Transcription
SPECIAL ARTICLEA Perspective on the New American Collegeof Cardiology/American Heart AssociationGuidelines for Cardiovascular Risk AssessmentIftikhar J. Kullo, MD; Jorge F. Trejo-Gutierrez, MD, MHS;Francisco Lopez-Jimenez, MD, MSc; Randal J. Thomas, MD, MSc;Thomas G. Allison, PhD, MPH; Sharon L. Mulvagh, MD;Adelaide M. Arruda-Olson, MD, PhD; Sharonne N. Hayes, MD;Amy W. Pollak, MD; Stephen L. Kopecky, MD; and R. Todd Hurst, MDAbstractThe recently published American College of Cardiology (ACC)/American Heart Association (AHA)guidelines for cardiovascular risk assessment provide equations to estimate the 10-year and lifetimeatherosclerotic cardiovascular disease (ASCVD) risk in African Americans and non-Hispanic whites,include stroke as an adverse cardiovascular outcome, and emphasize shared decision making. Theguidelines provide a valuable framework that can be adapted on the basis of clinical judgment and individual/institutional expertise. In this review, we provide a perspective on the new guidelines, highlighting what is new, what is controversial, and potential adaptations. We recommend obtaining familyhistory of ASCVD at the time of estimating ASCVD risk and consideration of imaging to assess subclinicaldisease burden in patients at intermediate risk. In addition to the adjuncts for ASCVD risk estimationrecommended in the guidelines, measures that may be useful in refining risk estimates include carotidultrasonography, aortic pulse wave velocity, and serum lipoprotein(a) levels. Finally, we stress the need forresearch efforts to improve assessment of ASCVD risk given the suboptimal performance of available riskalgorithms and suggest potential future directions in this regard.ª 2014 Mayo Foundation for Medical Education and ResearchAssessment of cardiovascular risk is anecessary first step to target therapytoward patients most likely to benefit.It has become evident that baseline atherosclerotic cardiovascular disease (ASCVD) risk is abetter predictor of treatment benefit than thedegree to which low-density lipoprotein cholesterol (LDL-C) is lowered.1,2 The recently published American College of Cardiology (ACC)/American Heart Association (AHA) guidelinesfor cholesterol lowering3 emphasize that the intensity of risk factor management should matchthe risk for adverse ASCVD events. In contrast,previous guidelines have favored achievingtarget LDL-C levels based on the magnitude ofestimated cardiovascular risk.4The most recent ACC/AHA guidelines include a new ASCVD risk calculator for use inthe clinical setting and address questions relevant to risk assessment using critical review ofthe available literature. The document includesnMayo Clin Proc. 2014;nn(n):1-13a disclaimer that the recommendations arenot a substitute for clinical judgment andthat decisions about care must be individualized for each patient. The guidelines provide avaluable framework that can be adapted onthe basis of clinical judgment and individual/institutional expertise. In this review, we provide a perspective on the new guidelines forassessing risk of ASCVD events in adultswithout known disease, highlighting what isnew, what is controversial, and potential futuredirections (Table 1).Preventive cardiologists from throughout theMayo Foundation contributed to this document.A core writing group reviewed the guidelines andexisting literature and made modifications basedon foundation-wide expertise in cardiovascularrisk assessment including imaging, circulatingbiomarkers, and genetic epidemiology. Input tothe draft was provided by each author, and afterseveral revisions, the draft was circulated to aMayo Clin Proc. n XXX 2014;nn(n):1-13 n mayoclinicproceedings.org n ª 2014 Mayo Foundation for Medical Education and ResearchFor editorialcomment, seepage XXX.From the Division ofCardiovascular Diseases,Mayo Clinic, Rochester,MN (I.J.K., F.L.-J., R.J.T.,T.G.A., S.L.M., A.M.A.-O.,S.N.H., A.W.P., S.L.K.);Division of CardiovascularDiseases, Mayo Clinic,Jacksonville, FL (J.F.T.-G.);and Division of Cardiovascular Diseases, MayoClinic, Scottsdale, AZ(R.T.H.).1
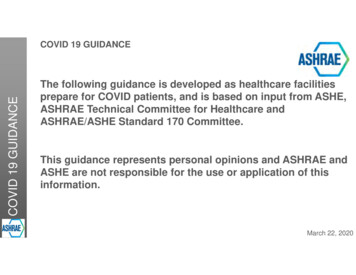
