Transcription
PSY C15.qxd 1/2/05 3:43 pm Page 314AbnormalPsychologyCHAPTER OUTLINELEARNING OBJECTIVESINTRODUCTIONWHAT DOES ‘ABNORMAL’ MEAN?WHAT CAUSES ABNORMAL BEHAVIOUR?Biology and geneticsPsychodynamics and the parent–child relationshipAttachment and securityLearned behaviourDistorted thinkingIntegrative modelsDISORDERS – SYMPTOMS AND CAUSESSchizophrenia – a living nightmareMood disorders – depressionAnxiety disorders – when fear takes overEating disorders – bulimia and anorexiaSubstance use disorders – abuse and dependencePersonality disorders – a way of beingFINAL THOUGHTSSUMMARYREVISION QUESTIONSFURTHER READING15
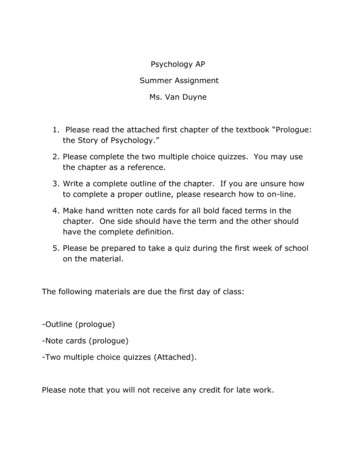
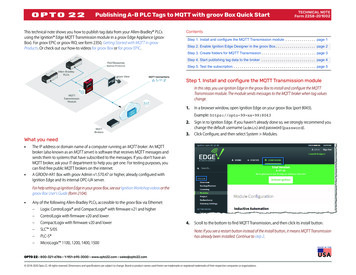
PSY C15.qxd 1/2/05 3:43 pm Page 315Learning ObjectivesBy the end of this chapter you should appreciate that:nabnormal psychology (or psychopathology) deals with sets of behaviours or symptoms that produce a functionalimpairment in people’s lives;npsychological disorders (e.g. schizophrenia) have been documented across time and culture;nthroughout history, the causes of abnormal behaviour have been construed from a number of differentperspectives;nbiological/genetic models focus on brain defects, biochemical imbalances and genetic predispositions as causesof psychopathology;nFreudian, contemporary psychodynamic and attachment models focus on the effects of early parent–childexperiences;nbehavioural models focus on the learning experiences that result in psychopathology;ncognitive models focus on the effect of distorted thought processes;nthe diathesis–stress perspective suggests that the factors identified by each of the other models may work inaccordance with one another;nthe developmental psychopathology perspective provides a framework for understanding how psychopathologydevelops from childhood to adulthood;nthese perspectives can help us understand the numerous disorders documented in classification systems such asthe DSM-IV and the ICD-10;nthere are several major forms of psychopathology, including schizophrenia, mood disorders, substance abuse,eating disorders and personality disorders.INTRODUCTIONAbnormal psychology is the study of mental disorders (also called mental illness, psychologicaldisorders or psychopathology) – what they looklike (symptoms), why they occur (etiology), howthey are maintained, and what effect they have onpeople’s lives.Mental disorders are surprisingly common. Forexample, a study conducted by the World HealthOrganization examined the prevalence, or frequency,of mental disorders in people visiting medicaldoctors in primary care settings in 14 countries.As figure 15.1 shows, the study revealed that24 per cent of these people had diagnosablemental disorders and another 10 per cent hadsevere symptoms of mental disorders (Üstün &Sartorious, 1995).
