Transcription
Region One Education Service Center2016-17 OPENWhat's New for 2016-17ENROLLMENTEasy EnrollSCAN:Enrollment has just becomeeasier!Avoid typing long URLs andscan directly to yourbenefits websites, videos,and benefits guides.Try it yourself! Scan theBENEFITUPDATESfollowing code in the picture.MedicalTRY MEDentalAccidentand more!www.mybenefitshub.com/region1
INTRO Login and complete your benefit enrollment. Open enrollment is from 7/21/16 to 8/22/16. Medical enroll is passive. If you wish to make changes please complete the TRS Enrollment,Change and Declination Form and submit to Hortencia I. Olivarez by no later than 8/22/16. Supplemental benefits enrollment is mandatory. Supplemental benefits are Accident, CriticalIllness, Dental, Disability, FSA, Heart Stroke, ID Theft, Legalease and Vision.ENROLLMENT DATES: 07/21/16 - 08/21/16www.mybenefitshub.com/region1CALL CENTER #: (800) 583-6908LOGIN INSTRUCTIONSOR SCAN1Go to:2Click Login3www.mybenefitshub.com/region1GOLOGINEnter Username & PasswordAll login credentials have been RESET tothe following defaults:Username:The first six (6) characters of your last name,followed by the first letter of your first name,followed by the last four (4) digits of yourSocial Security Number.If you have six (6) or less characters in yourlast name, use your full last name, followed bythe first letter of your first name, followed bythe last four (4) digits of your Social SecurityNumber.Default Password:Last Name* (lowercase, excluding punctuation)followed by the last four (4) digits of yourSocial Security Number.Supplemental Benefit elections will become effective 9/1/2016. After annual enrollment closes, benefit changes canonly be made if you experience a qualifying event (and changes must be made within 31 days of event).
BENEFITUPDATESAccident Supplemental Benefits by American Public LifeCoverage pays benefit amounts for covered medical expenses as aresult of an accident. Benefits are paid in addition to what yourmedical carrier pays and the money comes to you, not yourmedical provider.with benefits becoming available after the 3rd day of disability, oras late as the 90th day. Benefits are payable to age 65 if disabilityoccurs prior to age 65, and for up to one year at a time if disabilityoccurs after age 65, up to age 70. All new or increases in coverageare subject to pre-existing condition exclusions.Basic Life, Voluntary Life and AD&D Insurance by ONE AMERICABase Life Plan: Region One provides a 25,000 Basic Life withAD&D policy at no cost to the employee.NEW Healthcare & Dependent Care FSA by National BenefitsServicesTax-sheltered flexible spending accounts allow an individual to setaside dollars to pay for future health care and dependent careexpenses. Eligible expenses must be incurred within the plan year.The healthcare reimbursement maximum is 2,550/plan year.The dependent care reimbursement maximum is 5,000 if marriedor 2,500 if single per plan year.Voluntary Term Life: Optional term life is available for theemployee up to 500,000 not to exceed 7 times salary, for spouseup to 100% of the employee amount not to exceed 100,000, andunmarried dependent children to age 26 up to 10,000. AgeReduction applies. Guarantee issue: employee 100,000, spouse 25,000 and child(ren) 10,000. Please see brochure for details.AD&D: Accidental Death & Dismemberment pays you or yourbeneficiary in the event of a dismemberment or death due to anaccident. Employee will be covered for 100% of the electedamount, spouse will be covered for 50% of employee electedamount and child(ren) are covered for 10% of employee electedamount. Age Reduction applies. Please see brochure for details.Cancer Insurance by American Fidelity Assurance CompanyCancer insurance is designed to be a supplement and pays formany costs not covered by your medical insurance. There are 2plan options. Both plans include a diagnostic and preventionscreening once per calendar year. All new or increases incoverage are subject to pre-existing conditions.Critical Illness by AflacCritical Illness plan provides you with a lump sum cash benefit inthe event of a critical illness such as Heart Attack, Stroke, EndStage Renal Failure. See brochure for list of illnesses.NEW Dental Insurance by United HealthCareThe United HealthCare Dental Plan is a PPO Plan that allowsparticipants the freedom to choose any dentist. Diagnostic andPreventitive Services are paid at 100%, Basic Services are paid at80% and Major Services are paid at 50%. Orthodontics coveredonly for children to age 19, with a 1,000 lifetime maximum.Deductibles are 50 per person, 150 per family.Disability Insurance