Transcription
Students and Foundation Trainees in Otolaryngology (SFO UK)SFO UKENT UK t/a BACO & BAO-HNSRoyal College of Surgeons35-43 Lincoln's Inn FieldLondonWC2A 3PE 442074058371support@entuk.orgEar, Nose and Throat: The Official Handbook for MedicalStudents and Junior DoctorsBy the Students and Foundation Doctors in Otolaryngology (SFOUK)Part of ENT UK
Authors and EditorsAlexander YaoMichaella CameronCharlotte McIntyreJohn AllenMamoona Khalid-RajaJayesh DoshiAndrew RobsonDheeraj KaramchandaniRoland HettigeEamon ShamilIrfan SyedNimesh Patel
ContentsIntroductionPrefaceForewordA Career in Ear, Nose and Throat SurgeryFurther InformationGeneric Skills in ENTGeneral ENT HistoryEar ExaminationNasal ExaminationNeck and thyroid status examCranial Nerve ExaminationOtologyEar AnatomyDizziness and VertigoHearing LossTinnitusFacial Nerve PalsyOtalgiaOtorrhoeaOtitis ExternaAcute Otitis MediaOtitis Media with EffusionChronic Otitis MediaCholesteatomaRhinologyNasal Function and AnatomyEpistaxisNasal obstructionFractured NoseSeptoplasty/SeptorhinoplastyRhinitis and Rhinosinusitis
Allergic RhinitisNon-Allergic RhinitisAcute RhinosinusitisChronic RhinosinusitisNasal PolypsOther Sinonasal LesionsCleft Lip and PalateHead and NeckHead and Neck AnatomyFacial MusclesBlood Supply to the Face and NeckThe Major Salivary GlandsOral CavityTopography of the NeckFascial Layers of the NeckNervous Supply of the Head and NeckPhysiology of SwallowingTaking History of a Neck LumpCauses of Neck LumpBranchial CystsDysphagiaDysphoniaTonsillitisPharyngeal PouchGlobus PharyngeusThyroid MassesThyroglossal cyst or sinusMultinodular goitreThyroid cancerBenign and Malignant Neoplasms of the Salivary GlandsCarcinoma of the Oral CavityCarcinoma of the PharynxCarcinoma of the NasopharynxCarcinoma of the OropharynxCarcinoma of the HypopharynxCarcinoma of the Larynx
Laryngopharygeal refluxSnoring and Obstructive Sleep ApnoeaENT EmergenciesAcute Airways ObstructionEpistaxis (Nose Bleed)Foreign body in the noseNasal septum haematomaForeign body in the earPerforated tympanic membraneFB in the pharynx or oesophagusDeep neck space infectionsPenetrating neck traumaMedications in ENTAntibioticsSteroidsAntihistaminesVestibular sedatives & Meniere’s diseasePractical Procedures in ENTNasal CauteryAnterior Nasal PackingNasendoscopyOto-Microscopy and Foreign Body RemovalENT InvestigationsPure Tone AudiometryAudiogram Case Study 1Audiogram Case Study 2TympanometryHearing Tests In ChildrenENT OperationsGrommet InsertionMiddle ear and Mastoid surgeryTonsillectomy
AdenoidectomyFunctional Endoscopic Sinus SurgeryParotidectomyThyroidectomyNeck DissectionTracheostomy
Introduction
PrefaceENT makes up a significant part of the clinical practice of generalpractitioners, paediatricians and emergency doctors althoughexposure to the specialty is often limited during undergraduatetraining.This “E-book” has been written to provide a practical guide to theday-to-day management of common ENT conditions and will behelpful to medical students and junior doctors as well as otherclinicians that have exposure to ENT as part of their practice. It hasbeen developed by the Students and Foundation Doctors inOtolaryngology group (SFO UK), which is part of ENTUK. The groupaims to provide support for undergraduates in medicine and juniordoctors with an interest in ENT. The content is based on a Delphistudy that set out what the most important topics should be in anundergraduate ENT curriculum taking in to consideration guidancepublished in Tomorrow’s Doctors by the General Medical Councilguidance.Congratulations to the authors and to my colleagues on the SFO UKcommittee for delivering an excellent and novel educationalresource. A number of individuals have been instrumental inproducing this E-book from conception to production.These include Alex Yao, Michaella Cameron, Charlotte McIntyre,John Lee Allen and Mamoona Khalid-Raja. I also wish to particularlythank the section editors Andrew Robson, Dheeraj Karamchandani,Roland Hettige, Eamon Shamil, Nimesh Patel & Irfan Syed as wellas James Tysome & Victoria Ward (Elf-ENT) for allowing us to usemany of their images.Mr Jayesh DoshiPhD FRCS (ORL-HNS) MMedConsultant OtolaryngologistChairman of SFO UK committee (2018)