MAYO CLINIC PROCEEDINGSadjudicated end points for fatal or nonfatalmyocardial infarction and stroke (Figure 1).The cohorts include the ARIC (AtherosclerosisRisk in Communities) study,12,13 the Cardiovascular Health Study,14 and the CARDIA (Coronary Artery Risk Development in YoungAdults) study,15 combined with applicabledata from the Framingham and FraminghamOffspring study cohorts.16,17 The strongest predictors of the 10-year risk of “hard” ASCVDevents (defined as first occurrence of nonfatalmyocardial infarction or CHD death or fatalor nonfatal stroke)18 were age, sex, race, totalcholesterol, high-density lipoprotein cholesterol, systolic blood pressure, blood pressuretreatment status, diabetes, and current smokingstatus. An “app” has been developed that can beused online or on a mobile device to estimate apatient’s 10-year ASCVD risk.19ARTICLE HIGHLIGHTSnnThe availability of race- and sex-specific equations for estimating10-year and lifetime atherosclerotic cardiovascular disease(ASCVD) risk, inclusion of stroke as an adverse cardiovascularoutcome, and the emphasis on shared decision making arestrengths of the new American College of Cardiology/AmericanHeart Association guidelines for ASCVD risk assessment.The guidelines recommend 4 measures that may be consideredby clinicians and patients as adjuncts for refining risk estimatesdfamily history of ASCVD, high-sensitivity C-reactive protein, ankle-brachial index, and coronary artery calcium scoring.nAdditional measures that may be useful in risk estimationinclude carotid ultrasound, aortic pulse wave velocity, andcirculating levels of lipoprotein(a).nBecause of the suboptimal performance of available ASCVD riskalgorithms, research efforts to improve risk assessment inasymptomatic adults should be intensified.wider group. Feedback was incorporated iteratively until consensus was reached.WHAT IS NEW IN THE GUIDELINES?New Equation for Estimating 10-Year Risk ofASCVD EventsPopulation-based studies have identified factorsassociated with incident adverse cardiovascularevents.7 These risk factors have been includedin multivariate risk scores for not only coronaryheart disease (CHD) but also stroke, peripheralarterial disease, and heart failure as well as composite cardiovascular disease end points.8 Mostof these risk calculators estimate a patient’s probability of having a vascular event over 5 to 10years.9 The commonly used risk scores includethe Framingham CHD risk score,10 its derivative,the Adult Treatment Panel III (ATP-III) riskassessment profile,4 and the European SystematicCoronary Risk Evaluation (SCORE)11 algorithmfor ASCVD death. These risk equations werederived from cohorts that were established decades ago and had limited ethnic diversity.The new ASCVD risk calculator was developed from several relatively recently establishedpopulation-based cohorts that included AfricanAmerican or non-Hispanic white participantswith at least 12 years of follow-up and with2Mayo Clin Proc.nRecommended Adjuncts to Refine RiskEstimatesAdditional variables were tested for inclusionin the model if they were available in the databases and could be evaluated on the basis ofat least 10 years of follow-up, using theframework suggested by Hlatky et al.20 Thesevariables included diastolic blood pressure,family history of ASCVD, moderate or severechronic kidney disease (defined as an estimated glomerular filtration rate of 60 mL/min per 1.73 m2),21 and body mass index(continuous or categorical). None of thesevariables significantly improved predictionof 10-year ASCVD events when added tothe final base models. The guidelines recommend 4 markers that may be considered byclinicians and patients if uncertainty remainsafter calculating the 10-year ASCVD riskdfamily history, high-sensitivity C-reactive protein (hs-CRP), ankle-brachial index (ABI), andcoronary artery calcium (CAC) score.Focus on Hard ASCVD EventsCompared with earlier guidelines, the new riskassessment guidelines attempt to take into account that atherosclerosis is a chronic diseasethat affects multiple vascular beds. Risk isestimated for “hard” ASCVD events includingstroke, myocardial infarction, and death dueto stroke or myocardial infarction. “Soft” endpoints such as those that might be influencedby physician preferences (eg, revascularizationXXX .2014.06.018www.mayoclinicproceedings.org