PSY C15.qxd 1/2/05 3:43 pm Page 316316Abnormal Psychology603550% of patients3025201510Current % of population404030201000012Number of disorders3 or moreFigure 15.1Figure 15.2Rates of current mental disorder in patients presentingto primary care facilities across the world.Source: Adapted from Üstün and Sartorius (1995).Comorbidity in lifetime rates of mental disorders. Comorbidity is the occurrence of two or more disorders atthe same time. Of the 48 per cent of people reportinglifetime history of disorder in this study, over half reportedtwo or more simultaneous disorders. These data comefrom a survey in the US, but similar rates of comorbidityhave been found in countries around the world.Source: Kessler et al. (1994).Psychopathology can happen to anyone andaffects many people around them – there is noage, race or group that is immune. Furthermore,many people experience more than one disorderat the same time (see figure 15.2).WHAT DOES ‘ABNORMAL’ MEAN?Defining abnormality is deceptively difficult. When asked todescribe abnormal behaviour, people typically say that it occursinfrequently, is odd or strange, is characterized by suffering, or isdangerous. All of these are reasonable answers for some types ofabnormal behaviour, but none of them is sufficient in itself, andmaking them all necessary results in too strict a definition.One parsimonious and practical way to define abnormalbehaviour is to ask whether the behaviour causes impairment inthe person’s life. The more abehaviour gets in the way ofimpairment extent to which a behavisuccessful functioning in anour or set of behaviours gets in the wayimportant domain of lifeof successful functioning in an import(including the psychological,ant domain of the individual’s lifeinterpersonal and achievement/performance domains),the more likely it is to be considered a sign of abnormality. Whenseveral such behaviours or symptoms occur together, they mayconstitute a psychological disorder.Psychological disorders are formally defined in widely usedclassification systems, or nosologies: the International Classification of Diseases – 10th edition (ICD-10; World Health Organization, 1992) and the Diagnostic and Statistical Manual of MentalDisorders – 4th edition (DSM-IV; APA, 1994). Although they differfrom one another in format, these two systems cover the samedisorders and define them in a similar manner.The frequency and widespread suffering causedby mental disorders makes our understanding ofthem critical.Importantly, both the ICD-10 and the DSM-IV require thatthe level of impairment a person is experiencing be taken intoaccount when deciding whether they meet criteria for any mentaldisorder. For example, the DSM-IV diagnostic criteria for depression specify that: ‘The symptoms cause clinically significant distress or impairment in social, occupational, or other importantareas of functioning’ (p. 327). The ICD-10 description of depression also states: ‘The extent of ordinary social and work activitiesis often a useful general guide to the likely degree of severity ofthe episode’ (p. 121).Finally, it is important to be sensitive to how contextual factorsaffect judgements about abnormality, so as not to over- or underpathologize groups or individuals. Such factors include ethnicityand culture, gender, age and socio-political values. For example,homosexuality was once listed as a disorder in the DSM, but, associo-political values changed to become somewhat more liberaland accepting, it was deleted.WHAT CAUSES ABNORMALBEHAVIOUR?With a basis for understanding how to define abnormalbehaviour, we can focus on its causes. Abnormal behaviour isconstrued from a number of different perspectives. Each of thefollowing models tells us something about different aspects of amulti-faceted group of mental disorders.
PSY C15.qxd 1/2/05 3:43 pm Page 317317What Causes Abnormal Behaviour?BIOLOGYAND GENETICSBiological and genetic models assert that mental disorders are diseases, and symptoms of mental disorders are caused by factorssuch as brain defects (abnormalities in the structures ofbiochemical imbalance complex neurothe brain), biochemical imbaltransmitter dysregulation process involances (complex dysregulationving the various neurotransmitters inprocesses involving variousthe brainneurotransmitters) and geneticpredispositions (risk for psychopathology carried via ourgenetic predisposition likelihood ofgenetic material).showing condition or characteristicBy and large, the evidcarried by genetic materialence for brain defects andbiochemical imbalances ascauses of mental disorders is correlational, which means that,although we know that such biological problems occur amongpeople with mental disorders, we don’t know whether theyactually cause the disorder. Because the brain is a fairly malleable organ, our behaviour and experiences can also affect ourbrain functioning, suggesting that the