Transcription
SystemleadershipLessons and learning fromAQuA’s Integrated CareDiscovery CommunitiesAuthorsDavid FillinghamBelinda WeirOctober 2014
System leadership12345678Contents1Introduction32The AQuA Integrated Care Discovery Communities53The characteristics of effective system leaders114The current state of leadership in health and social care145Developing the system leaders of the future16‘Micro level’ – team and locality18‘Meso level’ – services and patient pathways19‘Macro level’ – whole system19What does the AQuA Leading Integrated System-Level ChangeProgramme do?20A case study: Manchester’s ‘Living Longer Living Better’programme24Context24Progress to date26The evolution of new leadership roles27Supported learning and development28Reframed governance arrangements29Reflections306Contents 1
System phy38References40About the authors43Acknowledgements44Contents 2
System leadership112345678IntroductionAcross the world health care systems are under pressure. Policy-makers and healthand social care leaders are individually and collectively searching for approachesthat can deliver better-quality, safer care and improved health at a reduced cost –the holy grail of health strategy. We have to rethink the way care is delivered, andimproved co-ordination around the needs of the individual will almost certainly bepart of the solution.In England a cross-party consensus is forming around the concept of ‘integratedcare’ approaches as the best hope for a sustainable NHS in the future (Goodwinet al 2013). There is general agreement that the goal involves more joining-up ofservices around the needs of individual patients and citizens. However, there isless agreement, and scant real evidence, about the best means of achieving this.The challenge to leaders in the health care system presented by this aspiration isimmense as there are unlikely to be any ready-made formulae that can be easilyapplied. Leading across complex interdependent systems of care is a new anddifferent role that needs to be undertaken alongside the already difficult task ofleading successful institutions.We believe that enough has been written to make the case for the need for a new styleof leadership across health and social care systems (Ham and Walsh 2013; Goldsmith nodate). The task now is to identify the skills, knowledge and behaviours that this newbreed of system leaders will need if they are to be successful and to consider howsuch an approach to developing leadership – which is likely to be different to thatfound inside many of our institutions – can best be fostered.This paper: describes the work carried out by AQuA (the Advancing Quality Alliance)and The King’s Fund in the north-west of England between 2011 and 2014,which has taken a ‘discovery’ approach to developing integrated care and theleadership capabilities to support itIntroduction 3
System leadership12345678 considers why the style of leadership currently dominant in much of healthand social care does not lend itself well to leading across complex integratednetworks and the implications for developing system leaders sets out in general what we have learned about the skills, knowledge andbehaviours displayed by the most effective ‘system leaders’ and systemleadership teams explores in more detail the learning from an in-depth case study in relation toone particular community – the City of Manchester concludes with reflections on this work for those interested in the developmentof the system leaders of the future.Introduction 4
System leadership12345678The AQuA IntegratedCare DiscoveryCommunities2If it is true that ‘the system is perfectly designed to get the results it gets’ we will needto redesign the system that produces and develops health care leaders if we wantthem to think and act differently (Batalden 2008).This section of our paper describes the learning emerging from work over thepast three years in the north-west of England with this assumption as its guidingprinciple. Since 2011 AQuA and The King’s Fund have worked in partnership tosupport a new form of learning and development – an Integrated Care DiscoveryCommunity. The aim has been to accelerate the development of effective integratedcare systems, while at the same time helping to grow a new cadre of system-levelleaders (OPM 2014). Nineteen health and social care economies have come togetherto share insights and learning.AQuA is unusual in the NHS in that it is a membership-funded improvementagency working at regional level hosted by a foundation trust. AQuA has 72 NHSorganisations in membership drawn equally from commissioners and every sectorof providers. One of the organisation’s core aims is to support members to join upservices around patients in order to achieve improved health, better quality of careand better value for taxpayers’ money.From the outset of this work, both AQuA and The King’s Fund believed that atraditional leadership development approach would not be best suited to thisparticularly complex challenge. We recognised that the members of the DiscoveryCommunities were at different stages in their progress towards integrated services,operating in different geographical, organisational and relational contexts. Theirlearning needs were not fully understood, although we observed a preferencefor technical tasks and skills-based training. This is not surprising: it fits with aThe AQuA Integrated Care Discovery Communities 5
