Transcription
ciclinical impressions PAGE 4DR. ALAN BAGDENA Conversation withDr. Larry WhitePAGE 14DR. MICHAEL SWARTZBonding Agent Bond StrengthPAGE 21DR. DAVID SARVERDiagnosis andTreatment PlanningPAGE 27DR. ROBERT WAUGHOptimizing Bond RetentionPAGE 31DR. STEPHEN TRACEYPatient SurveysPAGE 33DR. MORRIS STRAUSSReducing Wire PokesDR. ALAN BAGDENVOL 14NO 12005
LETTEREDITOR’S COLUMNVOL 14 NO 1 2005In Pursuit of ExcellenceDear Doctors,I am honored to announce thatDr. Larry White has taken the helmof Clinical Impressions as its editor.With over 45 years in the profession,Dr. White offers a unique combination of skills and experience that willserve you well in providing practicalways for improving the quality ofyour treatment and overall practice life.Perhaps best known as the esteemed editor of theJournal of Clinical Orthodontics for 17 years, Dr. White hasmany professional accomplishments. He is a diplomate ofthe American Board of Orthodontists and a fellow in theAmerican College of Dentists. He is past president of theRocky Mountain Society of Orthodontists, the NewMexico Orthodontic Society and the Texas Tweed StudyGroup. He serves as manuscript reviewer for the AmericanJournal of Orthodontics, is technology and new producteditor for the World Journal of Orthodontics, a contributing editor for the Orthodontic CyberJournal, and editor ofthe Dallas County Dental Society publication, Dateline. Aseditor of The Rocky Mountain Orthodontic Newsletter,Dr. White received the International College of DentistsGolden Scroll Award for the most improved dental journalin dental literature.Dr. White has contributed more than 100 original articles to dental literature and has presented lectures toorthodontic societies, universities and study clubs in over35 countries. He was the first director of the University ofTexas Health Science Center in San Antonio OrthodonticResidency Program. He currently practices orthodontics inDeSoto, Texas. So welcome, Larry. We know that with yourrecord of achievement, Clinical Impressions will continue tothrive under your able guidance.Best regards,Dan EvenPresident, Ormco CorporationCover: Photo DavidHills.netLarry W. White, DMD, MSDEditor, Clinical ImpressionsDallas, TexasAny advantage I bring to editing an orthodonticmanufacturer’s journal owes itself to my dailyengagement in clinical practice where I see theresults of diagnosis, treatment planning andtherapy. As I transitioned from private practiceto academic life and back to a private setting, Ihave had an unusual opportunity over the past sixyears to work with and for several orthodontists.I have concluded that, without exception, we allface the same problems; e.g., difficulty of correcting saggital discrepancies, changing the behaviorof noncompliant patients, eliminating bond failures, placating unreasonable parents and satisfying unhappy employees. As a famous politicianonce said, “I feel your pain.”I intend to rely on this shared experience as Iseek articles and clinical pearls that will reducethe frustrations, satisfy the needs, and fulfill theaspirations of clinicians who simply want to dotheir work better. You can help me with your feedback because that offers the only evidence ofwhether Clinical Impressions is performingaccording to its purpose.Many years ago, W. Edwards Deming developed the concept of Total Quality Control thatemphasized the delivery of consistently excellentgoods and services by implementing his 14Points. More than any other person, Deming isresponsible for the emergence of Japan as anindustrial colossus renowned for her excellentproducts. By the time I got around to taking hisseminars, Dr. Deming was 92, but he still hadplenty of energy and enthusiasm for the subjectof quality and how to achieve it consistently. We
no longer hear as much about Deming’s 14Points, mainly because they have become such apart of the DNA of successful companies, they nolonger require special courses. A few of thosepoints have particular relevance and form thebasis of his specific philosophy. I would like toshare them with you.1. Quality is defined by the customer. Demingsaid, “A satisfied customer is not enough. Business is built on the loyal customer, one who comesback and brings a friend.” Ultimately, managementmust anticipate whole new product categories thecustomer has never contemplated. For Ormco, thatmeans envisioning, developing and marketing systems that will benefit orthodontists even thoughthey haven’t yet asked for them.Deming would repeatedly remind audiencesthat the average customer has never led anadvance in the production of any good or service.No customer asked for electricity, the automobile,the camera, pneumatic tires, or the copyingmachine (or even the preadjusted orthodonticappliance). Real improvements must come frominnovators working hand-in-glove with companiesas committed as they are to improving productsand services that customers will eagerly endorse.2. Understand and reduce variation in everyprocess. Deming considered variation the primeenemy of quality and felt that predictability wasthe cardinal virtue of any process. Mixing systemsand brackets because of price advantage onlyincreases variation and mitigates against consistent quality. Deming felt price had no meaningwithout a measure of the quality being purchased.Orthodontists who continually look for companiesthat will compete for their business on price alonewill often find themselves at cross purposes withthe production of excellent treatment. They woulddo well to work