Transcription
Self-help and daily livingPain and arthritisPain andarthritisThis booklet provides informationand answers to your questionsabout this condition.Arthritis Research UK produceand print our booklets entirelyfrom charitable donations.
Pain and arthritis information bookletWhat is pain?Many people with arthritis livewith pain for years. This bookletexplains what pain is and how thebrain senses pain. It also describessome common conditions thatcan cause pain in and aroundjoints, as well as the differentmethods for helping people tocontrol long-term (chronic) pain.At the back of this booklet you’ll find a brief glossary ofmedical words – we’ve underlined these when they’refirst used.www.arthritisresearchuk.orgPage 2 of 28
Pain and arthritis information bookletArthritis Research UKWhat’s inside?2 Pain and arthritis at a glance4 What is pain?4 Pain and the brain5 Short-lived pain6 Arthritis, joint and muscle pain– Osteoarthritis– Rheumatoid arthritis– Neck and back pain– Chronic pain syndromes10 What can I do about my pain?– Drugs– Painkilling (analgesic) drugs– Non-steroidal anti-inflammatorydrugs (NSAIDs and coxibs)– Corticosteroid drugs– Drugs for nerve pain and chronicpain syndromes– Nerve blocks and other injectiontechniques for pain16 Other pain relief treatmentsand therapies– Transcutaneous electrical nervestimulation (TENS)– Acupuncture– Psychological techniques– Relaxation techniques andsleep patterns18 Self-help and daily living19 What should I do if my painis severe?19 Research and newdevelopments20 Glossary22 Where can I find out more?24 We’re here to help
Pain and arthritis information bookletAt a glancePain and arthritisWhat is pain?Put simply, pain is a protectivemechanism that alerts the brain whendamage has occurred. But pain isn’t justa sensation, it has emotional effects too– making us feel upset or distressed.Pain may continue when the damageseems to have gone. This is a featureof some chronic pain syndromes.What causes it?Pain may be caused by: a physical injury or damage toThere are now manyapproaches availableto help manage painincluding drugs,physical treatmentsand coping strategies. enjoyable activities, which can takeyour mind off the pain and make itmore manageable unhappy feelings, anxieties ordepression, which can worsen pain prescription drugs (that have a directeffect on the brain, chemically reducingthe impact of pain).body tissues c hemicals produced by inflammation damage to the nerves or nerve endings.The most common causes of chronic painin joints or muscles are: osteoarthritisr heumatoid arthritis neck and back pain chronic pain syndromes. hat can affect the severityWof my pain?The pain severity can be affectedby a number of factors including: how much you concentrate on the painHow can I manage my pain?There are a number of approachesavailable to help you manage your pain:Drugs: painkilling drugs ranging fromparacetamol to codeine and up tostronger options like oxycodone, slowrelease morphine or patches containingfentanyl or buprenorphine non-steroidal anti-inflammatorydrugs (NSAIDs) and coxibs, whichare painkillers as well as havingan anti-inflammatory action corticosteroids, often called steroids forshort, given as tablets or by injectionPage 4 of 28
Pain and arthritis information booklet drugs for nerve pain and chronicpain syndromes t ricyclic antidepressants, for exampleamitriptyline or dosulepin, improvesleep and help the brain to controlsensations from upper body and limbs g abapentin, carbamazepine andpregabalin can help control sometypes of pain, especially if causedby nerve damage.Other pain relief treatmentsand therapies: a heating pad or hot-water bottle t echnologies such as ultrasound,laser or interferential treatment exercise programmes.How can I help myself?Unfortunately, for some people pain islong-lasting, doesn’t respond fully todrugs or physical treatments, and can’tbe cured by surgery. In this case it’s worththinking about lifestyle changes, such as: learning to rest sensibly (but not givingup all exercise) an ice pack or cold-water compress massage (with or without creams avoiding certain