Transcription
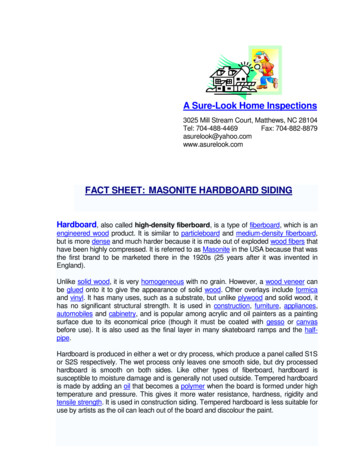
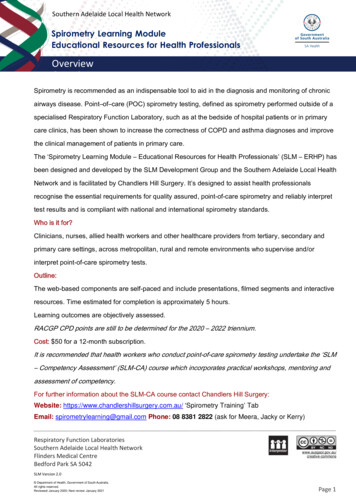
Fact SheetOvarian CystsIf you are reading this you have probably been toldyou have a cyst on your ovary and are worryingthat: it could be cancer it will affect your fertility (chances of having ababy) it may need surgery These are not true ‘cysts’ because they areunder 1cm in size and we call them follicles. On average, there are 5 -10 follicles in eachovary but this varies with age; young womengenerally have a lot of follicles, while women intheir 40s have only a few and women past themenopause usually have none.We hope this Fact Sheet answers some of yourquestions and reassures you that: ovarian cysts are common and often go away bythemselves ovarian cysts are seldom cancer (especially inwomen under 50 years, but even older women) ovarian cysts usually don’t prevent you fromfalling pregnant in the futureEach of these follicles houses an ‘egg’ which maybecome a baby if the egg is fertilised by a sperm.It is also reassuring to know that if surgery isneeded, it can usually be done via small cuts. Thisis called laparoscopic, or keyhole, surgery. Mostwomen go home the day of surgery, with very fewstaying one night in hospital. Complete recoveryfrom keyhole surgery generally takes a week or two.The normal ovary and its folliclesWomen have two ovaries on either side of theuterus (womb). Ovaries are extremely active inwomen under 50 years of age. They release an egg each month which, iffertilised by a sperm, can become a pregnancy. They produce female hormones called estrogenand progesterone which make the lining of theuterus (endometrium) ready for a pregnancy. Each month one follicle becomes the ‘dominantfollicle’ and grows to about 20 mm (2 cm) beforereleasing the egg. Once the egg has been released, the folliclechanges to form a structure called a corpusluteum. The corpus luteum is like a small factory,making large amounts of female hormones overthe next 10 days to prepare the lining of theuterus to receive a fertilised egg to form apregnancy. If the egg is not fertilised, the corpus luteumbegins to shrink and disappear, and a few dayslater, the lining of the uterus also comes awaywhich causes a menstrual period.123456-MenstruationMaturing follicleMature follicleOvulationCorpus luteumDeterioration of corpus luteumBefore the menopause, (that time in a woman’s lifewhen her periods stop forever), ovaries areapproximately 3 x 2 x 2cm in size but, because theyare so active, they change in size throughout themonth and from one month to the next.In young women, normal ovaries contain manysmall ‘cysts’ (fluid filled sacs) that can be seen onultrasound, or with the naked eye at surgery.Att: ShazzOvarian Cysts September 2018This written information is for guidance only and does notreplace consultation and advice by your health care provider.