ForewordEar, Nose, and Throat (ENT), or otorhinolaryngology, is an important,interesting and diverse specialty. It covers a wide range of areasfrom the common, such as tonsillitis, to the highly specialised,including cochlea implantation, congenital airway disease, voicedisorders, skull base and facial plastic surgery.Whether you become a GP or an A&E doctor, you will encounterENT pathologies in abundance, some of which can be lifethreatening. Yet, students have limited exposure to the specialtywithin most undergraduate curricula.This book complements the national ENT curriculum written byENTUK. Although not designed to be a comprehensive text, thisbook aims to provide you with the most important topics that youshould know by the time you finish medical school and qualify as afoundation doctor. The book will also prove useful for foundationdoctors wishing to refresh and review their ENT knowledge.Topics are presented systematically in an easy-to-read formatsuitable for short attachments. Students may also find it useful to useas reference material chapters explaining common medicines,investigations, procedures, and operations specific to ENT.ENT is a very hands-on specialty and ENT doctors are generallyvery approachable! So make the most of every opportunity to exudeenthusiasm, watch and participate during your attachment!Professor Anthony NarulaConsultant OtolaryngologistMA MB BChir FRCS FRCS (Ed)President of ENTUK (2016)
A Career in Ear, Nose and ThroatSurgeryEar Nose and Throat (ENT) surgery or Otorhinolaryngology offers anexciting and varied surgical career option. It has been described as a‘cradle to grave’ specialty with a caseload ranging from a baby withhearing loss, teenager with allergic rhinitis to an elderly man withthroat cancer. As there is no separate medical companion, ENTsurgeons also manage the non-surgical care of their patients.Furthermore, once at registrar level, on calls can be done fromhome, which can be considered as particularly attractive.SubspecialtiesHead and Neck SurgeryOtologySkull Base Surgery/Neuro-OtologyThyroid and Parathyroid SurgeryRhinologyFacial Plastic SurgeryPaediatricsLaryngologyTypical working week4 clinics a week2 surgical sessions a weekLight emergency workMultidisciplinary work with other specialties (audiology, speech andlanguage therapist, endocrinologist, oncologists, plastic surgeons,maxillofacial surgeons and dermatologists)
Further Information Approach your local ENT team!ENT UK: www.entuk.orgStudent and Foundation Trainees in Otolaryngology (SFO UK):http://sfo.entuk.orgAssociation of Otolaryngologist in Training (AOT) :www.aot.ac.ukRoyal College of Surgeons of England: www.rcseng.ac.ukBritish Association of Paediatric Otolaryngology (BAPO):www.bapo.org.ukBritish Rhinological Society (BRS) :www.britishrhinologicalsociety.org.ukBritish Otolaryngology & Allied Sciences Research Society(BOARS) https://www.entuk.org/boars-sectionIntercollegiate MRCS ew
Generic Skills in ENT
General ENT HistoryPrinciples of history taking in ENTGood history taking is an essential skill to be maintained throughoutyour training. By building a good rapport, you will help the patientfeel more comfortable about discussing his/her symptoms. Itprovides the opportunity to explore a patient’s concerns andexpectations. After completing a thorough history, you should have agood idea of what the top differential diagnoses could be.Before starting Wash your hands Introduce yourself and ensure the patient is comfortable Maintain good eye contact and remember the importance ofdeveloping good rapport with the patient (and the parents ifpresent)Structure of history taking Presenting complaint (PC) ‘How may I help you today?’ History of presenting complaint (HPC) ‘ When did this problembegin’ Enquire about the relevant risk factors and other specificquestions relating to the presenting complaint. Do have atargeted list of questions for PCs related to “Ear”, “Nose”, and“Throat/Head Neck” (For targeted histories, go to the relevantsub sections of this booklet) Previous episodes - Severity, response to previous treatmentand hospitalisation Past medical history (PMH) Birth History – Particularly important for ear conditions inchildren Drug history (DH) - Including over the counter medication andvaccinations Allergies Family History
Social history (SH) - Do not forget to enquire about the impactthat the presenting complaint has had on quality of lifeSystems review - Also enquire on any tendency to bruise orbleed easilyAt the end of the history Summarise the patient’s history to them. Clarify that youunderstood them correctly and whether there is anything elsethat they would like to mention.