activities asking for help using gadgets and home adaptations. rest and good-quality sleep transcutaneous electricalA doctor, physiotherapist, social workeror occupational therapist can offer experthelp and advice with these changes.that create a sense of warmth)nerve stimulation (TENS) acupuncture psychological techniques for examplegroup discussions and cognitivebehavioural therapy relaxation techniques for examplerelaxation tapes, yoga, the Alexandertechnique and hypnosis physiotherapy, osteopathy andchiropractic use techniques including: hat should I do if my painWis severe?For a small minority of people pain canbe severe and disabling. This can resultin a vicious circle of pain, anxiety anddepression, and becoming physicallyunfit. People affected in this way shouldbe referred to a pain management clinicto learn new ways to cope with pain. massage, manipulation and stretchingPage 5 of 28
Pain and arthritis information bookletWhat is pain?Although everyone understands what wemean by the word pain, it’s still difficult todefine. Put simply, it’s usually a protectivemechanism that alerts the brain whendamage has occurred. Pain isn’t just asensation, it has emotional effects too– making us feel upset or distressed(see Figure 1).Sometimes it’s difficult to explain theexact cause of long-term (chronic) painand this can also make it difficult totreat effectively. This type of chronicpain can sometimes be felt all over thebody (chronic widespread pain), as infibromyalgia, for example.See Arthritis Research UK bookletFibromyalgia.Figure 1 The causes of painPain may be caused by: hysical injury or damage to bodyPtissues, for example damage to thejoint cartilage in osteoarthritis. hemicals produced as a resultCof inflammation, for example inrheumatoid arthritis. Our bodies havespecialised nerve endings that detecttemperature and chemical changes ormechanical stresses. These chemicalsactivate specialised nerve endingswhich send pain signals via the spinalcord to the brain.Damage to nerves or nerve endings.This causes the nerves to sendpain signals to the spinal cordspontaneously without needing aspecific stimulus, or in response tosomething that wouldn’t normallyhurt, such as gentle stroking of theskin. This sometimes happens incomplex regional pain syndrome(reflex sympathetic dystrophy) andperipheral neuropathy (a commonproblem in diabetes).Such conditions are a challenge to boththe patient and the doctor. The factthat it’s hard to explain where thepain is coming from doesn’t mean thepain is imaginary or psychological.However, psychological factors can affectthe way in which the brain senses physicalpain (see section ‘Other pain relieftreatments and therapies’).Pain and the brainThe spinal cord has special ‘gate’mechanisms that interfere with painmessages coming from the nerves, andmay block or deflect them so the painsignal that reaches the brain is slightlyaltered. These ‘gates’ can either reduce orincrease the strength of the pain signal.Some treatments for pain are aimedat closing these ‘gates’ to reducethe sensation of pain, for example,transcutaneous electrical nervestimulation (TENS).Page 6 of 28
Pain and arthritis information bookletOnce the pain signal gets through thespinal ‘gate’, it’s further changed by evenmore complex systems in the brain.The pain message can be affected by anumber of factors including: h ow much you concentrate on the pain enjoyable activities, which can takeyour mind off the pain and make itmore manageable unhappy feelings, anxieties ordepression, which can worsen pain drugs that have a direct effect onthe brain, chemically reducing theimpact of pain.Short-lived painMost people have had first-handexperience of pain which is easilyunderstandable, is manageable,and doesn’t last very long. Gout is aform of arthritis that causes short-livedattacks of pain, lasting only a few days.See Arthritis Research UK bookletGout.Learning to cope with short-lived painis an important part of growing up.The experiences of pain we have aschildren, and the way we are taught tocope with it, may strongly influence howwe cope with pain in adult life.