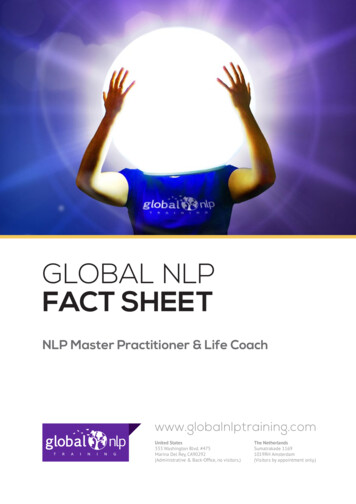
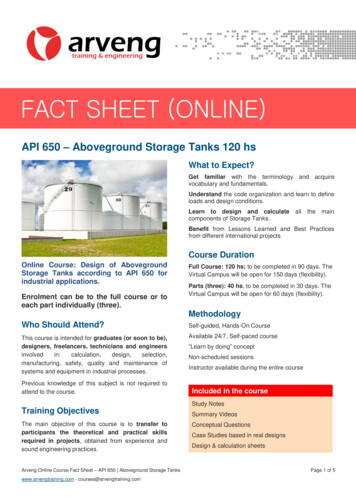
Fact SheetOvarian CystsSo what is the difference between a follicleand a true cyst?The difference is their size: a follicle is 10mm (2cm) or smaller a dominant follicle is 20-30mm or smaller an ovarian cyst is larger than 30mm (3cm) in sizeWe don’t usually consider surgery unless a cyst islarger than 50-60mm (5-6cm) although that maydepend on what the cyst looks like and whatsymptoms it causes. Ovarian cysts are so commonthat nearly every woman will have one at somestage in her life. Many women will have noproblems related to the cyst.What types of ovarian cysts are there?There are three main groups of ovarian cysts:1. Functional (physiological) cystsThese form when the dominant follicle andcorpus luteum do not behave as they normallywould during a particular menstrual cycle. Theyare therefore called either: Follicular cysts Corpus luteum cystsThey are common and mostly go away (resolve)by themselves without treatment.Functional CystsThese cysts form when the monthly ovarian cycledoes not follow its usual pattern. This is notsurprising – our bodies often make small mistakesin normal function. Follicular cysts form when the follicle does notrelease an egg but instead continues to swell upwith fluid. In the same way, a corpus luteum cyst formswhen the corpus luteum does not shrink awaybut continues to grow in size. Usually it will befilled with clear or light yellow fluid but it cancontain blood.Functional cysts are common and usually go awayby themselves, but this can take 2 – 3 months. Afterthe cyst goes away, the ovary usually goes back toworking normally. From time to time, anotherfunctional cyst may occur.Not surprisingly, your period may not come at theright time in a cycle affected by a functional ovariancyst. Often the period comes later than expectedbut it can come earlier. However, once the cyst hasresolved, the menstrual cycles return to normal.2. Benign (non-cancerous) ovarian cysts Benign tumours / growthso Dermoid cysts (also called teratomas)o Cystadenomas Endometriomas (small or large blood-filledsacs in the ovary)3. Ovarian cancersOvarian cancers are rare in women before themenopause and even in post-menopausalwoman most ovarian cysts are not cancer.Ovarian Cysts September 2018Ultrasound showing a simple follicular cyst –a dark fluid filled space with smooth walls.This written information is for guidance only and does notreplace consultation and advice by your health care provider.
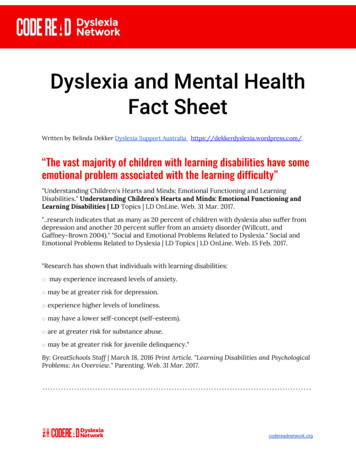
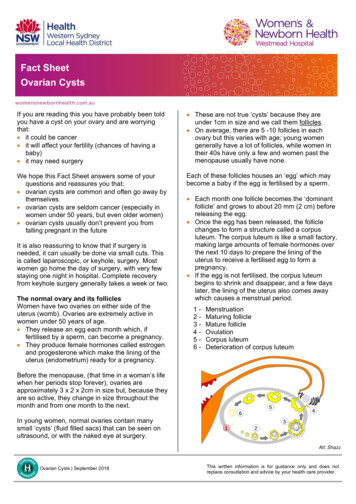
Fact SheetOvarian CystsBenign Tumours of the OvaryBenign (non-cancerous) tumours of the ovary arecommon.Dermoid CystsDermoid cysts are benign ovarian tumours whichcontain many different body tissues – fat, hair, skinand even teeth. They occur mostly in young womenand are even found in children. In women with adermoid cyst, 10% will have one in both ovaries(some may also develop one later in the otherovary).Dermoid cysts can usually be removed bylaparoscopic (keyhole) surgery as a one-dayprocedure.CystadenomasCystadenomas are benign tumours containing clear,water-like fluid or mucus fluid (like the mucus in asneeze). On ultrasound and at surgery, they oftenlook just like functional cysts - the difference is thatfunctional cysts usually go away over a few monthswhile cystadenomas keep getting bigger over time.Once a cystadenoma is about 5 - 6 cm in size andhas been there for several months (so it’s not likelyto be a functional cyst), you and your gynaecologistmay decide to have it removed, as it may twist theovary or burst in the future (both are not common).Cystadenomas can usually be removed bylaparoscopic (keyhole) surgery.Endometriomas (‘chocolate cysts’)Dermoid cyst of the ovaryAtt: By Photograph by Ed Uthman, MD. [Public domain],via Wikimedia CommonsDermoid cysts are ‘growths’, but many grow soslowly (1 – 2 mm per year) that surgery is often notrecommended unless they reach about 5cm(occasionally your gynaecologist may recommendremoving a smaller dermoid).At 5 cm, we advise removal of dermoid cysts, asthey may: cause the ovary to twist on