Transcription
10/23/2015Consolidated Community Reporting Initiative (CCRI)Provider Enrollment Frequently Asked QuestionsWhat is the CCRI enrollment process?To ensure continuity, the CCRI county representative will be required to assist providers in thecompletion of the CCRI Base Enrollment Application with applicable addenda, complete theCounty CCRI Attestation Form and submit the completed enrollment application(s),documentation and Attestation Form(s) in one complete package. Providers do not haveaccess to the OMHSAS Intranet site; therefore each county mental health program isresponsible for providing a CCRI enrollment application and working with their base-fundedmental health providers in completing the application.Related Attachments: CCRI Provider Enrollment Tool, CCRI Provider Change/Closure Form,CCRI Provider Enrollment Application Short Form, CCRI Provider Enrollment Base Application(Long Form)What requires a CCRI Provider Enrollment Base Application (Long Form) and what requiresthe CCRI Provider Enrollment Application Short Form?The CCRI short form is exclusive to CCRI and is used for a provider who is currently enrolled,has a valid PROMISe Provider Identification Number and is requesting to have the EPOMSPEP added to this location for service(s) contracted and paid with county base funds.The CCRI Base Enrollment Form is used for a provider who is not otherwise enrolled in PAMedicaid and who does not have a current PROMISe Provider Identification Number for theservice(s) contracted through and paid with county base funds.Related Attachments: CCRI Provider Enrollment Tool, CCRI Provider Change/Closure Form,CCRI Provider Enrollment Application Short Form, CCRI Provider Enrollment Base Application(Long Form)For all other questions, issues or concerns with CCRI Provider Enrollment please contact CCRI Data Support@pa.gov1
10/23/2015How do I find out whether provider applications were added for our county and the applicationas successful?Once the enrollment occurs for the CCRI provider, a letter is generated and mailed to theCCRI provider and a copy of the letter is generated to the county that submitted the CCRIProvider Enrollment Application. The provider enrollments would then appear on the latestPRV416 file (i.e., the statewide file of PROMISe - enrolled CCRI providers).Related Attachments: PRV416 FileWhat is the difference between the PRV414 and the PRV416?The PRV414 is a weekly file that contains a statewide listing of all PROMISe -enrolledproviders in Pennsylvania and the adjoining states of New Jersey, Delaware, Maryland, Ohio,West Virginia, and New York. This file is utilized by HealthChoices managed careorganizations, as well as CCRI counties. It is sent to CCRI Counties as a resource to identifypotential mental health providers with which to contract, and to research PROMISe IDs forenrolled providers.The PRV416 is a CCRI-specific monthly file that contains all active and closed provider servicelocations with a PROMISe EPOMS PEP. For CCRI encounter reporting, the provider musthave an open EPOMS PEP on the date of service in the PROMISe system.Related Attachments: PRV416 File, PRV 414 FileDoes the PRV416 file sent to us from the Department verify that a provider is enrolledcorrectly with an EPOMS PEP in PROMISe ? In other words, if a provider is listed on the 416file with the correct provider type and specialty code, can we then assume that they arecorrectly enrolled for provider billing and county CCRI encounter data reporting?Yes, the monthly PRV416 file is your source for CCRI provider information. The county canuse the file to verify the accuracy of enrollment of the county’s providers. The informationcontained in that file should reflect all providers enrolled into PROMISe .Related Attachments: PRV416 FileWho receives notice of successful enrollment with CCRI from OMHSAS?When a provider is enrolled with the CCRI initiative, the provider receives the original letteridentifying the PROMISe provider ID and specific information relevant to the enrollment andthe county receives a copy of the letter.For all other questions, issues or concerns with CCRI Provider Enrollment please contact CCRI Data Support@pa.gov2
