Transcription
New York StateElectronic Medicaid SystemRemittance Advice Guideline[Type text]Version 2013 - 01[Type text][Type text]7/31/2013
TABLE OF CONTENTSTABLE OF CONTENTS1.Purpose Statement . 42.Remittance Advice Formats . 52.1Electronic HIPAA 835/820 Transaction . 52.2PDF Remittance Advice . 62.3Paper Remittance Advice . 62.3.13.Remittance Sorts . 6Paper/PDF Remittance Advice Sections . 73.1Section One – Medicaid Check. 83.1.1Medicaid Check Stub Field Descriptions . 93.1.2Medicaid Check Field Descriptions . 93.2Section One – EFT Notification . 103.2.13.3EFT Notification Page Field Descriptions . 11Section One – Summout (No Payment) . 123.3.13.4Summout (No Payment) Field Descriptions . 12Section Two – Provider Notification . 133.4.13.5Provider Notification Field Descriptions . 14Section Three – Claim Detail . 153.5.1Child Care Claim Detail . 163.5.2Clinic APG Claim Detail . 243.5.3Claim Detail Page Field Descriptions . 273.5.4Dental Claim Detail. 323.5.5DME Claim Detail . 403.5.6Home Health Claim Detail . 483.5.7Inpatient Claim Detail . 573.5.8Nursing Home Claim Detail . 663.5.9Pharmacy Claim Detail . 753.5.10Practitioner Claim Detail . 833.5.11Transportation Claim Detail . 93REMITTANCE ADVICEVersion 2013 - 017/31/2013Page 2 of 108
CLAIMS SUBMISSION3.63.6.1Financial Transactions . 1013.6.2Accounts Receivable . 1033.74.Section Four – Financial Transactions and Accounts Receivable . 101Section Five – Edit (Error) Description . 105The Status of Claims . 106For eMedNY Billing Guideline questions, please contactthe eMedNY Call Center 1-800-343-9000.REMITTANCE ADVICEVersion 2013 - 017/31/2013Page 3 of 108
PURPOSE STATEMENT1. Purpose StatementThe purpose of this document is to familiarize the provider with the contents of the Remittance Advice.Remittance advices contain the following information:A listing of all claims (identified by several pieces of information as submitted on the claim) that have enteredthe computerized processing system during the corresponding cycleThe status of each claim (deny/paid/pend) after processingThe eMedNY edits (errors) failed by pending or denied claimsSubtotals and grand totals of claims and dollar amountsOther financial information such as recoupments, negative balances, etc.The remittance advice, in addition to showing a record of claim transactions and assisting providers in identifying andcorrecting billing errors, plays an important role in the communication between the provider and the eMedNYContractor for resolving billing or processing issues.REMITTANCE ADVICEVersion 2013 - 017/31/2013Page 4 of 108
PAPER REMITTANCE ADVICE SECTIONS2. Remittance Advice FormatsProviders may receive remittance advice information in one of three formats:The electronic HIPAA 835/820 transactionPDF Remittance AdvicePaper Remittance AdviceRemittance Advices contain a maximum of ten thousand (10,000) claim lines; any overflow will generate a separate 835and a separate check.Providers who submit claims under multiple ETINs will receive a separate remittance advice for each ETIN, regardless ofadvice format.2.1 Electronic HIPAA 835/820 TransactionThe electronic HIPAA 835/820 transaction (Remittance Advice) is available via the eMedNY eXchange or FTP. Forinstitutional providers, retro-adjustment information is also sent in the 835/820 transaction format. Pending claims arelisted in the Supplemental file that is delivered with the 835/820.To request the electronic remittance advice, providers must complete the Electronic Remittance Request Form, which isavailable at www.emedny.org by clicking on the link to the web page as follows: Electronic Remittance Request Form.Providers with only one ETIN receiving an electronic remittance will have the status of any claims submitted via paperforms, state-submitted adjustments/voids and Medicare Crossover claims reported on that electronic remittance. TheDefault Electronic Transmitter Identification Number (ETIN) Selection Form is available on emedny.org by clicking on thelink: Default ETIN Selection Form.Providers with multiple ETINs who receive the 835/820 electronic remittance advice may elect to receive the status ofpaper claim submissions, state-submitted adjustments/voids and Medicare Crossover claims in the 835 format. Therequest must be submitted using the Default ETIN Selection Form which is available at www.emedny.org by clicking onthe link to the web page as follows: Default ETIN Selection Form.Further information on the 835 transaction is available at www.emedny.org by clicking on the link to the web page thatfollows: eMedNY Transaction Information Standard Companion Guide CAQH - CORE CG X12.For additional information, providers may also call the eMedNY Call Center at 800-343-9000.REMITTANCE ADVICEVersion 2013 - 017/31/2013Page 5 of 108
PAPER REMITTANCE ADVICE SECTIONS2.2 PDF Remittance AdviceThe PDF Remittance Advice may be received electronically via the eMedNY eXchange or FTP and may opened withAdobe Reader (6.0 release or higher required). This may be downloaded from www.adobe.com.The PDF itself contains the same layout and fields found in the paper remittance advice that described in section 3below. Additionally, the remittance can be downloaded and stored electronically for ease of retrieval and you can stillprint a hard copy.PDF remittances are not held with the Medicaid check for two weeks but released two weeks earlier.To request the PDF Remittance Advice, providers must complete the PDF Paper Remittance Request Form which isavailable at www.emedny.org by clicking on the link: PDF Paper Remittance Request Form.2.3 Paper Remittance AdviceNote: Paper remittance advices are being phased out.Remittance advices are also available on paper.Providers who bill electronically but do not specifically request to receive the 835 transaction are sent paper remittanceadvices.2.3.1Remittance SortsThe default sort for the paper remittance advice is:Claim Status (denied, paid, pending) – Patient ID – TCNProviders can request other sort patterns that may better suit their accounting systems. The additional sorts availableare as follows:TCN – Claim Status – Patient ID – Date of ServicePatient ID – Claim Status – TCNDate of Service – Claim Status – Patient IDTo request a sort pattern other than the default, providers must complete the Paper Remittance Sort Request Formwhich is available at www.emedny.org by clicking on the link to the web page as follows: Paper Remittance Sort RequestForm.For additional information, providers may also call the eMedNY Call Center at 800-343-9000.REMITTANCE ADVICEVersion 2013 - 017/31/2013Page 6 of 108
