Transcription
Republic of the PhilippinesDepartment of HealthNATIONAL NUTRITION COUNCILPHILIPPINE PLAN OF ACTION FOR NUTRITION 2017-2022A call to urgent action for Filipinos and its leadershipExecutive Summary1.The Philippine Plan of Action for Nutrition (PPAN) 2017-2022 is an integral part ofthe Philippine Development Plan 2017-2022. It is consistent with the DuterteAdministration 10-point Economic Agenda, the Philippine Health Agenda, and thedevelopment pillars of malasakit (protective concern), pagbabago (change ortransformation), and kaunlaran (development), and the vision of Ambisyon 2040. Itfactors in and considers country commitments to the global community as embodiedin the 2030 Sustainable Development Goals, the 2025 Global Targets for Maternal,Infant and Young Child Nutrition, and the 2014 International Conference onNutrition.2.It is a results-based plan with SMART results at different levels designed in a resultsframework.3.It consists of 8 nutrition-specific programs, and initial list of 10 nutrition-sensitiveprograms, and 3 enabling programs. Member agencies of the National NutritionCouncil (NNC), namely, Department of Health, Department of Agriculture,Department of Social Welfare and Development, Department of Education,Department of Budget and Management, Department of Labor and Employment,Department of Trade and Industry, National Economic Development Authority,Department of Interior and Local Government, and the Department of Science andTechnology, other national government agencies, local government units (LGUs),non-government organizations (NGOs), academic institutions, and developmentpartners can undertake one or more of these programs. For better accountability, amember agency of the NNC Governing Board has been designated as lead for theseprograms. For some programs, the designated lead is the NNC Secretariat.4.The PPAN 2017-2022 comes with a budget estimate for the entire period of six years.The plan has a monitoring and evaluation framework showing the plan for progressmonitoring and evaluation through the six-year period.5.The National Nutrition Council Secretariat led and coordinated the plan formulation.Plan formulation started with the conduct of a nutrition landscape analysiscommissioned by NNC with support from Micronutrient Initiative, now NutritionInternational, and the United Nations Children’s Fund (UNICEF). A team of FilipinoPhilippine Plan of Action for Nutrition 2017-22 Executive Summary1
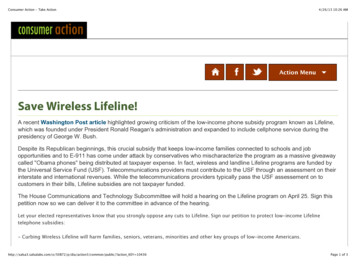
consultants conducted the assessment from August to October 2016 using landscapeanalysis based on document reviews, focus group discussions (FGDs), key informantinterviews, inter-sectoral consultations and validation meetings with a wide range ofstakeholders. The results of the analysis are contained in a separate document,“Situation Analysis of Nutrition in the Philippines”. However, its key findings are inthe first part of the plan document.6.Plan formulation was participatory, inter-sectoral, and multi-level. It engaged theparticipation of the NNC member agencies and their department senior officials atthe national and regional levels as well as members of provincial and municipalnutrition committees of LGUs where the FGDs were held, i.e. 6 regions, 5 provinces,and 22 cities and municipalities.7.Two consultation meetings, prior to the drafting of the plan and after the plan wasdrafted, were convened to ensure a wide participation in plan formulation.8.The first round of consultation with an inter-sectoral group of 16 agencies joined bydevelopment partners and the academe was held in Tagaytay City on 12-16September 2016. During the consultation, the national nutrition situation wasreviewed together with issues related to policy and program formulation andimplementation. The overall strategy and programs for PPAN 2017-2022 was agreedon during this consultation.9.The second round of consultation was held in Cebu on 17-18 November 2016.During this consultation, more specific directions for the programs identified in theTagaytay workshop were discussed and refined.10.This was followed by two more meetings of the NNC Technical Committee on 23November 2016, and 12 January 2017 before the final approval of the NNCGoverning