A PERSPECTIVE ON CARDIOVASCULAR RISK ASSESSMENTTABLE 1. Summary of ACC/AHA Recommendations for ASCVD Risk AssessmentaACC/AHA recommendationNHLBI gradeLOEACC/AHACORCommentsb1. The race- and sex-specific Pooled Cohortequations to predict 10-y risk for a first hardASCVD event should be used in non-HispanicAfrican Americans and non-Hispanic whitesaged 40-79 y2. Use of the sex-specific Pooled Cohortequations for non-Hispanic whites may beconsidered when estimating risk in patients frompopulations other than African Americans andnon-Hispanic whites3. If, after quantitative risk assessment, a risk-basedtreatment decision is uncertain, assessment of 1or more of the followingd family history, hsCRP, CAC score, or ABIdmay be consideredto inform treatment decision making4. The contribution to risk assessment for a firstASCVD event using ApoB, CKD, albuminuria,or CRF is uncertain at presentB (moderate)BIAlong with the use of the ASCVD risk calculator,family history of ASCVD should be obtained asfirst step in estimating risk of ASCVDE (expert opinion)CIIbE (expert opinion)BIIbThe accuracy of the ASCVD risk calculator is notestablished for Asian and Hispanic Americans.Among Asian Americans, those from the Indiansubcontinent may be at higher risk than otherethnic groupsIt is reasonable to consider additional modalities asadjuncts for risk stratification. See Tables 2 and 3for further recommendationsN (no recommendationfor or against)NANA5. CIMT is not recommended for routinemeasurement in clinical practice for riskassessment for a first ASCVD eventN (no recommendationfor or against)BIIIBIIaCIIb6. It is reasonable to assess traditional ASCVD risk B (moderate)factors every 4-6 y in adults aged 20-79 y whoare free from ASCVD and to estimate 10-yASCVD risk every 4-6 y in adults aged 40-79 ywithout ASCVD7. Assessing 30-y or lifetime ASCVD risk based on C (weak)traditional risk factors may be considered inadults aged 20-59 y without ASCVD who arenot at high short-term riskAssessment of CRF may be useful in prescribing anexercise regimen for patients. Although CRF haslimited sensitivity for detecting early coronaryartery disease, it provides prognosticinformation independent of conventional riskfactorsSelective use of carotid ultrasonography for plaquedetection and measurement of common CIMTis reasonable to consider as an adjunct for riskestimation; the test should be performedfollowing standardized protocols and establishedguidelinesEstimates of lifetime risk consider risks factorspresent at age 50 and therefore do not trulyreflect the lifetime risk of those younger than 50 y,as their risk factors will likely change over time30-y or lifetime ASCVD risk estimates should beused primarily to motivate patients regardinglifestyle changes but may also inform decisionsrelated to statin therapy, particularly in youngerindividualsABI ¼ ankle-brachial index; ACC ¼ American College of Cardiology; AHA ¼ American Heart Association; ApoB ¼ apolipoprotein B; ASCVD ¼ atherosclerotic cardiovascular disease; CAC ¼ coronary artery calcium; CIMT ¼ carotid intima-media thickness; CKD ¼ chronic kidney disease; COR ¼ class of recommendation; CRF ¼cardiorespiratory fitness; hs-CRP ¼ high-sensitivity C-reactive protein; LOE ¼ level of evidence; NA ¼ not applicable; NHLBI ¼ National Heart, Lung, and Blood Institute.bThese are expert statements not necessarily based on systematic review of evidence.aprocedures) and end points that are often difficult to ascertain reliably (eg, angina and heartfailure), were not included.Recommendations for Estimating LifetimeRiskThe ACC/AHA guidelines have a primary focuson 10-year risk of ASCVD events and a secondaryfocus on assessing lifetime risk for adults 20 to 59Mayo Clin Proc. n XXX 2014;nn(n):1-13www.mayoclinicproceedings.orgnyears old who are not at high short-term risk.Beginning at age 40, formal estimation of the10-year risk for ASCVD is recommended. Longterm or lifetime risk estimation is recommendedfor all persons who are 20 to 39 years of ageand for those 40 to 59 years old who are at low10-year risk ( 7.5%). At present, there is insufficient evidence for initiating pharmacologicaltherapy on the basis of lifetime risk .06.0183