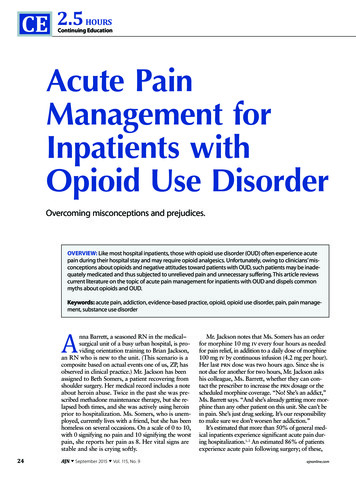
Pain and arthritis information bookletArthritis, joint andmuscle painThis section describes some of the mostcommon causes of chronic pain in jointsor muscles and the ways in which painfrom these conditions can be treated(see Figure 2).OsteoarthritisIn osteoarthritis, the cartilage thatcovers the surface of the bones in thejoints becomes roughened and thin.This is associated with damage to theunderlying bone, causing pain, stiffnessand deformity. Sometimes there may beswelling and a sudden increase in pain.When osteoarthritis affects the hands,the pain will often settle after a few weeksor months, although some deformity andstiffness may remain. In other joints, suchas the hips, knees or spine, the pain maylast a long time and, in some cases, it mayseverely limit normal activities.See Arthritis Research UK bookletsOsteoarthritis; Osteoarthritis of the knee.Figure 2 The most common causes of chronic pain in joints and musclesOsteoarthritisChronic painsyndromes, such ascomplex regionalpain syndromeMost common causesof chronic pain injoints and musclesRheumatoidarthritisNeck and backproblems,such as sciatica orspondylosisPage 8 of 28
Pain and arthritis information bookletPossible pain relief approachesfor osteoarthritis: pain-relieving (analgesic) and antiinflammatory drugsPeople withrheumatoid arthritisare usually treatedwith drugs thatcontrol the diseaseand reduce the riskof joint damage. N SAID gels and rubefacients physiotherapy, exercise andlosing weight orthotic treatments such as insolesand splints a steroid injection into the joint whenthere’s a lot of swelling or fluid.I n severe osteoarthritis, effective relieffrom pain may only be achieved bysurgery. The small but important risks ofsurgery have to be weighed against theseverity of the problem and the likelylong-term benefit of surgery.See Arthritis Research UK bookletsKeep moving; Physiotherapy andarthritis. Also see our range ofdrug leaflets and surgery booklets.Rheumatoid arthritisRheumatoid arthritis is a form ofinflammatory arthritis in which theaffected joints become warm, swollenand painful. The pain may be persistentand is sometimes difficult to control, butthis isn’t true for everyone. Many peopleare greatly helped by drugs, short periodsof rest and physiotherapy.For some, the arthritis goes away after afew months or years. For others it causeslonger-term problems. People withrheumatoid arthritis are usually treatedwith drugs that control the disease andreduce the risk of joint damage. These aresometimes called disease-modifying antirheumatic drugs (DMARDs). They’re notpainkillers or anti-inflammatory drugs, butbecause they control the disease the painshould be reduced.For about 1 in 10 people with rheumatoidarthritis the chronic joint pain neverdisappears completely. This pain isgenerally caused either by uncontrolledinflammation in and around the jointsdespite the use of DMARDs, or by thedamage and instability which result fromthe inflammation. Most people withrheumatoid arthritis will need painrelieving drugs and drugs that reduceinflammation in addition to DMARDs.It’s also important to balance rest andexercise sensibly – a physiotherapistcan advise on appropriate exercises.Surgery may sometimes be needed forparticularly painful or deformed joints.See Arthritis Research UK bookletRheumatoid arthritis.Page 9 of 28
Pain and arthritis information bookletNeck and back painMost people experience short spellsof neck pain or back pain that improvewithout specific treatment.If the pain keeps returning, there arepreventative approaches that can helpdeal with the problem. These include: exercises to strengthen the muscles special care with posture or yourworking position extra care during activities that involvebending, twisting or stretching being careful when liftingheavy objects.Neck pain after a whiplash injury canbe difficult to control in some people,but most improve with simple measuresafter a few weeks or months.For some people back pain spreadingdown one or both legs (sciatica) is causedby pressure on nerve roots in the spine.This pain may be relieved by x-ray guidedspinal injections, such as epidurals ornerve root blocks. These are specialistprocedures which are usually carriedout in a day-case operating theatre.A small number of people have backor neck pain that fails to improve