Board on 21 February 2017.11.Even as the PPAN 2017-2022 was being formulated, related concerns were broughtinto discussions of relevant sectors of the Philippine Development Plan, e.g.agriculture, fisheries and forestry.12.The PPAN 2017-2022 is divided into two parts: Part 1 consists of a summary of thesituation analysis of nutrition in the country in 2016; and Part 2 presents the plan.Nutrition problems to be addressed13.High levels of stunting and wasting among children under-five years of age, withlevels that have remained unchanged over the years (Figure 1). Also stunting isrelatively low among infants 0-11 months old, but is significantly higher among oneyear olds (Figure 2). The prevalence of stunting remains high for the older children.Philippine Plan of Action for Nutrition 2017-22 Executive Summary2
Figure 1. Trends in the Prevalence of Malnutrition among Children Under FiveYears Old: National Nutrition Surveys (NNS), 86.07.38.030.321.52010 6.21.1019897.5 ight-for-heightSource: FNRI-DOST. 1989-2015 NNSFigure 2. Trends in the Prevalence of Stunting in Children from Birth to ThreeYears:NNS, 2008to 201514.Deficiencies in vitamin A, iron, and iodine particularly among groups for which theproblem is of public health significance (Table 1)Philippine Plan of Action for Nutrition 2017-22 Executive Summary3
Table 1. Prevalence rate of micronutrient malnutritionMicronutrient deficiency/Populationgroup affectedPrevalence rate200820112013Vitamin A deficiency: % of children 6mos-6 years old with low to deficiencyserum retinol15.2No data20.4Anemia: % of anemic women ofreproductive age (20-39 years old)18.6No data11.7Iodine deficiency:--Median urinary iodine concentration ug/L (Should be 100 ug/L for children 612 years old, and lactating women, and 150 ug/L for pregnant women)o Children, 6-12 years old132No data168o Pregnant women105No data105o Lactating women81No data77Percent with iodine excretion concentration 50 mcg/L (should be less than20%)o Children, 6-12 years old19.716.4o Lactating women34.034.3Source: FNRI-DOST. 2008-2015 NNS15.Hunger and food insecurity with 68.3% of Filipino households not meeting theircaloric requirements. While this level is lower than that recorded in 1989 (74.1%) itis higher than the level reported in 1998 (57%) and 2008 (67%).16.At the same time, overweight and obesity among various population groups shouldbe addressed, especially among adults (Figure 3).Philippine Plan of Action for Nutrition 2017-22 Executive Summary4
Figure 3. Overweight and obesity among various population groups17.Maternal nutrition should also be addressed as survey results have shown that theprevalence of nutritionally-at-risk women has not improved over the years, with aprevalence rate between 24-26% since 2008. Furthermore, adolescent pregnantwomen, those of poor educational attainment, coming from the poorest wealthquintile, and are employed have relatively higher levels of undernutrition (Figure 4).Maternal nutrition could also affect the nutrition of the growing fetus.Figure 4.Prevalence of Nutritionally At-Risk Pregnant Women by Age,Educational Attainment, Place of Residence and Wealth IndexWealth indexAge (years) 20Richest21.9 20Rich39.6Educational attainmentCollege, gra duate1524.1Poorest24.420.8PoorestVoc ational graduate19.8Place of residence27.7High school gra duate28.6High school undergrad22.1MiddleCollege, undergraduteVoc ational under graduate18.629.7Rural23.8Urban24.824.3Elem graduateWor king/employment status18.3Elem , not com pletednon-working30.5No gr ade completed490102030405026.4Wor king6017.9010203040Source: FNRI-DOST. 2015 National Nutrition Survey18.Poor infant and young child feeding in the first two years of life coupled with boutsof infection can explain the high levels of stunting.19.Exclusive breastfeeding (EBF) in the first six months of life continues to be achallenge. EBF increased from 48.9% in 2011 to 52.3% in 2013 but went back toPhilippine Plan of Action for Nutrition 2017-22 Executive Summary5