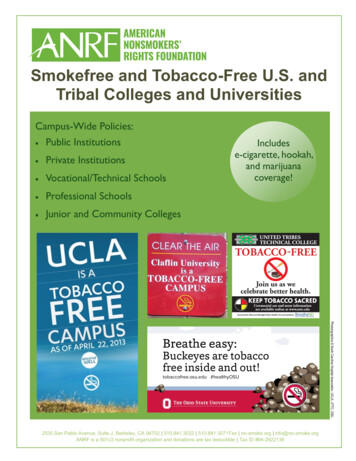
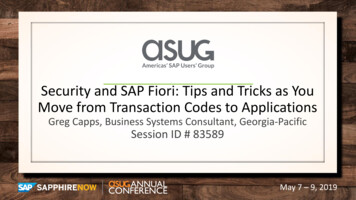
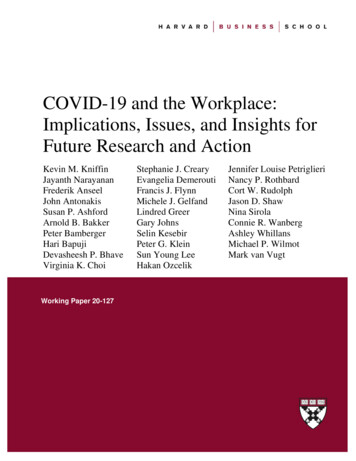
Ear examinationBefore starting Gel/wash your handsIntroduce yourself and ensure the patient is comfortableAsk about any pain or tendernessThe patient should be positioned on the chair and you shouldplace yourself to the side of the patient. In children, positioningis even more important. Children should be sat across theparent/nurses lap, with the side of the head held to the chest bythe carer’s hand (See Figure 1) Flailing arms can be securedwith the carer’s other hand. Ideally, aim to examine children asopportunistically as possible and incorporate play as part of theexamination.Figure 1: Correct positioning of a child for ear examInspectionFrom the front: note the size, assess symmetry of the pinna. Arethere differing degrees of protrusion? Is there an obviouslyabnormal pinna? For example, see Figure 2.