MAYO CLINIC PROCEEDINGSpatient’s risk for ASCVD and potential reduction of risk with drug therapy, adverse effectsfrom statins, cost of drug therapy, and patientpreferences related to preventive measures.The document acknowledges that no data areavailable to document that such an approach reduces adverse cardiovascular outcomes. Riskassessment combined with counseling hasbeen associated with favorable but modestchanges in patient knowledge and intention tochange and with physician prescribing behaviorand risk factor control.22,2324,626 Individuals aged 40-79y, free ofknown ASCVD, from ARIC,FHS, CARDIA, CHS cohorts11,240 White women9098 White men2641 African American women1647 African American men12-y follow-up for ASCVDeventsIncident ASCVD events902 in white women1259 in white men290 in African American women238 in African American menLIMITATIONS AND CONTROVERSIAL AREASRelatively Small African American CohortsInclusion of race-specific estimates of ASCVDrisk is a welcome new feature of the guidelines.However, in the cohorts used for derivingASCVD risk equations, there are nearly 5 timesmore white individuals than African Americanindividuals (Figure 1). Data from additionalAfrican American cohorts may be needed to increase the precision of risk estimates in AfricanAmericans.Multivariate regressionIndependent predictorsAge, sex, SBP, hypertensiontreatment status, T2D, current smoking,total and high density lipoproteincholesterolValidationLack of Multivariate Equations for Asian andHispanic AmericansSufficient data were not available for additionalrace/ethnic groups (Asians and Hispanics) toallow development of separate risk equations.When compared with non-Hispanic whites,the risk for ASCVD differs in Hispanic American,24 Asian American,25 and American Indianpopulations. For example, there is considerableheterogeneity in ASCVD risk among Asian populations, and those from the Indian subcontinentare considered to be at higher risk.25 Given theabsence of data, the guidelines recommend theuse of equations derived from non-Hispanicwhites in these ethnic groups, cautioning thatthe resulting risk estimates may be less accurate.FIGURE 1. Derivation and validation of theatherosclerotic cardiovascular disease (ASCVD)risk calculator using pooled cohorts. Participantswho met the following criteria were included:40 to 79 years of age, apparently healthy, andno history of nonfatal myocardial infarction(recognized or unrecognized), stroke, heartfailure, percutaneous coronary intervention,coronary artery bypass surgery, or atrial fibrillation. ARIC ¼ Atherosclerosis Risk in Communities study; CARDIA ¼ Coronary Artery RiskDevelopment in Young Adults; CHS ¼ Cardiovascular Health Study; FHS ¼ FraminghamHeart Study; SBP ¼ systolic blood pressure;T2D ¼ type 2 diabetes.but such information may be useful in motivatingyounger individuals to make lifestyle changesand healthy choices, including regular physicalactivity, healthy dietary patterns, and smokingcessation.Emphasis on Shared Decision MakingThe emphasis on shared decision making isan important new feature of the guidelines.The document encourages discussion of the4Mayo Clin Proc.nVariable Performance of the ASCVD RiskCalculator in Other CohortsSubsequent to the publication of the guidelines,investigators have tested the performance of theASCVD calculator in several cohorts. In 2 largecohorts of nurses and physicians, respectively,the ASCVD risk calculator performed suboptimally in terms of accuracy and discrimination,26overestimating risk by up to 100%. However, individuals in these cohorts were likely to engageXXX .2014.06.018www.mayoclinicproceedings.org
A PERSPECTIVE ON CARDIOVASCULAR RISK ASSESSMENTTABLE 2. Adjunctive Measures to Consider for Risk StratificationaVariableEvidenceThresholdFamily history Multiple studies have shown family History of ASCVD in firstof ASCVDhistory to be an independentdegree relatives: malepredictor of cardiovascular riskrelatives aged 55 y orfemale relatives aged 65 yCACIncreased CAC is associated with Scores 300 Agatston units or 75th percentile for ageadverse outcomes, and CACand sex are consideredscoring leads to considerableabnormal. NRI ¼ 23% forreclassification of risk. Among5-y risk in intermediate-riskavailable noninvasive tests, CACindividualsprovides the most incrementalinformation in individuals atintermediate riskABIAssociated with CHD risk and leads An ABI 0.9 is consideredabnormal; high