48.8% in 2015. However, a look at EBF rates by single age group within the 0-5months-old band would show declining EBF with the lowest rate among the 5-montholds (Table 2). The low rate of EBF together with the rate of never breastfedrepresent sub-optimal breastfeeding practice. These low rates deprive the infant ofneeded nutrients for optimum growth at the time when his or her growth is mostrapid.Table 2.Proportion of exclusive breastfeeding among infants 0-5 months old, bysingle age. Philippines, 2011 – 2015Age in monthsExclusive breastfeeding, in %201120132015All e: NNS 2011. 2013, and 2015, DOST-FNRI.Note: CV of estimates are 10% for all the age groups, except for the 5 -month old group for which theCV is 10.5 in 2011, 13.2 in 2013 and 12.8 in 2015 and are considered acceptable.20.By the sixth month of life, the infant should receive nourishment from solid andsemi-solid food, in addition to breastmilk. However, only 15.5% of infants 6-23months old receive the minimum acceptable diet1.21.As shown in Figure 5, the age group 6-11 months old are the worst off for thisindicator. Furthermore, while the highest wealth quintile has higher proportion ofchildren 6-23 months old with minimum acceptable diet, the level is still low at lessthan 20%. Thus, the problem for achieving optimum complementary feeding is notsimply rooted on income.1Minimum acceptable diet is based on the minimum frequency of feeds and diet diversity or consumption offoods from four groups of a group of seven groups that include grains, roots, and tubers; legumes and nuts;dairy products (milk, yogurt, cheese); flesh foods (meat, fish, poultry and liver/organ meats); eggs; vitamin -Arich fruits and vegetables; and other fruits and vegetables.Philippine Plan of Action for Nutrition 2017-22 Executive Summary6
Figure 5. Percent of children consuming minimum acceptable diet, Philippines2013Source: NNS 2013, DOST-FNRICausality of malnutrition22.Figure 6 shows a framework for the causality of child and maternal undernutrition.The framework notes undernutrition to arise from the immediate causes ofinadequate dietary intake and disease. These immediate causes are, in turn, linkedwith underlying causes at the household and communitylevels that include foodinsecurity, poor caring and feeding practices, and poor home environmentalconditions and inadequate health services. However, these immediate andunderlying causes are further linked to basic causes at the society level that coversamong others, low access and control of resources.23.While the framework in Figure 6 is a globally accepted, and used framework, aframework that integrates under- and overnutrition in one framework has beendeveloped for use in the ASEAN region (Figure 7).24.Thus, addressing both under- and overnutrition should involve actions to eliminateor reduce the negative impact of the identified causal factors.Philippine Plan of Action for Nutrition 2017-22 Executive Summary7
Figure 6. Causal framework of child and maternal undernutritionFigure 7. Conceptual framework of malnutritionPhilippine Plan of Action for Nutrition 2017-22 Executive Summary8
Goal25.To improve the nutrition situation of the country as a contribution to:a.The achievement of Ambisyon 20402 by improving the quality of the humanresource base of the countryb.Reducing inequality in human development outcomesc.Reducing child and maternal mortalityObjectives26.PPAN 2017-2022 has two layers of outcome objectives, the outcome targets and thesub-outcome or intermediate targets. The former refers to final outcomes againstwhich plan success will be measured. The latter refers to outcomes that willcontribute to the achievement of the final outcomes.Outcome targetsa.To reduce levels of child stunting and wastingIndicator 1 Prevalence (in percent) of stunted childrenunder five years old Prevalence (in percent) of wasted children1Baseline2022Target33.421.4 Under five years old7.1 5 6 – 10 years old8.6 5Ba s eline based on 2015 updating national nutrition s urvey conducted by the Food a nd Nutrition ResearchIns titute.b.To reduce micronutrient deficiencies to levels below public healthsignificanceIndicator 1Baseline2022TargetVitamin A deficiency Prevalence (in percent) of children 6 monthsto 5 years old with vitamin A deficiency (lowto deficient serum retinol)Anemia20.4 15 11.76.0Prevalence (in percent) of anemia among2Ambisyon 2040 is the Philippines’ long-term vision, i.e. “By 2040, the Philippines shall be a prosperous,predominantly middle-class society where no one is poor, our people shall live long and healthy lives, be smartand innovative, and shall live in a high-trust society. The Philippine hereby aims to triple real per capitaincome, and eradicate hunger and poverty by 2040, if not sooner” (Executive Order 05, October 2017).Philippine Plan of Action for Nutrition 2017-22 Executive Summary9