association betweenbiology and abnormal behaviour may be reciprocal rather thanunidirectional.Genetic models of mental disorder suggest that psychopathology is inherited from parents, and there is certainly evidence forthe familial transmission ofmany disorders. For example,familial transmission genetic transmismonozygotic (identical) twinssion of disordersshould be more likely thandizygotic (fraternal) twins tohave the same disorder because they share 100 per cent of theirgenetic material, whereas dizygotic twins share only 50 per cent.For many disorders, this is exactly what research shows.But given that monozygotic twins share 100 per cent of theirgenetic material, you might expect them to have the same disorders 100 per cent of the time. But in fact they have the samedisorders only about 50 per cent of the time. These findings haveled researchers to conclude that, rather than being deterministic,genetics contributes about 50 per cent of the risk for mental illness. Such findings show that it doesn’t make sense to questionwhether mental illness is a function of nature or nurture. Insteadwe need to focus on how the two interact.PSYCHODYNAMICSAND THE PARENT–CHILDRELATIONSHIPFreud emphasized the role of the early parent–child relationshipin the development of mental illness. According to Freud, to theextent that the child did not successfully negotiate the psychosexual stages (see chapter 14), mental illness would develop.But Freud didn’t focus on what actually occurred in the parent–child relationship (e.g. whether parents were actually poor caretakers). Instead, his focus was on the unconscious internal desiresand motivations of the child (e.g. sexual and aggressive impulses)and how the child negotiated them as s/he progressed throughthe early relationship with the child’s parents. For example, ifan adult male found himself unable to deal with authority figures,this might be interpreted as unresolved aggressive impulses towards his father. Whether his father behaved as a harsh authorityfigure or not would be considered less relevant. So, according toFreud, mental illness is due to intrapsychic (i.e. within the mind)conflict. This means a person may have very little insight intothe ‘true’ causes of their symptoms, as these are thought to beoccurring at an unconscious level of processing.Many of Freud’s ideas have gone unsupported by research, buta number of them have proven to be fairly accurate. For example,there is ample evidence that people experience and process thingsat a non-conscious level (see Westen, 1998; also chapter 14) andthat early interpersonal experiences affect later outcomes. In fact,this latter hypothesis became central to contemporary psychodynamic models of abnormal behaviour.Contemporary psychodynamic models (e.g., Kohut, 1977;Kernberg, 1976; Mitchell, 1988) also suggest that the earlyparent–child relationship is the original source of mental illness,and that what goes on in the mind of the child (and the adult)is important.But these models differ from Freud’s in that they focus moreon interpersonal relationships than on intrapsychic conflict. Theselater models suggest that the early relationship between the childand the primary caregiver is crucial to the development of theself-concept, concepts of others, and the quality of relationshipsthroughout life. The idea is that this early caregiver– child relationship is internalized by children, so that they learn about themselves and others from the manner in which the caregiver treatsthem. According to this framework, the nature of this internalized relationship and its resulting impact on the sense of self andthe sense of others is what can create vulnerability to psychological problems.ATTACHMENTAND SECURITYThe attachment model of psychopathology, developed byBowlby (1969; 1973; 1980; see also chapter 9) resembles the contemporary psychodynamic models in that it also emphasizes theearly parent–child relationship and how the resulting models ofself and others guide development. But rather than being interested in people’s perceptions of their early experience, Bowlbywas interested in the actual characteristics of the relationship. Herelied on observational studies of parents and children to build histheory, rather than on retrospective reports of adults. The theorytherefore has a strong empirical foundation.Attachment theory suggests that when parental behaviour failsto make children feel safe, secure, and able to turn to and trust theparent in times of need, then children will be unable to regulatetheir emotions and needs adaptively and will develop negative,‘insecure’ views of themselves and others. This would put children at risk for developing psychological disorders. Research supports this hypothesis, as ‘insecure’ children and adults show morepsychopathology than ‘secure’ children and adults (see Dozier,Stovall & Albus, 1999; Greenberg, 1999).