10/23/2015We have a few providers which we use on an occasional, as-needed basis (e.g., respite care).Should they be enrolled for the CCRI Initiative? We have contracts with them and pay on a perdiem cost basis.Yes. In order for CCRI encounters to be accepted, the providers must be appropriatelyenrolled in PROMISe with an EPOMS PEP.How are Purchased Drugs handled? Does every pharmacy need to be enrolled?You do not need to enroll pharmacies. Medication payments are not to be reported in EPOMS.They will continue to be reported in the Income & Expense Report.What cost centers are used for each individual service?This question can be answered by reviewing OMHSAS Bulletin 12-02.Related Attachment: OMHSAS Bulletin 12-02Who is responsible to submit CCRI revalidation information for continued enrollment inPROMISe ?The provider is responsible for submitting the re-validation information necessary for continuedenrollment in PROMISe . In addition, revalidation dates have been added to correspondencethat informs providers/counties of their revalidation enrollment date.Related Attachments: OMHSAS Bulletin 14-03If a provider is enrolled recently do they have to be CCRI revalidated again?Providers that initially enrolled with an effective date on or before March 25, 2011 will have tocomplete the re-enrollment process by March 24, 2016, and subsequent re-enrollments everyfive (5) years thereafter.Providers that initially enrolled after March 25, 2011 will not have to re-enroll until five (5) yearsfrom the date they were initially enrolled. They will also complete subsequent reenrollmentsevery five (5) years thereafter.For all other questions, issues or concerns with CCRI Provider Enrollment please contact CCRI Data Support@pa.gov3
10/23/2015How does a provider know their CCRI revalidation date?Providers can determine their next re-enrollment deadline by logging in to the provider portalfor each service location. The re-enrollment/revalidation date will be displayed in the mastheadof the provider portal for each service location. The date identified is the expiration date for thatspecific service location based on the most recent application on file with DHS/OMHSAS.When OMHSAS mails the confirmation letter out, we also include the revalidation date specificto the service location that was enrolled.What forms does the provider need to complete for the CCRI re-validation?Providers of CCRI, enrolled through the County MH Office will need to meet the requirementsset forth by the County. When the provider has met the County requirements, the County willprovide the current CCRI Base Provider Enrollment Application/required documentation andwill coordinate and submit the Provider Enrollment Application/documentation along with theCounty Attestation Form to OMHSAS at the address below, for processing.OMHSAS requires original hardcopy enrollment documents/supporting documentation, whichincludes original provider signature/dates.DHS/OMHSAS Business Partner Support Unit112 East Azalea Drive – 2nd FloorHarrisburg PA 17110Related Attachments: OMHSAS Bulletin 14-03, CCRI Provider Enrollment Application ShortForm, CCRI Provider Enrollment Base Application (Long Form)What effective date should be used on the CCRI revalidation?The date of when the provider is completing the application for revalidation.What specific services have to be CCRI revalidated for 2015? Is there a list of the services thatrequire revalidation?The Department must revalidate the enrollment of all providers, regardless of providertype/service at least every five (5) years.For all other questions, issues or concerns with CCRI Provider Enrollment please contact CCRI Data Support@pa.gov4
10/23/2015Is an attestation form required with the CCRI Encounter Submitters ProviderEnrollment/Revalidation Application?The County is the only entity that has a Provider Enrollment Submitter ID. The County doesnot need an attestation to approve the County Submitter ID.Related Attachment: CCRI Encounter Submitters Provider Enrollment/Revalidation ApplicationWith the upcoming electronic enrollment process is the only county responsibility incompleting the attestation form?OMHSAS will be establishing a webinar that explains how the electronic enrollment processwill work and confirm the role of the County.If I have questions about Provider Enrollment for CCRI who can I contact?All questions, issues or concerns about Provider Enrollment can be sentto CCRI Data Support@pa.gov. We will be able to provide prompt and accurate answers toquestions and inquiries received.Attachments:CCRI Provider Enrollment Application Short FormCCRI Provider Enrollment Base Application (Long Form)CCRI Provider Enrollment ToolCCRI Provider Change/Closure FormCCRI Encounter Submitters Provider Enrollment/Revalidation ApplicationOMHSAS Bulletin 12-02OMHSAS Bulletin 14-03PRV 414 FilePRV416 FileFor all other questions, issues or concerns with CCRI Provider Enrollment please contact CCRI Data Support@pa.gov5
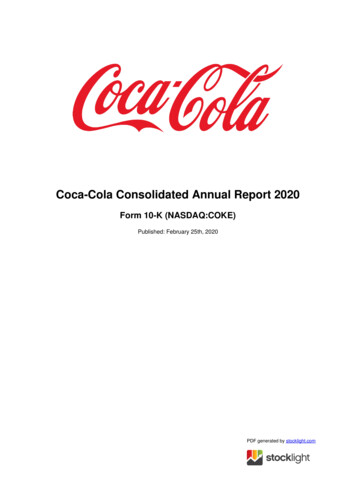