andbecomes chronic. It’s often difficult tounderstand why this has happened.This pain is disabling and the challengeis not to let it dominate your life. A painmanagement programme – includingeducation, exercise and coping strategies– may help.Spinal surgery can be highly successfulbut isn’t usually needed and should onlybe undertaken after careful considerationof the alternatives. Most people with backand neck pain won’t benefit from surgery.See Arthritis Research UK bookletsBack pain; Neck pain.Chronic pain syndromesChronic headaches, facial pains andchronic upper limb pain syndrome– previously called repetitive straininjury (RSI) – are examples of chronicpain syndromes. It’s often difficult toidentify exactly what causes the pain,but it’s affected by factors such as theway the sufferer walks, stands and usestheir muscles.As there’s no cure or simple explanationfor many of these chronic pain syndromes,people in chronic pain may see a largenumber of specialists and sometimesreceive different, or even contradictory,explanations and a wide variety ofsuggested treatments. Because theproblem seems to worsen without anycure being available, the person in painmay feel let down by modern medicine.Because it’s so difficult to explain whatcauses chronic pain, people often findit hard to help family, friends, workcolleagues and healthcare professionalsto understand how they’re feeling.Those people, in turn, may then findit difficult to deal with the problem.Page 10 of 28
It’s important tobalance rest andexercise sensibly– a physiotherapistcan advise onappropriateexercises.
Pain and arthritis information bookletHowever, there are pain managementclinics, specialising in the care of chronicpain. Your GP should be able to refer youfor advice and help.In many cases chronic pain leads tochanges in the way people behave –which may then make the pain worse.For example, a person with chronicpain in the right leg may start to standor walk leaning heavily to the left side,which may eventually lead to pain inthe left leg too. When people havechronic pain that prevents them fromdoing things that they need or wantto do, this may often affect their moodand feelings, leading to frustration,anxiety and depression. Just likechanges in the way people walk orstand, these changes in mood canmake the pain feel worse too.In complex regional pain syndrome(reflex sympathetic dystrophy) pain isconfined to a particular region of thebody (for example one arm or one leg)and often has a burning quality. It mayfollow a minor injury, an operationor a stroke or there may be no clearunderlying cause. It’s thought that thecommunication pathways between theaffected limb and the brain becomedisrupted, so the pain is more intense or,if it follows an injury, persists for longerthan expected.Treatment for complex regional painsyndrome may include standardpainkillers or stronger morphine-likepainkillers. However, some people willneed neuromodulatory drugs (forexample gabapentin, pregabalin) whichreduce the pain signals from the nerves tothe brain, or a sympathetic block – aninjection that suppresses the sympatheticnervous system. Rehabilitation is animportant aspect of the treatment andmay include specialist physiotherapy,occupational therapy and psychology.Most people with complex regional painsyndrome will benefit from touching ormoving the affected limb, in spite of pain.See Arthritis Research UK bookletComplex regional pain syndrome (CRPS).What can I do aboutmy pain?There are now more approachesavailable than ever before to helpmanage pain. Drugs, physical treatmentsand coping strategies can all play a part.One of the keys to handling pain is tounderstand what’s happening.DrugsBefore 1900, aspirin and simplederivatives of opium (similar to morphine)were the only pain-relieving drugsavailable, but now there are many more.Although it’s important to consider thebalance of benefit and the risk ofpossible side-effects of drug treatments,in general the risks are far outweighedby the benefits.Page 12 of 28
Pain and arthritis information bookletThere are painmanagement clinics,specialising in the careof people with chronicpain. Your GP shouldbe able to refer you foradvice and help.Because it’s so difficultto explain what causeschronic pain, people oftenfind it hard to help family,friends, work colleaguesand healthcare professionalsto understand howthey’re feeling.Page 13 of 28
