulations.
ArizonaEMS for Children’s program opted to focuson regionalization/standardizing 90% of pediatric patients treated in an EDaccess via the front door 10% arrive EMS Inclusive system improvement
Pediatric Prepared EmergencyCare April 2008 Stakeholder Meeting – Hospital CEOs,Emergency Department Leadership2008 – 2010: Stakeholder Committee Meetings – review andrefine criteriaLate 2010: Program transferred to AzAAP, Formal SteeringCommittee seatedDecember 2011: Initial site visitsMarch 2012: 7 Advanced Care sites, 2 Prepared Plus sitescertified by AzAAP BoardMay 2015: 36 Hospital Members, 26 Hospital EDs certified, 7reverification visits
AZ Goal – Inclusive System ofCare Voluntary System Developed by ED Nurses andPhysicians using the “Guidelines for Care of Children inthe Emergency Department”Three tiersSustainability: Membership and Certification FeesConsultation and EducationQuality Improvement
Levels of Care – Names notNumbers Prepared Care - This level of certification provides services forpediatric care as part of a general Emergency Department. Thehospital refers critically ill or injured children to other facilities andmay or may not have pediatric inpatient services available. Prepared Plus Care - This level of certification provides services formost pediatric emergency care. The hospital has a focus onpediatrics, but ICU services for children are not available. Prepared Advanced Care -This level of certification providesservices for all levels of pediatric emergency care. This hospitalsystem includes a Pediatric intensive care unit and has a specificfocus on pediatric services.
Criteria Example Physicians staffing Board-eligibleor Board-certified in one of theallopathic or osteopathic boardsof: Emergency Medicine,Pediatric Emergency Medicine,Pediatrics, Internal Medicine orFamily Medicine.4 hours of pediatric CME annuallyNon-board-certified physiciansare required to have current PALSor APLS certification. Nursing staff must be licensed inthe State of Arizona or multistatecompact privilege.All nursing staff shall have PALSor ENPC certification within 6months of hire.4 hours of pediatric CME annually
Cont QI review:All transfers outAll pediatric deathsAll childabuse/maltreatmentRequired Equipment GuidelinesDisasterTransfersAbuseSedationPatient safety Medication Weights ALARAin KG
Membership Benefits Members discussion forum Free educational classes and trainings members share guidelines, procedures, issues and questionsCertified Emergency Nurse Review CoursesEmergency Nursing Pediatric CoursesAdvanced Pediatric Life Support, Newborn ResuscitationProgram and/or STABLEIdentification and action on issues common to most or all EDsSite visit participants share learning
Arizona Wins . Life savedStandardizing careWeights in kilogramsImproved child abusepoliciesMock codesDisaster preparednessEquipment in placeClinical pathways sharedImproved flow Next Steps – Full set of vital signs onall kids% nurses with CEN,CPENPostmortem guidelinesIdentify joint QI targetsContinue to bump thebar moving evidence topractice faster
Trauma Centers/PPEC HonorHealth Scottsdale OsbornMedical CenterMaricopa Medical CenterPhoenix Children’s HospitalBanner Baywood Medical CenterBanner University Medical Center –Tucson CampusTuba City RegionalHealth Care Corp.Banner Boswell Medical CenterBanner Del E. Webb Medical CenterBanner Estrella Medical CenterBanner Gateway Medical CenterBanner Ironwood Medical CenterBanner Page Hospital Banner Gateway Medical CenterBanner Ironwood Medical CenterBanner Page HospitalHonorHealth Deer Valley MedicalCenterChinle Comprehensive Health CareFacilityCobre Valley Regional Medical CenterCopper Queen Community HospitalMt. Graham Regional Medical CenterNorthern Cochise Community HospitalOro Valley HospitalSummit Healthcare Regional MedicalCenterWhite Mountain Regional MedicalCenter
PPEC-Verified Arizona Children's Center at MaricopaMedical CenterBanner Thunderbird Medical CenterBanner University Medical Center-TucsonCardon’s Children’s Medical CenterPhoenix Children’s HospitalScottsdale Healthcare- Shea Medical CenterTucson Medical Center for ChildrenHonorHealth Deer Valley Medical CenterMendy’s PlaceMercy Gilbert Medical CenterHonorHealth Scottsdale Osborn MedicalCenterHonorHealth Scottsdale Thompson PeakMedical CenterSummit Healthcare Regional Medical CenterYuma Regional Medical Center Abrazo Central CampusBanner Baywood Medical CenterBanner Boswell Medical CenterBanner Del E. Webb Medical CenterBanner Estrella Medical CenterBanner Gateway Medical CenterBanner Goldfield Medical CenterBanner Ironwood Medical CenterBanner Page HospitalChinle Comprehensive Health Care FacilityCobre Valley Regional Medical CenterCopper Queen Community HospitalNorthern Cochise Community HospitalOro Valley HospitalTuba City Regional Health Care CorporationWhite Mountain Regional Medical Center
Questions?