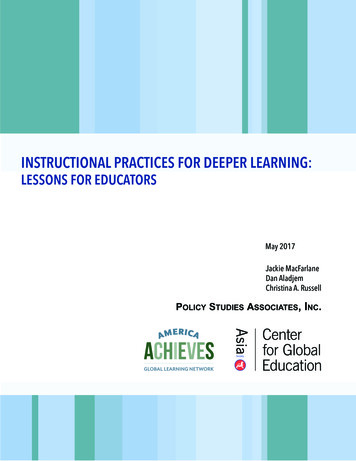
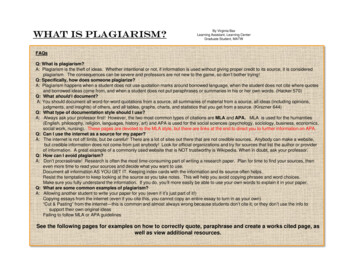
System leadership12345678common preconception of training and development and often feels safer. One ofour challenges was rapidly to build trust and safety in the communities so that theycould also work on leadership behaviours and group development.It was clear that a standard one-size-fits-all development programme wouldnot deliver the outcomes the Discovery Communities aspired towards. Insteadour strategy was to develop and support learning communities founded on theprinciples of learning in complex adaptive systems.Learning in a complex adaptive system Learning needs emerge and change Inter-organisational and inter-professional teams are critical to successful change What works is context specific so local organisation and health economies will needto adapt not just adopt A successful change will require attention to technical aspects (‘the anatomy’) andcultural aspects (‘the physiology’).(Zimmerman et al 1998)Over the three years since the Integrated Care Discovery Community was createdmembers have worked together in a variety of ways to test out ideas and todevelop new knowledge, skills and behaviours. While there has been input fromrecognised national and international experts on integrated care, there has alsobeen a continued and strong emphasis on the rapid testing and implementation oflearning in local communities. Figure 1 opposite sets out the key aspects of how theIntegrated Care Discovery Communities have operated.The AQuA Integrated Care Discovery Communities 6
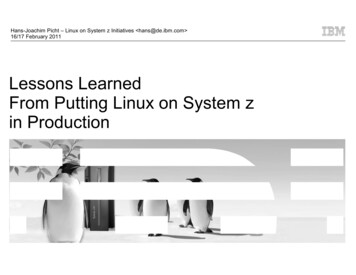
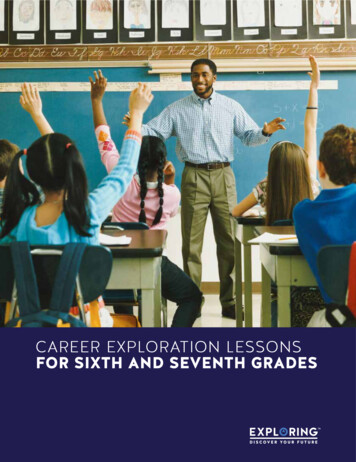
System leadership12345678Figure 1 How the Integrated Care Discovery Communities operate Technical workshopsand WebExs Engagement events andtechnical workshops Access to thought leadersand international experts Executive and team coaching Faculty and expert support Action learning sources AQuA’s integration systemframework and tool Measurement guideand guide forkey domain enablers Access to AQuA’smember portal Case studies from thenorth-west andinternational evidence PublicationsFeedback from community members endorsed the AQuA Integration SystemFramework (see Figure 2 overleaf) and Assessment Tool (see Figure 3, p 9) as beingparticularly helpful interventions. The framework was developed from observationsthat many organisations and communities found themselves struggling to knowwhere to begin. The Discovery Community therefore created an eight-domainframework to provide some structure and starting points to tackle the barriers tointegrated care at system level. The framework has been developed, tested, adapted,refined, implemented and evaluated over the past three years, and that processcontinues as new knowledge emerges, and as communities adapt the framework tosuit local needs. Currently it serves as a way of focusing the community teams on allthe elements that we understand impact on the delivery of integrated care services.The AQuA Integrated Care Discovery Communities 7
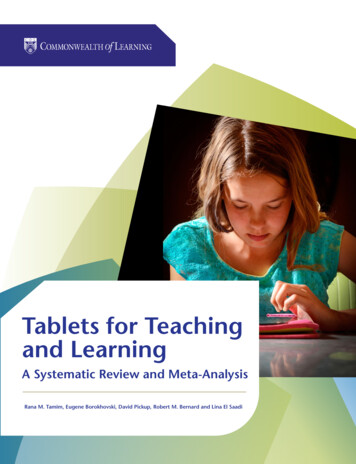
System leadership12345678Figure 2 AQuA’s Integration System FrameworkService andcare model designWorkforce Role design SkillsLeadership CapacityIntegration to improve SafetyService user andcarer engagement Experience EffectivenessHealth carevalueInformation andinformation technology Population health Use of resourcesFinancialand contractualmechanismsCultureGovernanceThere is much valuable learning in relation to each of these domains. Some ofthem are harder-edged – representing what Zimmerman describes as the anatomyof integrated services. These include work on service and workforce redesign,infrastructure and IT, and finance and contractual mechanisms. Others are softer(though not easier!) and represent the physiology of the integrated system: theyinclude work on leadership, patient and carer engagement, governance and culture.The Integrated Care Framework Assessment Tool has enabled health economies toassess their current level of readiness in relation to the introduction of integratedcare approaches. It has also given them focus as they have planned actions forimprovement and measured progress over time across the key enablers.The AQuA Integrated Care Discovery Communities 8
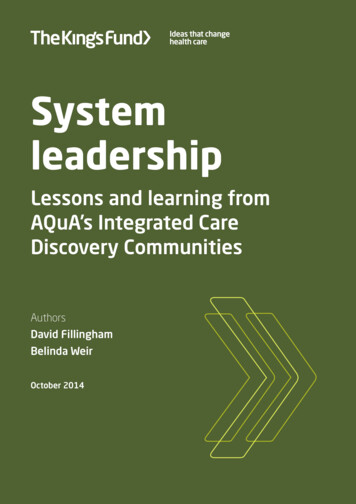