Indicator 1Baseline2022Target168 100women of reproductive ageIodine deficiency disorders Median urinary iodine concentration, mcg/L- Children 6-12 years old-Pregnant women105 150-Lactating women77 100Percent with urinary iodine concentration 50 mcg/L-Children 6-12 years old16.4 20-Lactating women33.4 201Ba s eline based on 2013 na tional nutrition s urvey conducted by the Food a nd Nutrition Research Institutec.No increase in overweight among childrenIndicator Baseline2022TargetPrevalence (in percent) of overweight Under five years old13.8 3.8 6 – 10 years old28.6 8.61Ba s eline based on 2015 na tional nutrition s urvey conducted by the Food a nd Nutrition Research Institute2Ba s eline based on 2013 na tional nutrition s urvey conducted by the Food a nd Nutrition Research Instituted.To reduce overweight among adolescents and 22 Target 528.01Ba s eline based on the 2013 na tional nutrition s urvey conducted by the Food a nd Nutrition Research InstitutePhilippine Plan of Action for Nutrition 2017-22 Executive Summary10
Sub-outcome or intermediate outcome targetsIndicatorBaselineTarget, 2022Reduce the proportion of nutritionally-at-risk pregnantwomen124.820.0Reduce the prevalence of low birthweight221.416.6Increase the percentage of infants 5 mos old who areexclusively breastfed124.733.3Increase the percentage of children 6-23 months old meetingthe minimum acceptable diet118.622.5Increase the percentage of households with diets that meet theenergy requirements 331.737.11Ba s eline based on 2015 updating national nutrition s urvey conducted by the Food a nd Nutrition Research InstituteBa s eline based on 2013 Na tional Demographic a nd Health Survey3Ba s eline based on 2013 na tional nutrition s urvey conducted by the Food a nd Nutrition Research Institute2Guiding Principles27.Attainment of nutritional well-being is a main responsibility of families butgovernment and other stakeholders have the duty to assist those who are unable toenjoy the right to good nutrition28.Priority will be given to the nutritionally vulnerable (pregnant women, lactatingwomen, infants and young children 0-23 months old), and nutritionally-affected(those who are already malnourished) from poor families and communities that haveless access to resources and services29.Participation of various stakeholders, including members of the community, in policyand plan formulation, implementation, monitoring and evaluation30.Gender sensitivity31.Efficiency and effectiveness in resource allocation and implementation of programsand projects32.Adherence to the principles of engagement of the Scaling Up Nutrition Movement asfollowsa.Transparency about intentions and impactb.Inclusivenessc.Being rights-basedd.Willingness to negotiatee.Predictability and mutual accountabilityPhilippine Plan of Action for Nutrition 2017-22 Executive Summary11
f.Cost-effectivenessg.Continuous communicativenessh.Acting with integrity and in an ethical manneri.Mutual respectfulnessj.Doing no harmStrategic Thrusts33.Focus on the first 1000 days of life. The first 1000 days of life refer to the period ofpregnancy up to the first two years of the child. This is the period during which keyhealth, nutrition, early education and related services should be delivered to ensurethe optimum physical and mental development of the child. This is also the periodduring which poor nutrition can have irreversible effects on the physical and mentaldevelopment of the child, consequences of which are felt way into adulthood.34.Complementation of nutrition-specific and nutrition-sensitive programs. Thisstrategic thrust recognizes that malnutrition has immediate, underlying, and basiccauses, which should be addressed to achieve targeted nutritional outcomes. Thus,there is a need to implement and deliver nutrition-specific interventions. Theseinterventions “address the immediate determinants of