PAPER REMITTANCE ADVICE SECTIONS3. Paper/PDF Remittance Advice SectionsThis section presents samples of provider remittance advices, followed by an explanation of theelements contained in the section. Unless otherwise noted, the remittance sections are the same for allprovider types.The information displayed in the remittance advice samples is for illustration purposes only. Thefollowing information applies to a remittance advice with the default sort pattern.The remittance advice is composed of five sections.Section One may contain one of the following documents:Medicaid CheckNotice of Electronic Funds TransferSummout (no claims paid)Section Two: Provider Notification (special messages)Section Three: Claim DetailThe layouts and field descriptions for each of the following remittance types will be described inthis section.Child CareClinic APGDentalDurable Medical Equipment (DME)Home HealthInpatientNursing HomePharmacyPractitionerTransportationSection Four may contain any of the following documents:Financial Transactions (recoupments)Accounts Receivable (cumulative financial information)Section Five: Edit (Error) DescriptionREMITTANCE ADVICEVersion 2013 - 017/31/2013Page 7 of 108
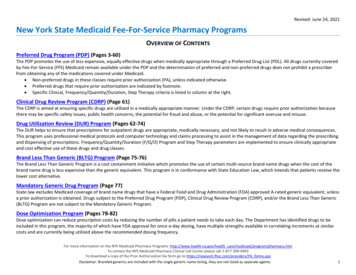
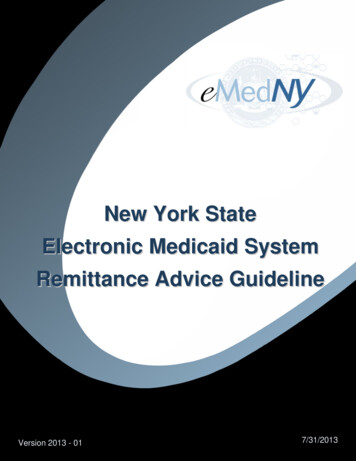
PAPER REMITTANCE ADVICE SECTIONS3.1 Section One – Medicaid CheckThis section contains the check stub and the Medicaid check (payment). A Medicaid check is issuedwhen the provider has claims approved for the cycle and the paid amount is greater than anyrecoupment amounts scheduled for the cycle.Exhibit 3.1-1TO: CITY PHARMACYDATE: 2007-08-06REMITTANCE NO: ############PROV ID: #################################### 2007-08-06CITY PHARMACY111 PARK AVENUEANYTOWNNY11111YOUR CHECK IS BELOW – TO DETACH, TEAR ALONG PERFORATED DASHED LINE292DATEREMITTANCE NUMBER2007-08-06PROVIDER ID NO.DOLLARS/CENTSPAY############################# *****104.88VOID AFTER 90 DAYSTOTHEORDER OFCITY PHARMACY111 PARK AVENUEANYTOWNNY11111MEDICAL ASSISTANCE (TITLE XIX) PROGRAMCHECKS DRAWN ONFIRSTNAME LASTNAMEKEY BANK N.A.60 STATE STREET, ALBANY, NEW YORK 12207AUTHORIZED SIGNATUREREMITTANCE ADVICEVersion 2013 - 017/31/2013Page 8 of 108
PAPER REMITTANCE ADVICE SECTIONS3.1.1Medicaid Check Stub Field DescriptionsUpper Left CornerProvider’s Name (as recorded in the Medicaid files)Upper Right CornerDate the remittance advice was issuedRemittance NumberPROV ID: This field will contain the Medicaid Provider ID and the NPI, when applicableNote: For reissued checks, the original check number will be displayed beneath the PROV ID.CenterMedicaid Provider ID/NPI/DateProvider’s Name/Address3.1.2Medicaid Check Field DescriptionsLeft SideTableDate the check was issuedRemittance NumberProvider ID No.: This field will contain the Medicaid Provider ID and the NPI, when applicableProvider’s Name/AddressRight SideDollar/Check Amount: This amount is the:the Net Total Paid Amount under the Grand Total subsection the total sum of the Financial Transaction section.REMITTANCE ADVICEVersion 2013 - 017/31/2013Page 9 of 108