by The StandardPlan provides a monthly income to an individual that is disableddue to an accident or illness. There are 4 different plans availableIt’s Important to Save Your Receipts! The IRS requires the FlexCard be used for eligible expenses only. Most of the time we canverify the eligibility of the expense automatically. Yet, there areinstances when you’ll receive a letter asking you to furnish anitemized receipt to verify the expense.Heart Stroke Insurance by Bay Bridge AdministratorsHeart Stroke plan is designed to supplement medical coverage inthe event of a Heart Attack, Heart Disease or Stroke. Pre-Existingconditions apply. Please see brochure for details.Identity Theft and LegalGuard by LEGALEASEID Monitoring offers consumers a comprehensive and proactivedefense against identity theft.LegalGuard helps you find the right type of attorney when a needarises. LegalGuard has the experience and relationships with theirnetwork providers to match you to the type of attorney you needin the right location, with availability to set up a consultation.make things less stressful.Medical Insurance by TRS ActiveCare Aetna and Allegian HealthPlanMedical is a passive enrollment for 2016-17 plan year.TRS ActiveCare Medical Plan Options for 2016-2017 areActiveCare 1-HD, ActiveCare Select, ActiveCare 2 and AllegianHealth Plans. Please see plan detail atwww.mybenefitshub.com/region1NEW Vision Insurance by United HealthCareUnited HealthCare is offering two Vision Plans. Both plans haveexam co-pays. High option has not materials copay where as lowplan has a 25 co-pay. See brochure for full details.Caller Center Informa onNumber: (800) 583-6908Hours: Monday - Friday, 7:30 A.M - 5:00 P.Mwww.mybenefitshub.com/region1
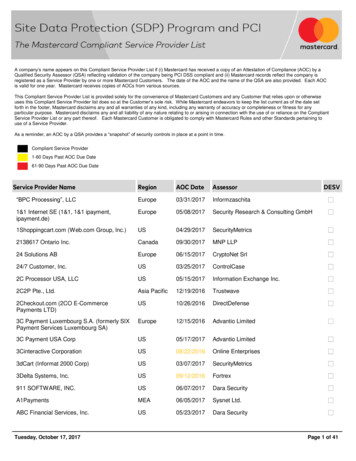
Enrollment, Change and Declination FormELIGIBILTY:Are you an active employee and making monthly contributions to TRS? YesIf no, are you regularly scheduled to work 10 or more hours per week? Yes(If no to both, you are noteligible for TRS ActiveCarecoverage)- No NoSECTION 1: ENROLLMENT/CHANGE TRANSACTION TYPE Annual Enrollment New Employee Add Dependent Special EnrollmentFor District Use Only For New Employee (check one): Effective on Actively at Work Effective 1st day of month followingTRS District #Actively at Work Date:Special Enrollment Event Date: / /Change Only: Marriage Name AddressEffective Date of Change/CancelSECTION 2: EMPLOYEE INFORMATIONLast Name: Other:Cancel Employee Death Loss of Eligibility Retirement/Terminated Non-Payment Other:/ /Effective/Change Date: Birth/Adoption Loss of CoverageDecline Coverage: Yes (Complete Section 6) N/A Plan/Coverage Court OrderCancel Dependent Divorce Death Loss of Eligibility Dropped Coverage Other:First Name:MI:Mailing Address:Home Phone Number:Cell Phone Number:Sex: M FDate of Birth:Were you covered by anotherdistrict? Yes NoIf so, which:Social Security #:City:City:Residence Address:Employer Approval:State:Zip:State:Zip:Email:Language: English SpanishEthnicity:Do you have a disability affecting your ability to communicate or read? Yes (Please complete Section 8) NoCity:Isthe Employee Covered By Other Insurance? Yes Carrier/Plan: NoState:CellPhoneNumber:Is the Employee Covered by Medicare? Yes Part A Part B Part C Part D Effective: NoZip:HomeEmail:Sex: M FLanguage: OtherReason for Medicare Coverage: Entitlement Age Disability End Stage Renal Disease (ESRD)Ethnicity:3: COVERAGE SELECTION (Please select a Plan of Coverage – Plan or HMO - and Coverage Type)SECTIONPlan Selection: ActiveCare 1-HD ActiveCare Select ActiveCare 2HMO Selection: FirstCare Health Plans Scott & White Health Plan Allegian Health Plans (formerly Valley Baptist Health Plans)Coverage Type Selected: Employee Only Employee Spouse Employee Child(ren) Employee FamilySECTION 4: DEPENDENT INFORMATION (Use additional form for additional dependents)SPOUSE Last Name:Street Address:City:Sex: M FFirst Name:State:Zip:Date of Birth: Stepchild No Medicare: Part AFirst Name: Foster ChildStreet Address:City: Grandchild Legal Guardian Part B Disabled Part C Part DMI: Other Phone Number: Same as EmployeeState:Social Security #:Date of Birth:Other Insurance: Yes. Carrier/PlanCHILD Last Name: Natural/AdoptedPhone Number:Social Security #:Other Insurance: Yes. Carrier/PlanCHILD Last Name: Natural/AdoptedStreet Address:City:MI: Same as Employee Stepchild Foster ChildZip Code:Phone Number:Sex: M F No Medicare: Part A Part BFirst Name: Grandchild Legal Guardian Disabled Part C Part DMI: OtherPhone Same as EmployeeState:Social Security #:Date of Birth:Other Insurance: Yes. Carrier/PlanZip Code:Phone Number:Sex: M F No Medicare: Part A Part BPLEASE CONTINUE ON NEXT PAGE Part C Part D