Pain and arthritis information bookletDrugs may be available under severaldifferent names. Each drug has anapproved (or generic) name butmanufacturers often give their ownbrand or trade name to the drug aswell. For example, Nurofen and Panadolare brand names for ibuprofen andparacetamol respectively, which are theapproved names. The approved nameshould always be on the pharmacist’slabel even if a brand name appears onthe packaging, but check with yourdoctor, nurse or pharmacist if you’re inany doubt. We’ll use the approved namesin the sections that follow. Tramadol, oxycodone, slow-releasePainkilling (analgesic) drugsAnalgesics are drugs that act specificallyagainst pain and are helpful for mosttypes of pain: Paracetamol is an example of asimple analgesic.Non-steroidal anti-inflammatorydrugs (NSAIDs and coxibs)NSAIDs combine pain-relieving effectswith an additional action that reducesinflammation. As inflammation is themain cause of pain in many conditions –including most forms of arthritis – thesedrugs can be doubly effective againstchronically painful conditions. More complex analgesics are relatedchemically to morphine but are muchless likely than morphine to causeproblems such as addiction. However,other side-effects such as constipationand drowsiness still occur. Codeineis an example. They’re often usedmore effectively in combination withparacetamol as compound tablets,for example: c o-codamol (paracetamoland codeine) co-dydramol (paracetamoland dihydrocodeine).morphine or patches containingfentanyl or buprenorphine are strongerdrugs which may be used for severepain but are used with more caution.All of these drugs can be seen as partof the morphine family, as can codeineand dihydrocodeine. Opioid analgesicscan cause constipation and may causedrowsiness, especially if taken withalcohol.See Arthritis Research UKdrug leaflet Painkillers.They can be used in combination withthe simple or compound analgesicsmentioned above, and can behelpful even when there isn’t a greatdeal of inflammation – for examplein osteoarthritis: Aspirin and ibuprofen are probablythe best-known NSAID tablets andare widely available over the counterwithout a prescription. Diclofenac, naproxen and indometacinare other commonly used NSAIDtablets. These are available witha doctor’s prescription.Page 15 of 28
Pain and arthritis information bookletAnyone whohas had severeindigestion orpeptic ulcers inthe past shouldusually avoidusing NSAIDs. Some NSAIDs (for example ibuprofen,diclofenac) are also available as gelswhich are applied to the skin aroundpainful joints. These may sometimesproduce local skin irritation. A newer type of NSAID commonlycalled coxibs (COX-2-specific NSAIDs),such as celecoxib or etoricoxib,are designed to control pain andinflammation but are less likely tocause indigestion and stomach ulcerssometimes associated withthe older NSAIDs.Like all drugs, NSAIDs can sometimes haveside-effects, but your doctor will takeprecautions to reduce the risk of these– for example, by prescribing the lowesteffective dose for the shortest possibleperiod of time.NSAIDs can cause digestive problems(stomach upsets, indigestion, or damageto the lining of the stomach) so in mostcases they’ll be prescribed along with adrug called a proton pump inhibitor (PPI),which will help to protect the stomach.NSAIDs also carry a slightly increased riskof heart attack or stroke. Although theincreased risk is small, your doctor willbe cautious about prescribing NSAIDs ifthere are other factors that may increaseyour overall risk – for example, if you’vepreviously had angina or a heart attackor if you smoke, or have circulationproblems, high blood pressure, highcholesterol or diabetes.See Arthritis Research UKdrug leaflet Non-steroidal antiinflammatory drugs.Corticosteroid drugsCorticosteroid drugs (steroids) may begiven either as tablets or by injection.They’re not painkillers, but by reducinginflammation they also reduce the pain.Prednisolone is the most commonlyprescribed steroid tablet forinflammatory arthritis. In certainconditions steroid tablets are prescribedbecause nothing else works, such as inpolymyalgia rheumatica.See Arthritis Research UK bookletPolymyalgia rheumatica (PMR).Steroids can also be given by injection– either into the joint itself or into softtissues near the joint. Steroid injectionsare usually very effective in relieving painand the benefit can last from a few weeksto several months. Sometimes the painmay flare up for a day or so just after theinjection before settling down.Page 16 of 28