ABI ( 1.4) isto considerable reclassification;also associated withamong men, the effect is toincreased risk5down-classify high-risk men;among women, the effect is toup-classify low-risk womenhs-CRPMultiple studies found hs-CRP to Levels 2 mg/L are consideredto be elevated. hs-CRP isbe associated with adverseassociated with other riskASCVD outcomesfactors such as obesity, andits predictive valuediminishes after adjustmentfor known risk factorsActionable next stepsAvailabilityShared decision makingThere is considerableregarding statin initiationvariability in obtainingand dose. Screening ofand documenting familyfirst-degree relativeshistory of ASCVDWidely availableShared decision makingregarding statin initiationand dose. Serialmeasurements are notrecommendedFeeFree 512 55bWidely availableShared decision makingregarding statin initiationand dose. Serialmeasurements are notindicated 559 99bLifestyle changes (diet,Widely availableexercise, and weightloss) reduce levels.Individuals with hs-CRPlevels 2 mg/L, LDL-Clevels 130 mg/dL, andno history of ASCVD ordiabetes benefited fromstatin medication in theJUPITER study6 76 17bABI ¼ ankle-brachial index; ASCVD ¼ atherosclerotic cardiovascular disease; CAC ¼ coronary artery calcium; CHD ¼ coronary heart disease; hs-CRP ¼ high-sensitivityC-reactive protein; JUPITER ¼ Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin; LDL-C ¼ low-density lipoprotein cholesterol;NRI ¼ net reclassification index.bMedicare reimbursement.ain healthy lifestyles and also to be taking lipidand blood pressureelowering medications. Ina randomly sampled contemporary cohort of30,239 adults from geographically diverse regions of the United States, 10,997 were eligiblefor statin drugs on the basis of the recent guidelines; observed and 5-year ASCVD risks predictedusing the ASCVD risk calculator were similar,with moderate to good discrimination.27 Kavousiet al28 applied the ACC/AHA, the ATP-III,4 andthe European Society of Cardiology29 guidelinesto a Dutch cohort of 4854 participants aged 55years or older who were recruited between1997 and 2001. The risk equations providedmodest discrimination; for example, in men, using the ASCVD risk calculator, the C statistic was0.67 for hard ASCVD events, 0.67 for hard CHDevents, and 0.76 for ASCVD mortality. Thesestudies highlight that the ASCVD risk equationsMayo Clin Proc. n XXX 2014;nn(n):1-13www.mayoclinicproceedings.orgnmay need to be recalibrated when used in nonUS populations as well as the need for additionalvalidation of the ASCVD risk equations.Adjunctive Measures for Risk StratificationAlthough an LDL-C level 160 to 189 mg/dL anda relatively high lifetime ASCVD risk can help indeciding whether to start statin therapy, 4 measures are recommended by the guidelines foruse when there is uncertainty about ASCVDrisk even after the risk calculator is used(Table 2). The following caveats should beconsidered when using these adjunctive measures for cardiovascular risk estimation.Family history. Family history is considered a“free genomic tool”30 but was not included inthe risk equations because definitions variedamong studies and information was 85
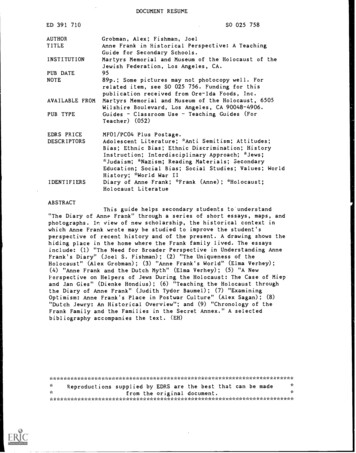
MAYO CLINIC PROCEEDINGSmissing. Although additional studies are neededto establish the extent to which family historyreclassifies risk, family history is meant to beroutinely obtained in the clinical setting and willbe useful as a supplement to the 10-year riskestimate. Increased awareness and documentation of family history of cancer and cardiovascular diseases are needed, as proposed in theCenters for Disease Control and Prevention’sFamily History Public Health Initiative.31Furthermore, documentation of family historywill be necessary to be compliant with meaningful use criteria for electronic medical records.Coronary Artery Calcium. Coronary arterycalcium is considered to be the most useful ofthe current adjunctive measures to improverisk assessment among individuals who are atintermediate risk according to the ASCVD riskcalculator. Uncertainty as to how CAC scorerelates to the 10-year risk of ASCVD and thelimited follow-up in available cohorts that havehad measurement of CAC make it a challengingto adjust ASCVD risk estimates on the basis ofthe CAC score.Ankle-Brachial