itself (ovariantorsion); this is not common occasionally burstBoth of these complications usually cause suddensevere pain and may need urgent surgery.However, a burst cyst that is not bleeding heavily,may be managed by a ‘watch and wait’ approach.Ovarian Cysts September 2018Endometriomas are not tumours. They form whenthere is endometriosis involving the ovary.Endometriosis is a common condition where thelining of the uterus (endometrium) - which shouldonly be found inside the uterus - grows outside theuterus instead, forming small spots around thepelvis (inside the lower part of the tummy) includinginside the ovaries.These spots bleed when you have a period andform small, blood-filled cysts which gradually growbigger over time because the blood is trappedinside the ovary. This old blood is dark and thick,and looks like liquid chocolate, giving the cysts theirname.Endometriomas are common and are benign (notcancerous). If they are small and not causing anyproblems, they do not need to be removed. In fact,many women with an endometrioma don’t evenknow it is there. However, some endometriomascause pain, pressure symptoms, or problems withfertility (they may make it more difficult for you to fallpregnant).This written information is for guidance only and does notreplace consultation and advice by your health care provider.
Fact SheetOvarian CystsIn these cases, you and your gynaecologist maydecide that you have the endometrioma removed.Endometriomas can usually be treated bylaparoscopic (keyhole) surgery as a single dayprocedure.Cancerous Cysts of the OvaryIf there is concern that a cyst might be a cancer,your GP or gynaecologist will send you to a doctorwho specialises in women’s cancer. These doctorsare called gynaecological oncologists. Thisspecialist will carefully work out whether you have acancer, what type it is and make a plan for yourtreatment. Pain –o Usually mild and caused by the cyst wallstretchingo Occasionally quite sudden and severe if thecyst bursts, has sudden bleeding into it, orcauses the ovary to twist (ovarian torsion) Period bleeding not coming at the right time –either sooner or later than you expect Feeling faint and nauseous (need to vomit) – notoften, corpus luteum cysts can cause heavybleeding inside the abdomen (tummy) whichmakes you feel unwell and light headed butwithout much pain.What should I do if think I have an ovarian cyst?If your symptoms are mild then you should see yourGP, who will ask you about your symptoms andexamine you. It may be possible for your doctor tofeel a cyst by checking your abdomen or by vaginalexamination.What symptoms might ovarian cysts cause?The symptoms caused by a cyst depend on its sizeand how quickly it is growing. Many cysts cause nosymptoms at all and may only be found during anultrasound looking for something else.On the other hand, even quite small cysts maycause symptoms, including any of the following: Feeling full in your lower abdomen (tummy) Pressure feelings on the bladder which make youfeel like you need to urinate (wee) frequently, orpressure feelings on the bowels making it feeluncomfortable when you open your bowels (poo) Discomfort (pain) having sexOvarian Cysts September 2018Your GP will most likely request: A pap smear if it’s due. A pregnancy test if there is a possibility youmay be pregnant. A pregnancy in the wrongplace (the tube, rather than the uterus) can givesymptoms just like an ovarian cyst. This type ofpregnancy is called an ectopic pregnancy. [seeour Fact Sheet on Ectopic Pregnancy] A pelvic ultrasound (scan) – either through thetummy wall or else through the vagina (called atransvaginal scan). A scan through the vagina isclose to the ovaries and gives much clearerpictures than a scan through the tummy. Avaginal scan is not uncomfortable, especiallysince it doesn’t need a full bladder. Ultrasound isexcellent at seeing a cyst on the ovary andworking out what kind of cyst it is. Rarely, ovarian cysts can cause particular bloodtests to become abnormal. Your doctor willdecide if you need these tests.This written information is for guidance only and does notreplace consultation and advice by your health care provider.