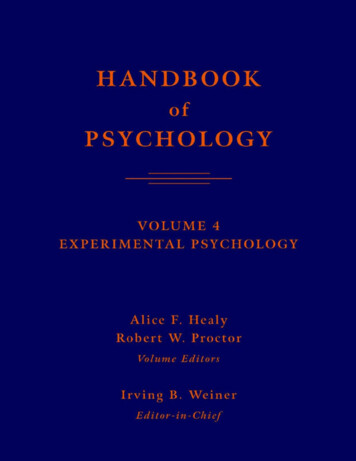
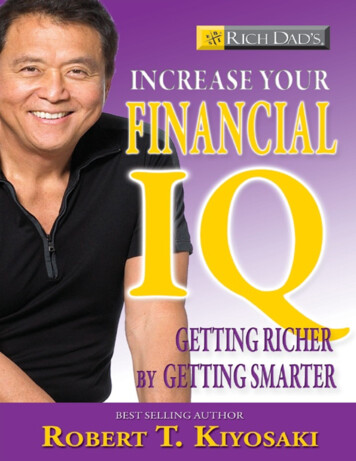
PSY C15.qxd 1/2/05 3:43 pm Page 318318Abnormal PsychologyResear ch close-up 1Reconciling the roles of genetics and theenvironment in risk for major depressionThe research issueAs you have read in this chapter, genetic and environmental models make very different assumptions about the causes ofdepression. Kendler et al. (1995) conducted a study in an effort to determine the extent to which genetic and environmentalfactors contribute to depression. In their study, Kendler and his colleagues examined two important questions: (1) dogenetic factors and stressful life events make unique contributions to risk for depression in women? and (2) do geneticfactors and stressful life events interact to create risk for depression? In particular, the researchers wondered whetherthe association between stressful life events and risk for depression would be greater among people at high genetic riskcompared to people at low genetic risk.Design and procedureTo examine these questions, Kender and colleagues studied four groups of women: (1) women with a depressed monozygotic (MZ) twin, (2) women with a depressed dizygotic (DZ) twin, (3) women with a non-depressed MZ twin, and (4) womenwith a non-depressed DZ twin. Women with a depressed MZ twin are at the highest genetic risk for depression, and womenwith a non-depressed MZ twin are at the lowest genetic risk for depression. For each woman, they assessed whether theperson in question had experienced a depressive episode in any given month over the course of approximately one year,and they recorded whether any severe life events occurred during each month over this one year time period.Results and implicationsBoth stressful life events and genetic factors made unique contributions to depression. Regardless of genetic risk, stressful life events were associated with depression, and regardless of life stress, genetic risk was associated with depression.However, the impact of stressful life events on risk for depression was greater among women at high genetic riskthan it was for women at low genetic risk (see figure 15.3).n Interestingly, the stressful life events that were found to be most strongly associated with depression were mainlyinterpersonal in nature (death of a close relative, serious marital problems, divorce/break-up, and assault), highlighting the importance of relationship factors in risk for depression.nHighProbability of onsetMZ withoutdepressionDZ withoutdepressionDZ withdepressionMZ withdepressionLowAbsentPresentStressful life eventsFigure 15.3Risk of onset of major depression as a function ofgenetic risk and stressful life events. Source:Kendler et al. (1995).The findings suggest that both genetic risk and stressful life events are important factors in understanding women’s riskfor depression. Moreover, consistent with a diathesis-stress model (see p. 319), women at high genetic risk who experience a stressful life event in the interpersonal domain of their lives are at greatest risk of all. Therefore, to understand riskfor depression among women best, we must consider both genetic factors and environmental factors.Kendler, K.S., Kessler, R.C., Walters, E.E. et al., 1995, ‘Stressful life events, genetic liability, and onset of an episode ofmajor depression in women’, American Journal of Psychiatry, 152, 833–42.