fetal and child nutrition anddevelopment, i.e. adequate food intake and nutrient intake, caregiving andparenting practices, and low burden of infectious diseases .35.Intensified mobilization of local government units. To ensure that PPAN 2017-2022delivers the planned outcomes, 36 areas with the highest prevalence of stuntingbased on the 2015 Updating National Nutrition Survey will be prioritized formobilization of LGUs (Table 3). Mobilization will aim to transform low-intensitynutrition programs to those that will deliver targeted outcomes. It will involvecapacity building and mentoring of LGUs on nutrition program management totransform them to self-propelling LGUs able to plan, implement, coordinate, andmonitor and evaluate effective nutrition programs. This strategy is also expected tocomplement the interventions in the first 1000 days.Philippine Plan of Action for Nutrition 2017-22 Executive Summary12
Table 3. PPAN 2017-2022 Focus Areas Based on Stunting 6.17.18.36.Areas/ ProvincesAbraAgusan del rines NorteCamarines SurCapizCatanduanesCotabatoEastern SamarIfugaoLanao del NorteLanao del .34.35.36.Areas/ ProvincesMaguindanaoMasbateMountain ProvinceNegros OccidentalNegros OrientalNorthern SamarOccidental MindoroPalawanQuirinoRomblonSamarSaranganiSouth CotabatoSultan KudaratSuluTawi-TawiZamboanga del NorteZamboanga SibugayReaching geographically isolated and disadvantaged areas (GIDAs), communities ofindigenous peoples, the urban poor especially those in resettlement areas. Effortsto ensure that PPAN 2017-2022 programs are designed and implemented to reachout to GIDAs and communities of indigenous peoples will be pursued. Thecommunity of NGOs and development partners’ resources will be engaged for thispurpose.There will also be efforts to reach the urban poor, especially those in resettlementareas.37.Complementation of actions of national and local governments. As LGUs arecharged with the delivery of services, including those related to nutrition, thenational government is charged with creating an enabling environment throughappropriate policies and continuous capacity building of various stakeholders.The combined impact of the programs from the national and local level is needed toensure the achievement of the desired outcomes. In this, there will be tworeinforcing strategies complementing one another, the implementation of NGAprograms and the delivery of nutrition services at the LGU level. This twinning ofvarious reinforcing projects will provide cushion for securing outcomes in case of ashortfall/gaps in the implementation of one of the programs.Philippine Plan of Action for Nutrition 2017-22 Executive Summary13
Program Framework38.Consistent with the recommendations from the Lancet Series on Maternal and ChildHealth and Nutrition in 2008 and 20133, the PPAN 2017-2022 will involve theimplementation of nutrition-specific and nutrition-sensitive programs (Figure 8). Theformer addresses the immediate causes of malnutrition, while the latter, theunderlying and basic causes.Figure 8. PPAN 2017-2022 Program FrameworkNutrition-specific programs39.Nutrition-specific programs are those that were planned and designed to producenutritional outcomes (Table 4). The selection of these nutrition-specific programswas inspired by global guidance like the WHO Essential Nutrition Actions, therecommendations of the Lancet Maternal and Child Nutrition Series, theInternational Conference for Nutrition 2 Framework for Action, among others.3The Lancet Series on Maternal and Child Health Nutrition is a collection of papers on evidence on maternaland child undernutrition – its nature, causality and needed action to address the problem. Two such serieshave been published, the first in 2008 and a follow-up publication in 2013.Philippine Plan of Action for Nutrition 2017-22 Executive Summary14