Index. Although noninvasiveand inexpensive, the ABI is not a sensitive measure of lower extremity arterial disease. Sensitivity can be increased by measuring ABIs afterexercise, but this requires a treadmill exercisetest with electrocardiographic monitoring.Furthermore, the ABI is lower in women andAfrican Americans,32 and sex- and race-specificcutoffs for defining an abnormal ABI remain tobe established. In patients with diabetes, the ABIcan be elevated because of medial arterial calcification. Finally, the ABI may be useful only inolder persons, most of whom would alreadyhave been identified as being at higher risk by theASCVD risk calculator.High-Sensitivity C-Reactive Protein. The incremental predictive value of hs-CRP remainsunclear.33-39 Also controversial is whetherbaseline hs-CRP levels predict response tostatin therapy.40 Levels differ by race andsex.41 In the clinical setting, elevations in hsCRP often represent the presence of centralobesity, metabolic syndrome, estrogen use,recent infection, or trauma.42 The orderingphysician should be aware of these caveatsand interpret levels accordingly.6Mayo Clin Proc.nThreshold for Using StatinsThe guidelines recommend statin treatmentwhen the 10-year ASCVD risk is 7.5% or higherand consideration of therapy in those with a10-year risk between 5.0% and less than7.5%.3 The cut points were based on randomized controlled trials of statins that revealedreduction in adverse ASCVD outcomes at theselevels of risk.1 In the analysis by Kavousi et al,28the ACC/AHA guidelines would recommendstatins for nearly all men and two-thirds ofwomen older than 55 years, proportionsexceeding those based on the ATP-III or European guidelines. When such large proportionsmeet the treatment threshold, risk estimationbecomes redundant, and a “polypill” or universal treatment strategy comes into play.43Certainly in making decisions on potentiallylifelong therapy in mostly asymptomatic individuals, it is important to take into account patient choices.44 One option may be to expandthe intermediate risk category to 5% to 10%or even 5% to 15% and use adjunctive measures to further refine and individualize risk estimates to facilitate shared decision makingregarding statin use.45 Such an approach wouldneed further investigation to determine optimalscreening algorithms to minimize cost andhow to use the results of adjunctive testing torefine risk estimates downward (avoid treatment) or upward (and make a stronger casefor treatment).Using Information From Adjunctive Tests toModify 10-Year ASCVD RiskAdjunctive tests might improve risk assessmentin individuals at intermediate 10-year ASCVDrisk and in those who are at low risk ( 5%) buthave very high levels of a single risk factor, astrong family history of ASCVD, or chronic inflammatory disease (see 2 illustrative case studiesin Figure 2). Because of lack of data, no specificrecommendations can be made on how thesemarkers should be used to modify risk estimates.One proposed option is to replace the chronological age in the ASCVD risk calculator with the“vascular age” derived from imaging results.46Another option is to multiply the baselineASCVD 10-year risk by the hazard ratio (HR)associated with an abnormal result; for example,having a CAC score greater than the 75th percentile for age and sex could double the riskXXX .2014.06.018www.mayoclinicproceedings.org
A PERSPECTIVE ON CARDIOVASCULAR RISK ASSESSMENTCase 1A 47-year-old woman undergoing a general medicalevaluation is concerned about her atheroscleroticcardiovascular disease (ASCVD) risk given her familyhistory (her mother had ischemic stroke at age 53 years).The patient is asymptomatic and does not have diabetesor hypertension but smokes 5 cigarettes a day. Sheexercises 2 to 3 times a week on an elliptical machine.Her lipid profile includes a total cholesterol level of 198mg/dL (to convert to mmol/L, multiply by 0.0259),high-density lipoprotein cholesterol level of 48 mg/dL (toconvert to mmol/L, multiply by 0.0259), triglyceride level of110 mg/dL (to convert to mmol/L, multiply by 0.0113), andcalculated low-density lipoprotein level of 128 mg/dL (toconvert to mmol/L, multiply by 0.0259). On examination,the patient’s blood pressure is 128/76 mm Hg, andcardiovascular examination