PSY C15.qxd 1/2/05 3:43 pm Page 319319What Causes Abnormal Behaviour?LEARNEDBEHAVIOURBehavioural models suggest that all behaviour, abnormalincluded, is a product of learning – mainly learning by association(see chapter 4).For example, according to the classical conditioning model oflearning (e.g. Pavlov, 1928), if a man experiences chest painswhich result in anxiety while shopping in a department store, hemay develop a fear of department stores and begin to avoid thembecause he associates them with anxiety. There is nothing inherently frightening about department stores, but this man fearsthem because of the association that he has formed with his earlier anxiety about having a possible heart attack. Here is anotherexample which instead uses the operant model of learning (e.g.Skinner, 1953): if a young normal weight woman begins to loseweight and her friends and family praise her for doing so, she maycontinue to lose weight, even if it means starving herself. Herrestricted eating behaviour will continue because she now associates a reduction in her diet with the praise and acceptance ofothers.There is a third type of learning that does not rely on personalexperiences to establish associations. In observational learning,behaviour is learned simply by watching someone else do something and observing what happens to them (Bandura, 1969). Forexample, a young boy may learn to be aggressive after watchinghis peers act aggressively.Each of these learning models was built on a solid foundationof empirical research, and there is a great deal of evidence thateach of the three learning processes plays an important role inabnormal behaviour.DISTORTEDTHINKINGCognitive models of abnormal behaviour focus on the waypeople think about themselves, others and the world (e.g. Becket al., 1979). Distorted cognitive processes – such as selectivelyattending to some information and ignoring other information,exaggerating negative feelings, expecting the worst, or makinginaccurate attributions about events (see chapters 14 and 17) –have been shown to play an important role in various types ofpsychological disorders.For example, suppose a woman has a bad day at work. If shesays to herself, ‘Oh well, tomorrow will be better’, she will probably feel fine. But if she says to herself, ‘Oh, I’m just a horribleperson with no future’ (i.e. if she exaggerates her negative feelings), she may become depressed. Or suppose a young man losesat a game of cards. If he thinks, ‘I sure had bad luck with the cardstoday’, he will feel fine. But if he thinks, ‘My rotten friends purposely cheated me!’ he may become hostile and aggressive.single model can provide a full explanation of their onset andcourse over time. Instead, each model can help us to understanda different aspect of each disorder. This is where integrativemodels are useful.You may have noticed that only some of the models aboveexplicitly focus on childhood factors that may contribute to thedevelopment of abnormal behaviour, whereas the others onlydo so at an implicit level. For example, behavioural modelssuggest that abnormal behaviour is the product of ‘earlier’ learning experiences, but theydon’t elaborate on exactlydevelopmental psychopathology awhat those experiences are.perspective suggesting that risk forBy contrast, developmentalpsychopathology depends on success atpsychopathology provides anegotiating and mastering importantmore rigorous frameworkdevelopmental tasksfor understanding how psychopathology develops fromchildhood to adulthood. It isdiathesis–stress model suggests thatalso likely that mental illnesssome people possess an enduringresults only when particularvulnerability factor (diathesis), which,combinations of factors arewhen coupled with a proximal stressor,present. This notion is at theresults in psychological symptomsheart of the diathesis–stressmodel.The diathesis–stress modelThe diathesis–stress model of mental illness (figure 15.4) suggeststhat some people possess an enduring vulnerability factor (a diathesis) which, when coupled with a proximal (recent) stressor, resultsin psychological disorder. Neither the diathesis nor the stressoralone is enough to lead to symptoms – both must be present.Diatheses and stressors can be defined broadly. For example, agenetic or biological predisposition to mental illness might be thediathesis, and a troubled parent–child relationship could be thestressor; or a dysfunctional pattern of thinking about the worldcan be the diathesis, and a major life event the NoDisorder?NoDisorder?NoStress?Figure 15.4INTEGRATIVEMODELSThe models of abnormal behaviour described above are quitedifferent from one another, and each is more or less well suitedto particular disorders. As most disorders are quite complex, noThe diathesis–stress model of psychopathology. According tothis model, psychopathology is most likely to result when aperson with a diathesis (vulnerability) experiences a stressor.This model helps us to understand why only some peoplewith vulnerabilities, such as a genetic predisposition, developpsychopathology.