Table 4. Nutrition-specific programsProgramProject/ComponentAgencies involved1. Infant and youngchild feeding1.Health systems supportDOH, LGUs2.Community-based health andnutrition supportDOH, NGOs, LGUs,DevelopmentPartners (DPs)3.Maternity Protection andImproving Capacities ofWorkplaces on BreastfeedingDOLE, Employers,Employees’ Unions,NGOs, LGUs, DPs4.Establishment of breastfeedingplaces in non-healthestablishmentsAll agencies, NGOs,LGUs, DPs, CSC5.6.Enforcement of the Milk CodeEnhancement of Facilities(Including RUTF and RUSF) andprovision of servicesBuilding of Capacity of LocalImplementersDOH, LGUs8.Supplementary feeding ofpregnant womenDOH, NGOs, LGUs,DPs9.Supplementary feeding ofchildren 6-23 months oldDOH, NGOs, LGUs,DPs,NNC2. IntegratedManagement ofAcute Malnutrition7.3. National DietarySupplementationProgram5. Micronutrientsupplementation(vitamin A, iron-folicacid, multiplemicronutrientDOH, NGOs, LGUs,DP10. Supplementary feeding ofchildren 24-59 months oldDSWD, NGOs, LGUs,DPs, NNC11. Supplementary feeding of schoolchildrenDepEd, NGOs, LGUs,DPs12. Food plants for producingsupplementary foods4. National NutritionPromotion Programfor Behavior ChangeDOH, NGOs, LGUs,DP13. In schoolsFNRI, LGUs, SUCs,NGOsDepEd, NGOs, LGUs,DPs14. In communitiesDOH, DSWD, NGOs,LGUs, DPs15. In the workplaceDOH, DOLE, NGOs,LGUs, DPs16. Resource centerNNC (coordinator)17. In health unit18. In schoolsDOH, NGOs, LGUs19. Communication supportDOH, NGOs, LGUsPhilippine Plan of Action for Nutrition 2017-22 Executive SummaryDepEd, NGOs, LGUs15
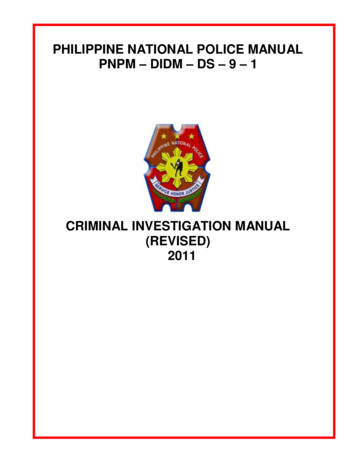
ProgramProject/ComponentAgencies involved20. Rice fortification with ironDOH, NNC, DSWD,DepED, NGOs, LGUs,industry21. Flour fortification with iron andvitamin ADOH, NNC, DSWD,DepED, NGOs, LGUs,industry22. Cooking oil fortification withvitamin ADOH, NNC, DSWD,DepED, NGOs, LGUs,industry23. Sugar fortification with vitamin ADOH, NNC, DSWD,DepED, NGOs, LGUs,industry24. Salt iodizationDOH, NNC, DSWD,DepED, NGOs, LGUs,industryDOH, DSWD,National/LocalNutrition Cluster,National/LocalDRRMC, NGOs,LGUs, DPsDOH, DSWD, DOLE,NGOs, LGUs,industry, CSC, DPsDOH, DSWD, DOLE,NGOs, LGUs,industry, CSC, DPsDOH, DSWD, DOLE,NGOs, LGUs,industry, CSC, DPspowder, zinc)6. Mandatory foodfortification(technologydevelopment,capacity building,regulation andmonitoring,promotion)7.Nutrition inemergencies25. Capacity building formainstreaming nutritionprotection in emergencies8.Overweight andObesityManagement andPrevention Program26. Healthy Food Environment27. Promotion of healthy lifestyle28. Weight ManagementIntervention (for Overweight andObese Individuals)Nutrition-sensitive programs40.Complementing these nutrition-specific interventions are nutrition-sensitiveprograms. These are development programs and projects that will be tweaked toproduce nutritional outcomes. Tweaking can be done by targeting households withundernourished children or nutritionally-vulnerable groups, or targeting areas withhigh levels of malnutrition, or being a channel for delivering nutrition-specificinterventions. Table 5 shows an initial list of development programs and projectsthat will be tweaked to produce nutritional outcomes in addition to their originalobjectives. The list will be updated in the course of plan implementation.Philippine Plan of Action for Nutrition 2017-22 Executive Summary16
Table 5. Nutrition-sensitive programProjectAgency involved1. Farm-to-market roads and child nutritionDA, LGUs2. Target Actions to Reduce Poverty and Generate EconomicTransformation (TARGET) and child nutritionDA, LGUs3. Coconut Rehabilitation ProgramPCA4. Gulayan sa PaaralanBPI, DepED5. Diskwento caravans in depressed areasDTI, LGUs6. Family development sessions for child and family nutritionprojectDSWD, LGUs7. Mainstreaming nutrition in sustainable livelihoodDSWD, LGUs8. Public works infrastructure and child nutritionDPWH, LGUs9. Adolescent Health and Nutrition DevelopmentDOH, LGUs10. Sagana at Ligtas na Tubig sa Lahat (SALINTUBIG) and otherprograms on water, sanitation and hygieneDOH, DILG, LWUAEnabling programs41.Mobilization of local government units for nutrition outcomes - This program aimsto deliver 36 provinces and the majority of its LGUs (total of 708 municipalities andcities), converting them from LGUs with low-intensity nutrition programs to onesthat deliver nutritional outcomes during the six-year period of the PPAN. It is one ofthe cornerstones of the PPAN 2017-2022.42.It is an essential part of the set of programs ensuring two contributions to the PPANplanned outcomes. One is by ensuring that the 36 focus provinces and their 708cities and municipalities deliver nutritional