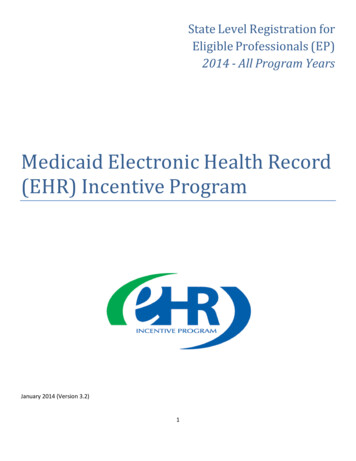
REMITTANCE ADVICE FORMATS3.2 Section One – EFT NotificationThis section indicates the amount of the EFT. An EFT transaction is processed when the provider has claims approvedfor the cycle and the paid amount is greater than any recoupment amounts scheduled for the cycle.Exhibit 3.2-1TO: CITY PHARMACY################## 2007-08-06CITY PHARMACY111 PARK AVENUEANYTOWNNYCITY PHARMACYDATE: 2007-08-06REMITTANCE NO: ############PROV ID: ########/##########11111 104.88PAYMENT IN THE ABOVE AMOUNT WILL BE DEPOSITED VIA AN ELECTRONIC FUNDS TRANSFER.REMITTANCE ADVICEVersion 2013 - 017/31/2013Page 10 of 108
REMITTANCE ADVICE FORMATS3.2.1EFT Notification Page Field DescriptionsUpper Left CornerProvider’s Name (as recorded in the Medicaid files)Upper Right CornerDate: The date on which the remittance advice was issuedRemittance NumberPROV ID: This field contains the Medicaid Provider ID and the NPI, when applicableCenterMedicaid Provider ID/NPI/DateProvider’s Name/AddressProvider’s Name – Amount transferred to the provider’s account.This amount is the:Net Total Paid Amount from the Grand Total subsection the total sum of the Financial Transaction section.REMITTANCE ADVICEVersion 2013 - 017/31/2013Page 11 of 108
REMITTANCE ADVICE FORMATS3.3 Section One – Summout (No Payment)A summout is produced when the provider has no positive total payment. This may happen when the provider hasclaims approved for the cycle and the expected paid amount is less than or equal to any recoupment amounts scheduledfor the cycle.Exhibit 3.3-1TO: ABC PHARMACYDATE: 08/06/2007REMITTANCE NO: ###########PROV ID: ########/##########NO PAYMENT WILL BE RECEIVED THIS CYCLE. SEE REMITTANCE FOR DETAILS.CITY PHARMACY111 PARK AVENUEANYTOWNNY111113.3.1Summout (No Payment) Field DescriptionsUpper Left CornerProvider’s Name (as recorded in the Medicaid files)Upper Right CornerDate the remittance advice was issuedRemittance NumberPROV ID: This field contains the Medicaid Provider ID and the NPI, when applicableCenterNotification that no payment was made for the cycle (no claims were approved)Provider’s Name/AddressREMITTANCE ADVICEVersion 2013 - 017/31/2013Page 12 of 108
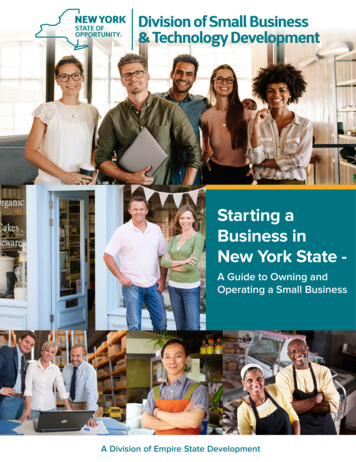
REMITTANCE ADVICE FORMATS3.4 Section Two – Provider NotificationThis section is used to communicate important messages to providers.Exhibit 3.4-1PAGE01DATE08/06/07CYCLE 1563ETIN:CHILD CAREPROV ID: ########REMITTANCE NO: ##########TO: ABC CHILD CARE123 MAIN STREETANYTOWN, NEW YORK 11111REMITTANCE ADVICE MESSAGE TEXT*** ELECTRONIC FUNDS TRANSFER (EFT) FOR PROVIDER PAYMENTS IS NOW AVAILABLE ***PROVIDERS WHO ENROLL IN EFT WILL HAVE THEIR MEDICAID PAYMENTS DIRECTLY DEPOSITEDINTO THEIR CHECKING OR SAVINGS ACCOUNT.THE EFT TRANSACTIONS WILL BE INITIATED ON WEDNESDAYS AND DUE TO NORMAL BANKINGPROCEDURES, THE TRANSFERRED FUNDS MAY NOT BECOME AVAILABLE IN THE PROVIDER’SCHOSEN ACCOUNT FOR UP TO 48 HOURS AFTER TRANSFER. PLEASE