Commonwealth of PennsylvaniaOffice of Mental Health and Substance Abuse ServicesConsolidated Community Reporting Initiative Provider Enrollment ApplicationShort FormInstructions for Completing the Consolidated Community Reporting Initiative (CCRI) Provider EnrollmentApplication – Short FormThis application is for providers already enrolled in either Medical Assistance Fee-for-Service or HealthChoicesand requesting enrollment as a CCRI provider.1. Action Requested:Enter the effective date of enrollment and your 13 digit PROMISe provider ID number.2. Enrollee’s Name:List the applicant’s name (individual practitioner or facility) and date of birth (if applicant is an individual). Ifoperating under a fictitious business/doing-business-as (dba) name, attach copy of recorded/stampedfictitious business name statement/permit.3. Provider Type Number and Description:Enter the provider type number and the description of the provider type you are requesting enrollment for.4. Provider Specialty Number and Description:Enter the provider specialty and the description of the provider specialty you are requesting enrollment for.5.License number:Enter the professional or state license number, if applicable6. Physical Service Location:List the physical address where services will be provided. A Post Office Box is not a valid service location.6a. Mail to Information:Indicate the address where you want correspondence to be mailed. (e.g. notification of enrollment)7. Sign and date the application, print your name and list your telephone number. The signature should bethat of the individual applying for enrollment, or someone able to represent the facility applying forenrollment. Use black ink.Forward completed application to the county in which the CCRI contract is associated with.The County MH/MR representative will be required to complete and submit the “CCRIAttestation Form” to support the enrollment of this service provider along with the completedapplication.Page 1 of 3Updated 02/01/2013
Commonwealth of PennsylvaniaOffice of Mental Health and Substance Abuse ServicesConsolidated Community Reporting Initiative Provider Enrollment ApplicationShort FormThis application is for providers already enrolled in either Medical Assistance fee-for-service or HealthChoicesand requesting enrollment as a CCRI provider.1.Action Requested:Add the EPOMS PEP to an existing service location.Effective date of enrollment:PROMISe Provider ID & Service Location: /2.Enter Name of Enrollee:Facility Name:OrLast Name: First: Middle:Date of Birth: / /Ex: (2012/xx/xx)Gender:MaleFemale3. Provider Type Number and Description: /4. Provider Specialty Number and Description: /5. License Number: (Professional or State License, if applicable)6. Physical Service Location:6a. Mail to Information:( ) -( ) -StreetCityStateZip (9 digit)CountyStreetCityStateZip (9 digit)CountyPhonePhoneEmailEmail7. I certify that the information provided in this enrollment package is true to the best of my knowledge.( )Provider’s SignaturePage 2 of 3Printed NameTelephoneDateUpdated 02/01/2013
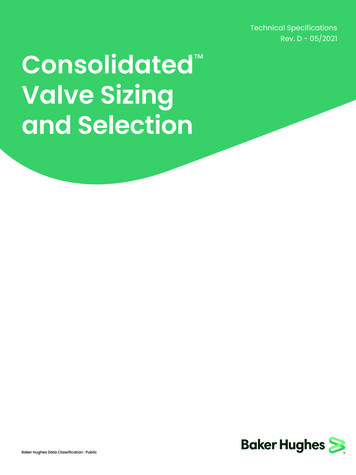
Commonwealth Of PennsylvaniaOffice of Mental Health and Substance Abuse ServicesConsolidated Community Reporting InitiativeAttestation FormCounty Name:CCRI County Contact Name:Print Namehas successfully completed theName of Providercredentialing process as a provider.Type of CCRI Service The population to be served is consistent with the requirements for this service. The County or County Contractor(s), where applicable, has/have approved the enrollment of thisprovider for the CCRI program.Provider Type Number and Description: /Provider Specialty Number and Description: /The requested effective date of the CCRI enrollment into PROMISe is ,CCRI County Contact SignaturePrinted NameDateSubmittal InformationThe county will submit the CCRI enrollment packet along with this CCRI Attestation Form to thefollowing address:DPW/OMHSASBusiness Partner Support UnitCCRI Enrollment112 East Azalea DriveHarrisburg, Pennsylvania 17110-3594Applications that are received directly from the provider will be returned unprocessed.Page 3 of 3Updated 02/01/2013
Commonwealth of PennsylvaniaOffice of Mental Health and Substance Abuse ServicesConsolidated Community Reporting Initiative Provider EnrollmentBase ApplicationInstructions for Completing the Consolidated Community Reporting Initiative (CCRI) ProviderEnrollment Base ApplicationTo the County: Refer to the County Funded Services document and/or the CCR POMS ReportingTool when assisting the provider in identifying the correct provider type/specialty combination specificto the service being paid for through the County contract.1. Action Requested:Check Initial Enrollment, check whether you are an individual or facility and enter the effective date ofenrollment.2. Enrollee’s Name:List the applicant’s name (individual practitioner or facility) and date of birth (if applicant is an individual). Ifoperating under a fictitious business/doing-business-as (dba) name, attach copy of recorded/stampedfictitious business name statement/permit.3. Tax Identification Information (TIN):List the enrollee’s Social Security Number (SSN) or Federal Employer Identification Number (FEIN).Enclose verification of the TIN with your application (e.g., a copy of Social Security card, W-2 or a copy ofan IRS-generated document containing the IRS number and name. Note: A W-9 is not acceptable proofof tax ID.)Enter the legal name as shown on the tax ID, and the corresponding