Figure 2: Congenital Microtia of the External Auditory CanalInspect each ear individually - Start with the normal earPre-auricular - Inspect for scars (previous parotidectomy ormiddle ear surgery), swelling (infection, parotid tumour),erythema (infection/ inflammation), sinuses, pits, fistulaePinna - Note any signs of erythema, swelling (infection,haematoma) or tendernessPost-auricular - Move pinna anteriorly to inspect behind thepinna. Note any post-auricular scars. Acute and/ or painfulswelling here suggests infection (mastoiditis or lymphadenitis)Examine the other ear. Note any difference.Otoscopy
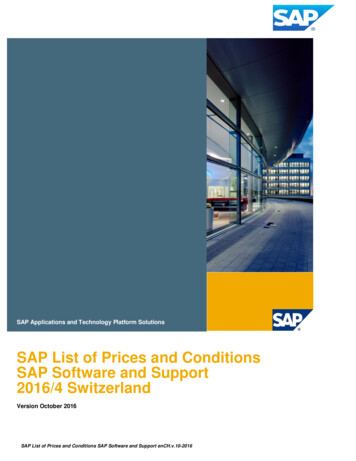
Ensure the otoscope has good magnification and illumination.Use the largest speculum that will fit comfortable in the externalauditory canal (EAC)Start with the “normal” earGently pull the pinna upwards and backwards to straighten theear canal to best visualise the tympanic membrane. In children,pulling the pinna downwards and backwards may provide bettervisualisationHold the otoscope like a pencil and use your little finger as afulcrum against the cheek to avoid injury should the patientmove suddenlyInspect systematicallyFigure 3: Normal right tympanic membraneExternal auditory canal: Wax or discharge, erythema, swelling(infection, trauma)Tympanic membrane (See Figure 3): Is there a normal lightreflex in the anteroinferior quadrant? Colour of drum - Normal isgreyish & translucent. Pink/red colouring can meaninfection/inflammation and white plaques can indicatetympanosclerosis. Position of drum - Retracted (cholesteatoma,infection), bulging (infection), perforation
Ossicles: The malleus, incus and stapes can be seensometimes through the tympanic membrane especially if there isa perforation.Pneumatic otoscopy can also be used to assess tympanicmembrane mobility – this modified otoscope has an air-tight sealwhen placed in the ear canal and a rubber bulb (similar to that ofa sphygmomanometer) which the user can squeeze whichalters the pressure within the ear canalHearing testsThese tests include the Pure Tone Audiogram (see Chapter:ENT Investigations - Pure Tone Audiogram).Examine a patient’s response grossly to your greeting. Can theyhear you? Is there a hearing aid being used?(i) Free field speech testingFree field testing is a good screening tool for hearing lossUse of masking improves the accuracy of testing: Rub thetragus of the contralateral ear whilst performing this to preventsound being heard in the contralateral non-test earUse polysyllabic phrase (number or letter) e.g. ‘C5’, ‘37’ ormotivational phrases in children e.g. ball, sweets, crispsTest normal ear first. Perform, in order of intensity at 60cm(arms length) and 15cm: whisper, conversational speech, loudvoice. Patient should be able to repeat 50% of theletters/numbers correctly.If he/she can repeat:Whisper at 60cm – Hearing better than 30dBWhisper at 15cm – Hearing better than 35dBConversational voice at 15cm - Hearing better than 55dBLoud voice at 60cm – Hearing worse than 75-90dB
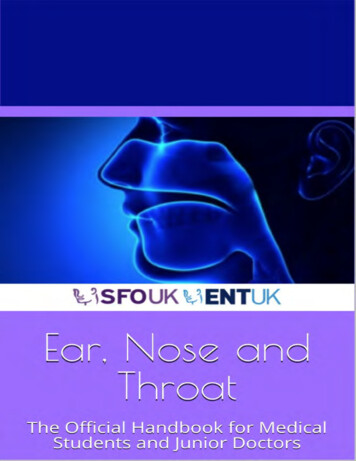
ii) Weber’s and Rinne’s testsThese tests assess air conduction (AC) and bone conduction (BC)and are used to help delineate whether hearing loss is sensorineural(SNHL)or conductive (CHL) in origin.Weber’s testFigure 4: Weber’s testVibrating 512Hz tuning fork applied firmly to the midline of theforehead, apex of head(see Figure 4)Ask the patient if he/she can hear a tone in the right ear, left earor centre of the headThe “louder” ear may be due to conductive hearing loss in thatear (sound travels through the bone), or sensorineural hearingloss in the other earYou can work out which this is by performing Rinne’s test.Rinne’s test
Figure 5: Rinne’s testPlace vibrating tuning fork with base on mastoid process(position 1, testing bone conduction). See Figure 5Then move the tuning fork so its prongs are adjacent to (but nottouching) the external auditory meatus (position 2, testing airconduction).Ask patient to tell you which is louder, when the fork is placedbehind the ear or in front of the earPosition 2 is louder than position 1 in the normal ear (PositiveRinne), as an intact hearing a
General ENT History Principles of history taking in ENT Good history taking is an essential skill to be maintained throughout your training. By building a good rapport, you will help the patient feel more comfortable about discussing his/her symptoms. It provides the opportunity to explore a patient’s concerns and expectations. After completing a thorough history, you should have a