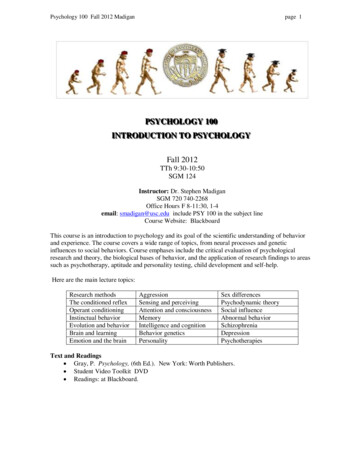
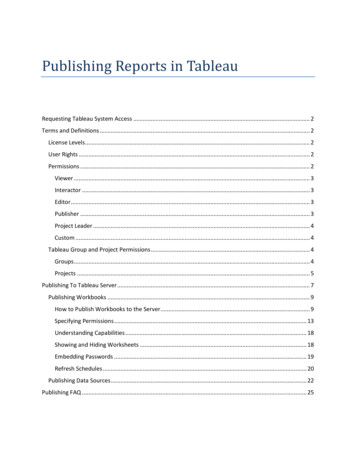
PSY C15.qxd 1/2/05 3:43 pm Page 320320Abnormal PsychologyFor each disorder we will look at its symptoms and the course ittakes. Then we will consider its causes, both biological/geneticand psychosocial, and the factors that affect its course. Prevalencerates (i.e. the cross-sectional proportion of occurrences of thedisorder in the population) for various disorders are shown infigure 15.5.A LIVING NIGHTMAREImages of schizophrenia are easy to conjure – a dishevelled person,alone, talking to himself or yelling at someone else that only heseems to see. This is a frightening image, for the symptoms it portrays are extremely odd and disconcerting. Indeed, schizophreniacan be a frightening disorder to deal with, not only for those involvedwith schizophrenic people, but for the sufferers themselves.Schizophrenia is a severe mental disorder, experienced by manysufferers as a living nightmare, a fact highlighted by the high rateof suicide among schizophrenics (Caldwell & Gottesman, 1992;see table 15.1).As you read this section, try to imagine what it might feel liketo experience some of the things schizophrenic people experience. For example, many schizophrenic people hear voices. Haveyou ever heard someone call your name, only to find there was% of population10isordels Oiv e brsdi esso srd iv eer sa0Figure 15.5Lifetime prevalence rates for psychological disorders. Theserates are from studies conducted in the US (Kessler et al.,1994), but cross-national studies indicate similar rates of disorders in other countries such as Switzerland, Germany andPuerto Rico. Source: Kessler et al. (1994).Table 15.1 Suicide: a serious mental health and public healthproblemFacts about suicidennnnSCHIZOPHRENIA –155nDISORDERS – SYMPTOMS AND CAUSES20EatAccording to this model, psychopathology is best understoodusing a lifespan development approach. It considers how thenegotiation and attainment of earlier developmental tasks affectspeople’s capacities to manage later tasks (e.g. Cicchetti, Rogosch& Toth, 1994).In other words, people may travel down one of many paths;their success or failure at various junctures along the way determines the subsequent path that they follow. So earlier deficits infunctioning may leave us unprepared to successfully negotiatesubsequent related situations, putting us at even greater risk forpsychopathology.For example, a young girl who is harshly and chronicallycriticized by her parents may develop low self-esteem and theexpectation that people will not like her, which puts her at risk ofbecoming depressed. She may then have difficulty making friendsin school because she is afraid of rejection. She may feel lonelyand undesirable, her withdrawal leading to actual rejection by herpeers, continuing her risk for depression. But if this young girl hasa teacher who treats her with warmth and care and helps her learnhow to make friends, her risk for depression might be reduced.This is because she is acquiring important skills that have thepotential to change the course of her subsequent development.25hiDevelopmental psychopathology30ScAs you read through the following sections on the various disorders, you might want to consider how a diathesis–stress processcould describe how each comes about.Risk factors for suicideSuicide occurs across the world,but rates vary by cultureSelf-inflicted injuries, includingsuicide, were the 12th leadingcause of death in the world in1998In all cultures, men are morelikely than women are tocomplete suicideRates of suicide in children andadolescents are on the risePeople with mental disorders,especially depression, substanceuse disorders, schizophrenia,and borderline personalitydisorder, are at high risk forsuicidennnnnnnnnnnnPast history of attemptedsuicideTalking about committingsuicideA clear plan to commitsuicideAvailable means (e.g.firearms, drugs)DepressionSubstance abuseHopelessnessImpulsivityStressful life eventsLack of social supportSaying goodbye to peopleGiving away personal itemsno one there? How did that feel? Rather disconcerting, mostlikely. Now magnify your feelings about 100 times and you maystart to sense how the schizophrenic person feels.SymptomsSchizophrenia is characterized by psychosis, or a breakwith reality. People who arepsychosis a break with reality, characteristic of schizophrenia