Pain and arthritis information bookletSee Arthritis Research UKdrug leaflets Local steroid injections;Steroid tablets.Side-effects usually develop only whensteroid tablets are used for more thana few months, and are more likely to occurwith larger doses. The most commonside-effects are increased appetiteand weight gain, muscle weakness,and anxiety or sleeplessness. They mayalso cause thin, slow-to-heal skin or thin,fragile bones (osteoporosis). However, therisk of developing osteoporosis can bereduced by medication.See Arthritis Research UKdrug leaflet Drugs for osteoporosis.Drugs for nerve pain and chronicpain syndromes Tricyclic antidepressants (mostcommonly amitriptyline or dosulepin)are prescribed to be taken at night forpeople who have chronic widespreadpain, especially fibromyalgia wheredisturbed or unrefreshing sleep isthought to contribute to the ongoingpain. These drugs act partly by improvingsleep and partly by helping the brainto control sensations coming from theupper body and limbs. At the low dosesused for chronic pain they aren’t trulyanti-depressant. Side-effects includedrowsiness in the morning and a drymouth, although these aren’t usually aproblem if the dose is increased slowly. abapentin, carbamazepine andGpregabalin are members of a groupof neuromodulatory drugs (drugs thatact on the nervous system) often usedto treat epilepsy. However, they can alsobe useful in controlling some types ofpain, particularly where the pain is dueto nerve damage.Nerve blocks and other injectiontechniques for painIncreasingly, pain specialists are usinginjections to block pain by a directaction on a nerve or on the spinalnerve root when other treatments fail.These injections usually combine alocal anaesthetic with a corticosteroid.They’re not suitable for all types ofpain, but they’re sometimes helpful forosteoarthritis of the small facet jointsbetween the bones of the spine or forcompression of nerves in the lower spine.Increasingly, painspecialists areusing injectionsto block pain bya direct action ona nerve or on thespinal nerve root.Page 17 of 28
Pain and arthritis information bookletLearning to restsensibly, avoidingcertain activities,asking for help, andusing gadgets andhome adaptationsare all importantways of adjustingand learningto cope.The exact site for the injection can usuallyonly be decided after special scans,such as magnetic resonance imaging(MRI) or computerised tomography (CT).The specialist can then place theneedle accurately by following an x-rayimage, which is displayed on a screen.These treatments are for symptomcontrol and aren’t cures.arthritis or back pain. They don’t cure theproblem, but they are safe and soothing.Physiotherapists, osteopaths andchiropractors may use a variety ofdifferent manual techniques, includingmassage, manipulation and stretching,to relieve pain and to help return themuscles and joints to normal. They mayalso use technologies such as ultrasound,laser or interferential treatment.Exercise programmes, initially supervisedby a physiotherapist, may help tocontrol your pain. They help to relaxand strengthen the muscles and mayalso improve general fitness. Pilates orcore stability exercises are increasinglyrecommended for people with backpain. Exercise at a time when you’re notfeeling too stiff and take some painkillersbeforehand if you need to. Take time torelax and rest afterwards.Simple measures that can help to relievejoint or muscle pain include: a heated wheat or rice pad or ahot-water bottleIt’s important to go to a qualifiedpractitioner, preferably with the adviceand guidance of your doctor. If there’sno improvement after a few weeks oftreatment, further investigations maybe needed. It’s better to exercise littleand often rather than a lot occasionally.Find a form of exercise that you enjoy soyou’re more likely to continue with it. a n ice pack or a cold-water compress massage (with or without creamsTranscutaneous electrical nervestimulation (TENS)Other pain relieftreatments and therapiesthat create a sense of warmth, calledrubefacients) adequate r est time.These techniques are often helpful afteran injury and for sudden flare-ups ofThis is a technique that uses small pulsesof electricity to produce a tinglingsensation. It aims to disrupt pain signalsby reducing the sensitivity of the nerveendings in the spinal cord. It doesn’t helpeverybody, but some people find it veryPage 18 of 28