System leadership12345678Figure 3 AQuA’s Integrated Care Framework Assessment ToolLeadership5This informs:Serviceredesign economy action plans4 how the programmeof support is shapedGovernance3 development of theframework and tool.21WorkforceCulture0Informationand ITService user andcarer engagementFinancial andcontractual mechanismsApril 2012October 2012May lture2.332.742.83Service user and carer engagement1.252.002.21Financial and contractual mechanisms2.082.212.79Information and IT2.082.032.27Workforce1.882.031.83Service redesign1.541.841.88Note: The Integrated Care Framework Assessment Tool asks participants to score themselves on a rangefrom a 0 (low) to 5 (high) on their self-assessed capability level across each of the eight domains. Theyare guided in this by a series of definition statements for each level for each domain. The scoring shownwas carried out in Salford during a period of just over a year but it is typical of the patterns generatedby teams within communities. The value of the tool lies in generating debate among partners, creatinga shared awareness of strengths and weaknesses, and helping to develop jointly owned action plans.The AQuA Integrated Care Discovery Communities 9
System leadership12345678An excellent example of this is to be found in the community of Salford. HereSalford clinical commissioning group (CCG), Salford Royal NHS Foundation Trustand Salford City Council have been working together to develop an integrated careprogramme to meet the needs of a fictional but typical resident – Sally Ford – andher family. Similar approaches have of course been adopted earlier and successfullyin Torbay (Mrs Smith), Jonkoping (Esther) and elsewhere. While these all use thedevice of a person as a means of engaging communities and stakeholders aroundindividual needs, it is worth noting that Sally Ford is from Salford. She speaks witha Salford accent, lives in a Salford street, travels on Salford trams. This then is anexample of adaptation as much as of adopting good practice from elsewhere, and itreflects Zimmerman’s notion that improvement approaches must be context-specific.Leaders in the Salford community used the AQuA framework at six-monthintervals to self-diagnose progress and areas in need of attention. They encouragedteams at different levels in each of the partner organisations to use the frameworkand through this process gained insights by comparing the results. This activityhas in itself been an important leadership development intervention: exchanginginformation, testing assumptions and coming together to develop a sharedunderstanding of need and strength across the community partners has helpedleaders to break down barriers and forge new relationships.The AQuA Integrated Care Discovery Communities 10
System leadership12345678The characteristics ofeffective system leaders3The NHS and local government have many highly experienced, capable and skilledleaders. They have risen to leadership positions in complex, politically chargedenvironments and are battle-hardened from their experiences of seeking to improvequality in ever-more challenging economic times. So why is it so difficult for theseleaders to shift their focus to deliver more co-ordinated approaches? The DiscoveryCommunity has attempted to answer this question by drawing on lessons fromoutside the health and social care system.There is a fascinating literature on the differences in nature between markets,hierarchies and networks, illustrated by Walter Powell’s summary shown in Table 1.Table 1 Learning from other sectors: markets, hierarchies, networksKey featuresMarketHierarchyNetworkNormative basisContractsEmployment relationshipComplementary strengthsMeans ofcommunicationPricesRoutines and rulesRelationshipsConflict resolutionHaggling/litigationAdministrative edictReciprocity seekingwin/winCommitment amongthe partiesLowMedium to highHighTone or climateSuspicionFormal bureaucraticOpen-ended dentSource: Adapted from Powell (1990)The characteristics of effective system leaders 11
System leadership12345678Using Powell’s model we would suggest that the NHS in England maintainsall the characteristics of a hierarchy. Although arguably versions of an internalmarket have existed since 1989, the predominant culture is still one of directionor regulation from above. Foundation trusts are ostensibly independent but areheavily regulated and many senior leaders feel themselves to be in a hierarchicalrelationship with Monitor. For NHS trusts this is even more clearly the case interms of their relationship with the NHS Trust Development Authority. Sir DavidNicholson’s exhortation for leaders to look ‘outwards not upwards!’ is not in realitythe dominant leadership strategy within the NHS (Thompson et al 1991).Why is that a problem? After all, routines and rules that support regulation,monitoring and compliance with safety and performance targets are undeniablyimportant. But if hierarchies are useful for many things, they are not the mosteffective structures for co-ordinating products and services across complexinterdependent networks. In other sectors there has been a growing trend towardsdifferent forms of social and economic organisation. This is apparent in fields asdiverse as textiles, finance, telecommunications and the media and film industries(Tam 1994). These new organisational forms lie part-way between traditionalcorporate hierarchies and free markets. They have been characterised in a varietyof different ways – as strategic alliances (Jarillo 1988), dynamic networks (Milesand Snow 1986), or value-adding partnerships (Johnston and Lawrence 1988).In the commercial world new forms of leadership have emerged to support thesedynamic networks. These leaders display a new set of attributes that are differentfrom the ones that helped them successfully climb the corporate ladder (MossKanter 1985). They must: learn to operate without the might of the hierarchy behind them and use theirindividual skills rather than their formal position to achieve results be able to compete in a way that enhances rather than undercuts thecompetition – to do this these leaders must become successful collaborators conduct their business to the highest ethical standards; trust is crucial tosuccessful alliance-building develop a process focus – concentrating not only on what is to be achievedbut how.The characteristics of effective system leaders 12
System leadership12345678Such networks are consciously managed by entrepreneurs who use collaborativeapproaches to pursue their institutional objectives. What lessons are there in thisfor the NHS? Even the guru of private sector competitiveness, Michael Porter, hasrecognised that to deliver improved value (increased quality at lower cost) there isa need for health care organisations to co-operate together across the whole valuecycle of care delivery. Porter’s argument is that ‘accountability for value should beshared amongst the providers involved’ rather than ‘focussed factories concentratingon narrow groups of interventions, we need integrated practice units accountablefor total care’ (Porter and Teisberg 2006).In its next stage of evolution, health care needs to operate much more effectivelythrough dispersed networks rather than through top-heavy hierarchies.In the next section we consider how far the NHS exhibits the type of collaborativeleadership now seen in some commercial settings.The characteristics of effective system leaders 13
System leadership12345678The current state ofleadership in health andsocial care4A seminal King’s Fund report on health care leadership in 2011 observed that aleadership model holds sway within the NHS based on the idea of the single heroicindividual (The King’s Fund 2011). Such a model has been fostered in part by thedominant political and clinical role models within the service. The heroic leadershipstyle suited the goals of capacity-building and target delivery within institutionalsilos as the NHS sought to reduce long wait times during the 2000s.It comes as little surprise that a deeper analysis of almost 1,000 top health careleaders found that 80 per cent had ‘pacesetting’ as a favoured style. Pacesettersare good at driving up performance on a narrow range of goals within a singleorganisation (The King’s Fund 2012), but the characteristics of pacesetting are a longway removed from those displayed by effective leaders of dynamic networks in thecommercial world.As Ham and Hopson make clear, ‘the skills required to lead different organisationalmodels are often different from those required to run a successful single institution’(The King’s Fund and Foundation Trust Network 2014, pp 3–6).Indeed, the pacesetting style identified as predominant among top NHS leaders isin many ways antithetical to the leadership requirements for effective integratedcare services. Pacesetting leaders ‘know’ what is required, and waste little timeasking questions, since uncertainty may be perceived as a weakness and sharedunderstanding takes time to achieve. But in complex adaptive systems there is muchthat is unknown: uncertainty and ambiguity are the modus operandi for leaders.While decision-making across organisational boundaries and traditional governancestructures is a lengthy and often frustrating process, the lack of shared goals, ofThe current state of leadership in health and social care 14
System leadership12345678collective understanding of the issues and of the opportunity to hear from manyvoices means that system-level plans fail, too often, to deliver system-level change.Based on our experience of working in-depth with such leaders over the past threeyears, curiosity, connectivity and coaching capability seem to be far more significanttraits of effective leadership in the current health and social care environment. Thisis explored in more detail in Chapter 6 in relation to the specific example of theCity of Manchester.This analysis is not exclusive to the health sector. Archie Brown, in The myth of thestrong leader (2014), describes the sub-optimal perception of the role of the headof an organisation as ‘the leader as boss’, described in earlier work by Pe
support a new form of learning and development – an Integrated Care Discovery Community. The aim has been to accelerate the development of effective integrated care systems, while at the same time helping to grow a new cadre of system-level leaders (OPM 2014). Nin