CHILD Last Name: Natural/AdoptedFirst Name: Stepchild Foster ChildMI: Grandchild Legal Guardian Disabled Other Same as EmployeeStreet Address:City:State:Date of Birth:Zip Code:Phone Number:Sex: M FSocial Security #:Other Insurance: Yes. Carrier/PlanCHILD Last Name: Natural/Adopted Stepchild No Medicare: Part AFirst Name: Foster Child Grandchild Part B Part C Part DMI: Legal Guardian Disabled Other Same as EmployeeStreet Address:City:Date of Birth:State:Social Security #:Other Insurance: Yes. Carrier/PlanSECTION 5: DISABLED DEPENDENTS OVER AGE 26Zip Code: NoPhone Number:Sex: M F: Medicare: Part A Part B Part C Part D Request for Continuation of Coverage for Handicapped Child form and Attending Physician’s StatementPlease note that a Request for Continuation of Coverage for Handicapped Child form and Attending Physician’s Statement are required for coverage of a disabled child overage 26. See your Benefits Administrator for the forms, which must be completed in full and submitted to your Benefits Administrator.SECTION 6: DECLINATION OF COVERAGEThis is to certify that the available coverage has been explained to me. I have been given the opportunity to apply for the coverage available to me and mydependents and have voluntarily elected to decline the coverage as elected me:Gender:Name:FGender:FMFSSN:Date of Birth:SSN:Date of Birth:SSN:Date of Birth:MSSN:Date of Birth:MSSN:Date of Birth:Name:Gender:SSN:Date of Birth: EmployeeReason: Other Coverage Other: SpouseReason: Other Coverage Other: ChildReason: Other Coverage Other: ChildReason: Other Coverage Other: ChildReason: Other Coverage Other:Address:same as employeeAddress:same as employeeAddress:same as employeeAddress:same as employeeAddress:same as employee ChildAddress:Reason: Other Coverage Other:same as employeeSECTION 7: COVERAGE CONDITIONS I am employed by the Employer named in this Enrollment Application and Change Form. I am eligible to participate in the coverage(s) offered by theTRS-ActiveCare program which is administered by Aetna, with HMO benefits provided by SHA, L.L.C. dba FirstCare Health Plan, Scott and WhiteHealth Plan, and Allegian Insurance Company dba Allegian Health Plans. On behalf of myself and any dependents listed on their EnrollmentApplication and Change Form, I apply for those coverage(s) for which I am eligible.o If I am enrolling a grandchild in Section 4, I certify that my household is the grandchild’s primary residence and the grandchild is my dependentfor federal income tax purposes for the reporting year in which coverage of the grandchild is in effect.o If I am enrolling a child as an “other Child” in Section 4, I certify that my household is the child’s primary residence, that I provide at least 50% ofthe child support, that neither of the children’s natural parents reside in my household, and that I have the legal right to make decisionsregarding the child’s medical care. Only those coverage(s) and amount for which I am eligible will be available to me. I understand that if this Enrollment Application and Change Formis accepted, the coverage(s) will become effective in accordance with the provisions or the TRS-ActiveCare program. I understand that by enrolling for coverage with Employer named in the Enrollment Application and Change Form that any TRS-ActiveCarecoverage I previously elected under another TRS-ActiveCare participating district/entity will be terminated under TRS Rules. I authorize necessary payroll deduction by my Employer, if any, to cover the cost of my coverage(s). I agree that my Employer acts as my agent.All notices given to my Employer are binding upon me. I also agree that my participation in the coverage(s) is subject to any future amendments. I understand that by declining TRS-ActiveCare coverage now or by terminating TRS-ActiveCare coverage during the plan year, I am not eligible tore-enroll in TRS-ActiveCare until the next plan year, unless I experience a special enrollment event. I state that the information given on the Enrollment Application and Change Form is true and correct. I understand and agree that anyincorrect statements material to the risk and knowingly made by me will invalidate my coverage(s).Applicant Signature: Date:SECTION 8: SPECIAL NOTES REGARDING MY ENROLLMENT (Please indicate any special information regarding my enrollment for Aetna, Caremark ormy selected HMO)
Medical Insurance by TRS Activeare Aetna and Allegian Health Plan Medical is a passive enrollment for 2016-17 plan year. . Health Plan, and Allegian Insurance Company dba Allegian Health Plans. On behal