PSY C15.qxd 1/2/05 3:43 pm Page 321321Disorders – Symptoms and Causespsychotic think and behave in ways that have little to do withreality, showing significant impairment in just about every important domain of functioning – perception, thought, language,memory, emotion and behaviour. People with schizophreniamay exhibit any of these symptoms:Perceiving things that are not there – these hallucinationsare usually auditory (e.g. hearing voices), but visual andtactile hallucinations (e.g. seeing God or the devil, or feeling that insects are crawling under your skin) also occurrelatively frequently.n Believing things that are not true – paranoid delusions areparticularly common. A schizophrenic woman may believethat the government is plotting against her or that aliensparanoid delusions elaborate setplan to kill her. Everythingof beliefs, commonly experienced bywill be interpreted in theschizophrenics, characterized by signicontext of the delusion, evenficant distrust of others and feelings ofthings that are meant to help,persecutionso medication will be seen aspoison. Delusions of grandeurare also common: a schizophrenic person may believe thathe is someone famous, such as Elvis or Jesus Christ, and mayinsist on behaving like and being treated as that person.n Using odd or bizarre language, such as idiosyncratic meanings for common words or made-up words (neologisms)that only have meaning to them. They may also go off ontangents when they speak.n Disturbances in affect – flat affect can result in a lack of facialexpressions and emotionless, monotone speech, while inappropriate affect is characterized by laughing when nothingfunny has happened, crying when nothing sad has happenedor getting angry when nothing upsetting has happened.n Behavioural disturbances in four important areas:1. odd mannerisms, such as repetitive movements orbehaviours and odd facial expressions (e.g. grimaces);2. a significant lack of motivation, called avolition;3. difficulty taking care of themselves, including basic lifeskills such as paying bills, shopping, and dressing; and4. poor social skills, being socially withdrawn, and havingdisturbed relationships with others (the nature of interpersonal relationships plays a key role in the course ofthe disorder).npositive symptoms in schizophrenia,symptoms that indicate the presence ofsomething unusual, such as hallucinations, delusions, odd speech and inappropriate affectnegative symptoms in schizophrenia,symptoms that indicate the absence ofsomething normal, such as good socialskills, appropriate affect, motivation andlife skillsThe symptoms of schizophrenia are grouped into twocategories: positive and negative symptoms. Positive symptoms indicate the presenceof something unusual (suchas hallucinations, delusions,odd speech and inappropriateaffect) and negative symptomsindicate the absence of something normal (such as goodsocial skills, appropriate affect,motivation and life skills).The course of schizophreniaSchizophrenia is a chronic disorder. Although some people havebrief episodes of schizophrenic-like behaviour (called brief reactive psychoses), most people with schizophrenia suffer fromsymptoms for their entire lives.One common course of schizophrenia is a period of negative symptoms and odd behaviour during which the person’sfunctioning slowly deteriorates (the prodromal phase), followedby a ‘first break’ – the first episode of positive symptoms. Somepeople experience an episode of positive symptoms with a fewwarning signs beforehand. The manifestation of symptomscan also take a number of different forms. For example, somepeople may be delusional but still be able to take basic careof themselves, carry on a conversation and succeed in schooland work, whereas others may be completely debilitated by thedisorder.Schizophrenia typically has its onset in late adolescence orearly adulthood. Although it can start in childhood, this is quiterare. Sufferers don’t necessarily deteriorate over time, but theydo have relapses into episodes of positive symptoms.Causes of schizophrenia and factorsaffecting its course1 Genetic and biological factors These account for our initialvulnerability to schizophrenia, although exactly how they do sois unclear.What is clear is that schizophrenia tends to be inherited. Forexample, monozygotic twins have the highest concordance ratesfor schizophrenia (Gottesman, 1991), meaning that they aremore likely to both have schizophrenia if one of them has it, compared to people who shareless ge
Learning Objectives By the end of this chapter you should appreciate that: n abnormal psychology (or psychopathology) deals with sets of behaviours or symptoms that produce a functional impairment in people’s lives; n psychological disorders (e.g. schizophrenia) have been documented across time and culture;