current address, telephone and faxnumbers and contact information. (Note: Do not list tax information of entity to which payment will bemade if said entity is not the enrollee.)4. National Provider Identifier (NPI) #:List your 10 digit NPI # and taxonomy(s). Include a copy of your NPPES confirmation letter verifying yourNPI #.5. Business Type:Check the appropriate box for your business type (check one box only). Include corporation papers fromthe Department of State Corporation Bureau or a copy of your business partnership agreement, ifapplicable.6. Provider Type Number and Description:Enter the provider type number and the description of the provider type you are requesting enrollment for.Please contact the County MH/MR representative who will be assisting you in identifying the correctprovider type specific to the service being paid for through the County contract.7. Provider Specialty Number and Description:Enter the provider specialty and the description of the provider specialty you are requesting enrollment for.Please contact the County MH/MR representative who will be assisting you in identifying the correctprovider specialty specific to the service being paid for through the County contract.1 of 3Updated February 1, 2013
7a. Procedure code and modifier:This section applies to providers who are enrolling as one of the following provider types with 2153-53108-110 (only if enrolling for H2013)Enter the procedure code and modifier, if applicable, of the service you will be providing.8. Program Eligibility Maintenance:This block is already completed.9. License number:Enter the professional or state license number, if applicable10. Managing Employee or Agent Disclosure:Indicate whether you retain any managing employees or agents. If ‘yes’ please complete Attachment I –Managing Employee or Agent Disclosure Form11. Confidential Information:The individual applying for enrollment OR the representative of the facility applying for enrollment mustcomplete ALL confidential information questions. If “Yes” is answered to any of the questions, provide adetailed explanation and include it with your completed enrollment application.12. Physical Service Location:List the physical address where services will be provided. A Post Office Box is not a valid service location.Complete a separate Page 4 of the application for each intended physical service location.13. Mail To Information:Indicate the address where you want correspondence to be mailed. (e.g. notification of enrollment)14. Pay To Information:Indicate address where payments will be sent. Payments will be initiated via the county.15. Home Office Information:Indicate the entity’s headquarters address.16. Sign and date the application, print your name and list your telephone number. The signature should bethat of the individual applying for enrollment, or someone able to represent the facility applying forenrollment. Use black ink.2 of 3Updated February 1, 2013
Additional Required Forms:Also include as applicable: One DPW Outpatient Provider Agreement with original signature.Completed Ownership or Control Interest FormsCopy of DPW Certificate of Compliance, Department of State Licensure, or an appropriate license or atailored service description that supports the provider type/specialty being requested for enrollment.Verification of Tax ID name and number.Forward the completed application to the county in which the CCRI contract is associatedwith.The County MH/MR representative will be required to complete and submit the “CCRIAttestation Form” to support the enrollment of this service provider along with the completedapplication.Applications that are received directly from the provider will be returned unprocessed.3 of 3Updated February 1, 2013
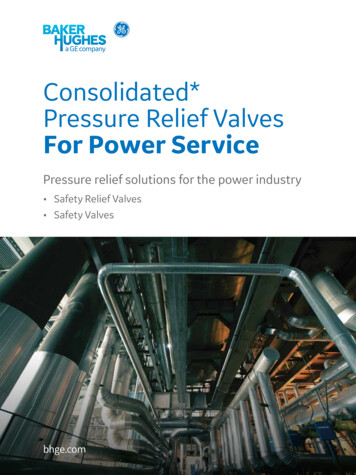
Commonwealth of PennsylvaniaOffice of Mental Health and Substance Abuse ServicesConsolidated Community Reporting Initiative Provider EnrollmentBase ApplicationPage 1 of 4For OMHSAS Internal Use Only1.PROMISe ID /Action Requested:Initial Consolidate Community Reporting Initiative Enrollment (New)IndividualFacilityEffective date of enrollment:2.Enter Name of Enrollee:Facility Name:OrLast Name: First: Middle:Date of Birth: / /3.Ex: (2012/xx/xx)Gender:MaleFemaleTax Identification InformationSocial Security Number: - -*A copy of the document generated by the IRS that includes your name and SSN must accompany *************************************Federal Tax ID Number: -*A copy of the document generated by the Federal IRS with the name and IRS number must accompanythis application.Legal Name (must be same as denoted on tax ID):Address:City: County: Sta
What requires a CCRI Provider Enrollment Base Application (Long Form) and what requires the CCRI Provider Enrollment Application Short Form? The CCRI short form is exclusive to CCRI and is used for a provider who is currently enrolled, has a valid PROMISe Provider