Fact SheetOvarian CystsManagement of an Ovarian CystIf you have an ovarian cyst, managing it will dependon what type of cyst it is, how big it is, and whatproblems you are experiencing. Functional cysts can be watched for a fewmonths as they will usually go away on their own. You and your gynaecologist may decide to havethe cyst removed if it:o does not go away on its own after 3 monthso is causing significant pain or pressuresymptomso is quite big (more than 6cm)o is a type of cyst that does not go away byitself (like a dermoid)Removal of a cyst can usually be done withkeyhole surgery (laparoscopy).Sometimes big cysts need a larger cut on theabdominal (tummy) wall. This operation is called alaparotomy and you will usually need to stay inhospital for 2-3 days after the operation. It alsotakes a longer to fully recover from this type ofsurgery.Managing ovarian cysts before and after themenopauseBefore the menopause (when the ovaries stopfunctioning and your periods stop completely), it isusual to try and remove the cyst (ovariancystectomy) but keep the ovary. Sometimes it maybe necessary to remove the whole ovary(oophorectomy). Remember that, because you haveanother ovary, your fertility and hormones areusually not affected by losing one ovary.After the menopause it is more common to removethe entire ovary and tube at the same time as thecyst. This is not because the cyst is cancer, or evenmight become cancer, but because there is nobenefit trying to save the ovary at this age whenremoving it lessens the chance that you maydevelop a cancer in that ovary/tube some yearslater.Ovarian Cysts September 2018What about taking the oral contraceptivepill?Taking the pill: Will not treat a cyst if it is already there, it isbetter to wait for the cyst to go away by itself. Reduces the chance of getting functional ovariancysts (follicular cysts and corpus luteum cysts)because it stops ovulation. It is worth consideringgoing on the pill if you often develop functionalcysts. Reduces your chance of developing cancer ofthe ovary. Does not reduce the chance of developing abenign tumour of the ovary (dermoid orcystadenoma).What if I have severe pain?If you experience severe pain, nausea, or arefeeling faint, you should get someone to take you tohospital or call an ambulance. Further care willdepend on the diagnosis your medical team makesafter examining you and looking at your ultrasoundand other tests.Treatment may be: Urgent surgery (usually keyhole laparoscopicsurgery) - generally needed for:o Ovarian torsion (twisting of the ovary)o A cyst that is bleeding heavily[Please read our fact sheet on Laparoscopy] Giving painkillers and watching / waiting is oftenthe best treatment when there is no sign oftorsion and little or no blood in the pelvis. In suchconditions, the pain will generally settle within 24– 48 hours. This works for:o sudden bleeding inside a functional cyst –usually a ‘haemorrhagic (bleeding) corpusluteum’.o a cyst that has burst but is not bleedingheavily.This written information is for guidance only and does notreplace consultation and advice by your health care provider.
Fact SheetOvarian CystsIf you have symptoms which you maythink are due to an ovarian cyst, pleasetalk about them with your doctor. If acyst is found, remember that most goaway without needing surgery. Largercysts which do not go away can usuallybe treated with a day surgery. Mostcysts are not cancer and earlytreatment of ovarian cancer increasesyour chances of being cured.Other causes of ‘cysts’Sometimes cysts form in structures near the ovariesand it can be tricky for an ultrasound to tell exactlywhere the cyst is growing. While there can rarely becysts near the bowel and bladder, the mostcommon place for other cysts to form is in, or near,the fallopian tubes. Hydrosalpinx (‘water in the tube’) – this is wherethe fallopian tube swells up with fluid, it is oftenthe result of a past infection with a sexuallytransmitted infection such as chlamydia orgonorrhoea. A hydrosalpinx can affect fertility. Paraovarian cyst – a cyst in a fold of tissue nextto the tube and ovary which generally requires notreatment. Para-fimbrial cysts – small ( 1cm) cysts thatgrow from the end of the tubes; extremelycommon, present in at least 25% of women;rarely need treatment. Ectopic pregnancy - a pregnancy in the wrongplace (the tube) rather than the uterus cansometimes look like an ovarian cyst onultrasound.Ovarian Cysts September 2018What about Polycystic Ovaries (PCO)? PCO means ‘many cysts on the ovary’ but the‘cysts’ that are seen in this condition are not truecysts – instead PCO actually means having lotsof small follicles (2 – 9mm). Lots of follicles are often normal for youngwomen and is not usually Polycystic OvarySyndrome (PCOS), particularly if they haveregular periods and no abnormal facial or bodyhair. If a woman only has a period every few monthsand/or she also has a problem with facial/bodyhair and acne, she may have PCOS. In PCOS,the hormones do not follow the normal menstrualcycle. The woman has many small ovarianfollicles. These are not true ovarian cysts andthey should not be removed.[Please see our factsheet on Polycystic OvarySyndrome (PCOS)]This written information is for guidance only and does notreplace consultation and advice by your health care provider.
ultrasound, or with the naked eye at surgery. These are not true ‘cysts’ because they are under 1cm in size and we call them follicles. On average, there are 5 -10 follicles in each ovary but this varies with age; young women generally have a lot of follicles, wh