outcomes. Two, by inspiring andproviding models and practices that other provinces, cities, and municipalities canadapt.43.LGU mobilization is expected to facilitate convergence of services, that among otherswill involve national government agencies working in tandem with the demands ofthe LGUs being mobilized.a.Mobilization of Local Government Units for Delivery of Nutritional Outcomesthrough the NNC Regional Network that will start with the formulation orupdating the local nutrition action plan. Efforts will also ensure itsintegration in the annual investment program of the LGUs, and its fullimplementation. To catalyze related processes, inter-agency mobilizationteams at the national and local levels will be organized and provide technicalassistance to focus LGUs.Philippine Plan of Action for Nutrition 2017-22 Executive Summary17
44.b.Enabling Policy and Legal Framework for LGU Mobilization that will involvethe formulation of national issuances that will assist LGUs in managing theirlocal nutrition action plans.c.Development of Continuing Opportunities for LGU Excellence in NutritionProgramming that will generate success stories and good practices that LGUscan adapt.d.Mobilization of Rural Improvement Clubs and other community-basedorganizations for nutrition action to ensure the close link with the families inthe community.Policy development for food and nutrition - The ultimate goal in the current periodof the PPAN 2017-2022 is to secure important pieces of legislative, policy andbudgetary support that will enable the NGAs and the LGUs to implement the PPANmore robustly. Project 2 (Public Advocacy for Improved Support to Nutrition in thePhilippines) will expand and deepen the understanding and appreciation of nutritionin the public mind not just for the benefit of the PPAN 2017 -2022 but forgenerations beyond the current plan period.a.b.45.Securing policy support for improving nutrition, specifically along the prioritylegislative measures, that include the following:1)Regulation of the Marketing of Foods of Poor Nutritional Quality forChildren2)Amendment of PD 1569 Barangay Nutrition Scholar3)Program Strengthening and Institutionalization of the First 1000 DaysProgram4)Amendment of RA 8976 or the Food Fortification Act5)Adoption of Maternity Protection Policy (Extended Maternity Leave)6)Mandatory Plantilla Position for NAOs7)Creating a system of food distribution addressing the nutritionalneeds of the people8)Taxation of sugar-sweetened beveragesPublic advocacy for improved support to nutrition will apply variousstrategies to influence actions of national and local leaders.Strengthened management support to the PPAN 2017-2022 – by improving theefficiency and effectiveness in the planning, implementation, and overallmanagement of the nutrition specific and nutrition sensitive programs.a.Securing resource requirements (human, financial, and organizational, forPPANPhilippine Plan of Action for Nutrition 2017-22 Executive Summary18
b.Strengthening coordination, monitoring, evaluation and management ofPPAN across NNC including member agencies and NNC SecretariatService targets46.As a rule, 90% of the target population group of relevant nutrition-specificinterventions will be targeted. This is based on estimates of the Lancet Series onMaternal and Child Malnutrition that a 90% coverage of key services can result toreduced mortality and stunting at significant levels. An exception though is theprogram on obesity for which the target has been set to 50% of the targetpopulation.Implementation and Management Mechanism47.Operationalizing the PPAN 2017-2022 will involve the formulation of the NationalPPAN Implementation Plan also for the same time. This implementation plan willcover specific activities to be undertaken for each program for each year. It will beupdated annually to respond to the evolving situation. The implementation plan willinclude a resource framework with explicit estimates of funded and unfundedbudget
A call to urgent action for Filipinos and its leadership Executive Summary 1. The Philippine Plan of Action for Nutrition (PPAN) 2017-2022 is an integral part of the Philippine Development Plan 2017-2022. It is consistent with the Duterte Administration 10-poi