Injury Prevention
RoleStatewide and local injury data collection Provide leadership Program development and implementation Training and education Public information Policy Surveillance
Injury Prevention DataEmergency department, hospitalizationsand death Only Arizona residents Tribal/Federal facilities CDC methodology
In 2014, an average week of injuries inArizona resulted in approximately:89 resident deaths 714 inpatient hospitalizations 7,766 emergency department visits
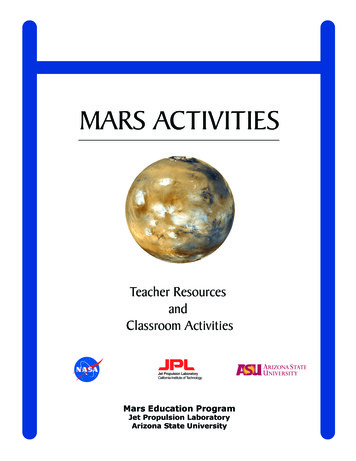
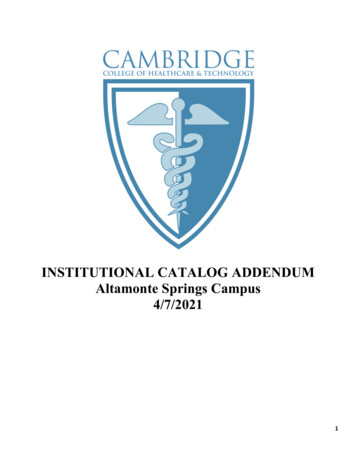
Injuries in Arizona 2014Numberof Deaths1,123Age-AdjustedRatePer 100,000population16.597715.03 Unintentional Falls4 Motor Vehicle Traffic Crashes88011.76509.55 Homicide6 Unintentional Suffocation2924.61241.77 Unintentional Natural/Environment8 Unintentional Drowning591.4781.2500.7300.4Rank Cause of Injury Death1 Suicide2 Unintentional Poisoning9 Other Land Transport/Transport10 Unintentional Fire/FlameSource: Arizona Vital Records, 2014
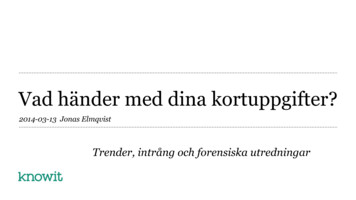
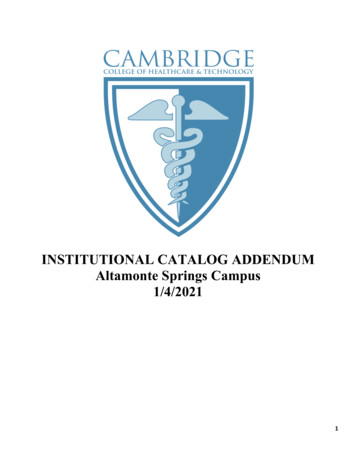
Arizona Has Higher Injury Mortality RatesCompared to the United States
Levels of Evidence-based Public HealthStrategies Best or Effective Practices indicate there is strong evidence the intervention works.There are sustainable, replicable programs that have demonstrated positive impacton prevention, costs and /or other stated outcomes. Promising Practices indicate there is some evidence the intervention is effective, butadditional research is needed in multiple settings to determine their full impact oreffectiveness. Innovative Practices are cutting edge efforts that are untested or locally developed inwhich there is currently insufficient evidence to determine their impact. Untested Practices have not been evaluated or documented. If a particular strategy isnot considered evidence-based, it does not mean the strategy is ineffective, butrather additional study is needed to determine whether the intervention is effective.
Community Guide The Task Force on Community Preventive Services is anindependent, nonfederal, volunteer body of experts inpublic health and prevention research, practice andpolicy, appointed by the CDC Director to:‹Prioritize topics for systematic review ‹Oversee systematic reviewsdone for the Community Guide ‹Develop evidence-basedrecommendations using the systematic review results ‹Identifyareas that need further research http://www.thecommunityguide.org/mvoi/index.html
What Questions Does the Task Force Askabout Interventions? Does it work? ‹How well? ‹For whom? ‹Under whatcircumstances is it appropriate?What does it cost?Are there barriers to its use?Are there any harms?Are there any unanticipated outcomes?
What Do the Findings Mean? Recommended– strong or sufficient evidence that theintervention is effective.Recommended Against– strong or sufficient evidencethat the intervention is harmful or not effective.Insufficient Evidence – the available studies do notprovide sufficient evidence to determine if theintervention is, or is not, effective.
What Does “InsufficientEvidence” Mean?Insufficient evidence means that additionalresearch is needed to determine whetheror not the intervention is effective. This does NOT mean that the interventiondoes not work.
Insufficient Evidence Findings In some cases there are not enough studies todraw firm conclusions. Reasons include:‹A lack of studies, or a lack of studies withrigorous methodsIn other cases, there are a sufficient number ofstudies, but the findings are inconsistent.Reasons include:‹Confounding variables or inconsistency in howthe intervention was implemented in studies
Insufficient EvidenceFindings and Research One major use of Insufficient Evidence findingsis to influence future research. These findingscan:‹Identify promising, but understudied, topics withimportant public health implications‹Help to allocate scarce research funds tothose topics, which might otherwise beallocated to topics where strong orsufficient evidence already exists
http://www.sprc.org
ChallengesFeels good-short term gratification Resource intensive Funding risks Credibility
ResourcesIPAC meets quarterly Safe States Safestates.org HospitalSIGCDC SAMHSA ADHS-Office of Injury Prevention
Questions?
MSN, RN, CEN, FAEN Pediatric Prepared Emergency Care/ Injury Prevention. Performance Measures . emergency education for the license/certification renewal of BLS and ALS providers. . Certified