findings are unremarkable. Her10-year ASCVD risk is estimated at 4.1%, but given herfamily history of stroke, her physician orders carotidultrasonography to determine the intima-media thicknessand presence or absence of plaque. Her common carotidintima-media thickness is greater than the 75th percentilefor her age and sex, and she also has focal intimalthickening in both carotid bulbs. After a discussion of heroverall risk factor profile, family history, carotidultrasonographic findings, and the potential benefit, cost,and adverse effects of statins, she opts for moderateintensity statin therapy. She is also counseled to quitsmoking.Case 2A 56-year-old African American man who is an executiveis undergoing general medical evaluation includingscreening for cardiovascular disease. He is asymptomaticand exercises 4 times a week, 45 minutes each time. He isa nonsmoker and has no hypertension, diabetes, or familyhistory of ASCVD. His cardiovascular examination yieldsnormal findings. His blood pressure is 126/80 mm Hg. Hislipid profile includes a total cholesterol level of 165 mg/dL,high-density lipoprotein cholesterol level of 60 mg/dL,triglyceride level of 125 mg/dL, and low-density lipoproteincholesterol level of 80 mg/dL. His 10-year ASCVD risk isestimated at 6.1%. After a discussion with his preventivecardiologist, the patient remains uncertain whether hewants to take a statin and opts for additional testing.Computed tomography is performed to detect coronarycalcium and reveals no evidence of calcified plaque. Thepatient, in consultation with his preventive cardiologist,decides to withhold statin treatment and to continue hisregular exercise program and a low saturated fat diet.FIGURE 2. Case studies.independent of conventional risk factors, so the10-year risk could be multiplied by 2. The validity of this approach is uncertain because itdoes not take into account the prevalence ofthe abnormal risk marker.47 Finally, whetherto downgrade a patient’s risk estimated fromthe ASCVD calculator on the basis of resultsfrom adjunctive testing is another area ofcontroversy.Mayo Clin Proc. n XXX al PopulationsThere is insufficient evidence to guide management of certain patient populations who may beat increased risk of adverse cardiovascular outcomes. The additive risk of these conditionsindependent of conventional risk factors is uncertain. These conditions include systemic inflammatory diseases,48 a history of gestationaldiabetes or hypertensive disorders of pregnancyinluding preeclampsia,49 chronic kidney disease,50 and human immunodeficiency virusinfection.51 Imaging studies to assess subclinical disease burden may be useful in these settings to better define ASCVD risk.USE OF ADJUNCTIVE MEASURES TOREFINE ESTIMATES OF ASCVD RISKWe suggest the following adaptation of theACC/AHA guidelines for the use of adjunctivetests to refine ASCVD risk estimates.Family HistoryA family history of early-onset ASCVD (definedas occurrence of an ASCVD event in a firstdegree male relative before age 55 years or in afirst-degree female relative before age 65 years)should be sought from every patient who presents for cardiovascular screening.30,52-54 Werecommend obtaining a family history concurrent with estimating risk using the ASCVDcalculator, rather than later as an adjunctivemeasure. The presence of a family history ofASCVD is likely to be an important factor inshared decision making regarding lifestylechanges and statin use and also provides an opportunity to detect additional individuals in afamily who may be at risk. We recognize theneed for additional studies to estimate moreprecisely the relative risk that results from thepresence of a family history of ASCVD. In theabsence of robust relative risk estimates for thepresence of family history, clinical judgmentcould be utilized in deciding how much to“adjust” the risk estimated from the ASCVDequation.Adjunctive TestingWe agree that CAC scoring can be used selectively to aid decision making in situati
ª 2014 Mayo Foundation for Medical Education and Research nMayo Clin Proc. 2014;nn( ):1-13 A ssessment of cardiovascular risk is a necessary first step to target therapy toward patients most likely to benefit. It has become evident that baseline atheroscle-rotic cardiovascular disease (