Pain and arthritis information bookleteffective, especially when the pain is dueto nerve damage. Some people becomeallergic to the jelly used to apply thepads, but otherwise TENS has few sideeffects. A physiotherapist can advise youon the correct position of the pads, thefrequency and strength of the pulses,and how long the treatment should last.AcupunctureAcupuncture is used by doctors andother practitioners for many purposesincluding pain relief – often with goodeffect. Very fine needles are inserted intospecific points in the body. It’s thoughtto work by diverting or changing thepainful sensations that are sent to thebrain and by stimulating the body’s ownpain-relieving hormones (endorphinsand encephalins).Psychological techniquesPsychologists are specialists whooften work as part of the team in painmanagement clinics. They help peopleto think differently about their painand change their behaviour as a result.Although some people are suspiciousof this approach at first, it has proved tobe very successful in helping people tomanage their symptoms. Pain is never apurely physical phenomenon, and whenthe pain is chronic, or its cause is difficultto determine, the psychological and socialeffects need to be specifically addressed.
Pain and arthritis information bookletRelaxation techniques andsleep patternsRelaxation techniques are helpful inmany conditions. They work by: relaxing the tense and painful muscles relieving the anxiety that makes painmore difficult to bear.Relaxation tapes, yoga and hypnosiscan sometimes be helpful. Specialmethods like the Alexander technique(which teaches awareness of postureand relaxation to reduce muscle tension)may also help. They’re often used by painmanagement clinics. It’s worth askingyour doctor about these techniques.It’s recognised that disturbed orunrefreshing sleep increases thesymptoms of pain – especially musclepain. If you wake still feeling tired or wakefrequently during the night, a doctor orphysiotherapist may be able to adviseyou about improving this.See Arthritis Research UK bookletsFatigue and arthritis; Sleep and arthritis.Self-help and daily livingUnfortunately, for some people pain islong-lasting, doesn’t respond fully todrugs or physical treatments, and can’tbe cured by surgery. In this case it’sworth thinking about lifestyle changes.Learning to rest sensibly, avoidingcertain activities, asking for help,and using gadgets and home adaptationsare all important ways of adjusting andlearning to cope. A doctor, social worker,physiotherapist or occupational therapistcan offer expert help and advice withthese changes.
Pain and arthritis information bookletArthritis Research UKWhat should I do if mypain is severe?Research and newdevelopmentsFor a small minority of people pain canbe severe and disabling. The pain oftenmeans you have to rest more, or can onlywalk or move awkwardly. This can resultin a vicious circle of pain, anxiety anddepression, and becoming physicallyunfit. It can be difficult to pluck up thecourage to do exercises despite the pain,to find other things to concentrate on andto refocus your thoughts away from thepain. People affected in this way shouldbe referred to a pain management clinic.Learning new ways to cope with pain canhelp. It can be helpful in certain situationsto focus more on improving your abilityto function rather than trying to reducepain. This can sometimes be achieved bydeveloping strategies to help with fearof movement. With help from family andfriends, as well as from specialists, you canstill have a fulfilling life.Alongside the University of Nottinghamand local NHS Trusts, Arthritis ResearchUK are proud to support the world’sfirst national centre for research intounderstanding the mechanismsof pain in arthritis.See Arthritis Research UK guideLiving with long-term pain: a gui
See Arthritis Research UK booklets Keep moving; Physiotherapy and arthritis. Also see our range of drug leaflets and surgery booklets. Rheumatoid arthritis Rheumatoid arthritis is a form of inflammatory arthritis in which the affected joints become warm, swollen and painful. The pain may