CONTACT YOUR BANKINGINSTITUTION REGARDING THE AVAILABILITY OF FUNDS.PLEASE NOTE THAT EFT DOES NOT WAIVE THE TWO-WEEK LAG FOR MEDICAID DISBURSEMENTS.TO ENROLL IN EFT, PROVIDERS MUST COMPLETE AN EFT ENROLLMENT FORM THAT CAN BEFOUND AT WWW.EMEDNY.ORG. CLICK ON PROVIDER ENROLLMENT FORMS WHICH CAN BE FOUNDIN THE FEATURED LINKS SECTION. DETAILED INSTRUCTIONS WILL ALSO BE FOUND THERE.AFTER SENDING THE EFT ENROLLMENT FORM TO EMEDNY, PLEASE ALLOW A MINIMUM TIME OF SIXTO EIGHT WEEKS FOR PROCESSING. DURING THIS PERIOD OF TIME YOU SHOULD REVIEWYOUR BANK STATEMENTS AND LOOK FOR AN EFT TRANSACTION IN THE AMOUNT OF 0.01 WHICH EMEDNYWILL SUBMIT AS A TEST. YOUR FIRST REAL EFT TRANSACTION WILL TAKE PLACE APPROXIMATELYFOUR TO FIVE WEEKS LATER.IF YOU HAVE ANY QUESTIONS ABOUT THE EFT PROCESS, PLEASE CALL THE EMEDNY CALL CENTERAT 1-800-343-9000.NOTICE: THIS COMMUNICATION AND ANY ATTACHMENTS MAY CONTAIN INFORMATION THAT IS PRIVILEGEDAND CONFIDENTIAL UNDER STATE AND FEDERAL LAW AND IS INTENDED ONLY FOR THE USE OF THE SPECIFICINDIVIDUAL(S) TO WHOM IT IS ADDRESSED. THIS INFORMATION MAY ONLY BE USED OR DISCLOSED INACCORDANCE WITH LAW, AND YOU MAY BE SUBJECT TO PENALTIES UNDER LAW FOR IMPROPER USE ORFURTHER DISCLOSURE OF INFORMATION IN THIS COMMUNICATION AND ANY ATTACHMENTS. IF YOU HAVERECEIVED THIS COMMUNICATION IN ERROR, PLEASE IMMEDIATELY NOTIFY NYHIPPADESK@CSRA.COM ORCALL 1-800-541-2831. PROVIDERS WHO DO NOT HAVE ACCESS TO E-MAIL SHOULD CONTACT 1-800-343-9000.REMITTANCE ADVICEVersion 2013 - 017/31/2013Page 13 of 108
PAPER REMITTANCE ADVICE SECTIONS3.4.1Provider Notification Field DescriptionsUpper Left CornerProvider’s Name/Address (as recorded in the Medicaid files)Upper Right CornerRemittance Page NumberDate the remittance advice was issuedCycle Number: The pre-assigned number for the claims processing period. It is helpful to have the cycle numberavailable when calling the eMedNY Call Center with questions about specific processed claims or payments.ETIN (not applicable)Name of Section: PROVIDER NOTIFICATIONPROV ID: This field contains the Medicaid Provider ID and the NPI, when applicableRemittance NumberCenterMessage TextREMITTANCE ADVICEVersion 2013 - 017/31/2013Page 14 of 108
PAPER REMITTANCE ADVICE SECTIONS3.5 Section Three – Claim DetailThis section provides a listing of all claims processed during the specific cycle.There are nine unique Claim Detail types.Child CareDentalDurable Medical Equipment (DME)Home HealthInpatientNursing HomePharmacyPractitionerTransportationREMITTANCE ADVICEVersion 2013 - 017/31/2013Page 15 of 108
PAPER REMITTANCE ADVICE SECTIONS3.5.1Child Care Claim DetailThe Child Care Claim Detail section is used by Child Care provider type.Exhibit 3.5.1-1PAGE02DATE08/06/07CYCLE 1563ETIN:CHILD CAREPROV ID: ########REMITTANCE NO: ##########TO: ABC CHILD CARE123 MAIN STREETANYTOWN, NEW YORK xx-xPATIENTOTHERSERVICE RATE REP’TEDFULL DAYSCALC’EDPARTICIPATION INSURANCEDATESCO-INSURANCEDAYSREPORTEDCODEFROMFC DAYS PAYMENTDEDUCTEDTHRUMM/DD/YY 1210 ####
Providers with multiple ETINs who receive the 835/820 electronic remittance advice may elect to receive the status of paper claim submissions, state-submitted adjustmen