closely with companies they trustto deliver innovative and quality products and forget about the pennies they might save with acheaper product.3. Change and improvement must be continualand all-encompassing and involve everyone; i.e.,employees, management and outside suppliers.The Japanese word for such a concept is kaizen.Deming often said that time alone will bringchange, but continual improvement for every strategy, product and process in an organization has tohave the active commitment of everyone. Thispremise has special relevance for orthodontistsbecause although they can control themselves andtheir office personnel to some extent, they mustdepend entirely on orthodontic manufacturers forthe instruments and systems they employ.Ormco has committed itself to seeking alignments with the most innovative orthodontists inthe world to bring clinicians and their patientsproducts and services that can consistently produce excellent results. They make training in thesesystems readily available and easily obtainable bysponsoring seminars all over the world. As orthodontists seek to deliver consistently excellenttherapy to their patients, they realize the needfor a partnership with a company that shares thatcommitment. Ormco intends to be that kind ofcompany for those doctors who seek the best.In Memoriam: Dr. Ronald H. RothDr. Ron Roth, world-renowned orthodonticeducator and clinician, died January 23, 2005.Dr. Roth served as adjunct and clinical professorof orthodontics at several universities and wasa founder and director of the Roth/WilliamsCenter for Functional Occlusion.Dr. Roth’s passion for uniting facial esthetics,mechanics and function into a diagnostic regimen will remain his lasting legacy and serve as inspiration for those who now pick up thetorch he lighted with his sagacity and curiosity. We wish to recognizeDr. Roth’s numerous contributions to the orthodontic profession andextend our deepest condolences to his family and loved ones.3
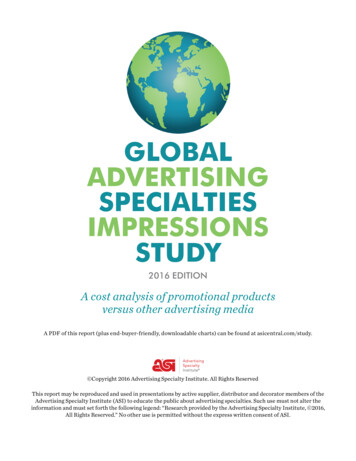
A ConversationTHE DAMON SYSTEM: QUESTIONS AND ANSWERSAlan Bagden, DMDSpringfield, VirginiaDr. Alan Bagden has been involved with the development of Damon System protocolssince 2000, is coauthor of the Damon Workbook and has lectured extensively addressinggroups of doctors in seminars in the U.S. and abroad. Clinicians using the System, as wellas those contemplating its use, appreciate the insights to treatment mechanics he offers.From these presentations Dr. Larry White drew the questions for this interview.Dr. Alan Bagden has been inthe private practice of orthodontics in Northern Virginiafor the past 20 years. As anadvocate of economical andefficient clinical treatment, hehas been a frequent contibutor to Clinical Impressionsand, as a result, has becomeactively invoved in the development of the DamonSystem. Together with Dr.Damon he has edited theDamon System Workbookand has delivered DamonSystem lectures throughoutNorth and South America,Europe, Asia and Australia.He is currently involved innumerous clinical studiesconcerning the DamonSystem and shares some ofhis particular insights into thefine points of the System.Dr. White: Alan, what first prompted you to consider employing the Damon System?Dr. Bagden: When I first saw Dwight Damon'streated case photos, I thought they were too good tobe true. I was skeptical whether it was really possibleto treat patients so quickly, with so few extractionsand without rapid palatal expanders. Eager to compare results from the Damon System with traditionalbrackets, I performed a tightly controlled split-mouthstudy of ten individuals with Damon brackets on oneside of the mouth and traditional brackets on theother. What I found completely dispelled my skepticism. The Damon side moved teeth twice as fast as thetraditional side. I decided to immerse myself witheverything I could to learn more about the System,and to begin using the system on more and morepatients. Within a few months, the results I saw formyself made my decision clear. This is a better way todo orthodontics.2a4Dr. White: You were using a conventional .018 slotbracket before converting to the Damon System,which at the time came only in an .022 slot. I’mcurious about the reason you didn’t switch to theDamon .018 when it became available.Dr. Bagden: Initial tooth movement in the DamonSystem is accomplished with small, light wires. I likethis philosophy and, in fact, have always been an advocate of light forces. For some reason, however, I hadbought into the idea that forces delivered through asmall slot would be lower than those deliveredthrough a larger one. Upon closer analysis, I learnedthat this is not the case. Less force is delivered withless binding and friction in an .022 slot than in an.018 slot. In a passive system, the wire-to-lumen ratiois key. And with the reduced friction and bindingthat results from the large lumen-to-wire ratio, teethlevel and align with far more efficiency and muchless force than conventionally ligated brackets. The2b2cFigures 2a-g. The posterior transverse arch adaptation fostered by the Damon System occurs without the use of or need for heavy-forcemidface is dramatic. Smiles are broader, midfaces are fuller and esthetics are ultimately improved.
System is not forcing teeth into new positions, butrather allowing for a more-naturally fostered physiological adaptation.Dr. White: So it is the light-force philosophy thatdictates the recommended protocol for starting caseswith an .014 round Copper Ni-Ti wire, right?Dr. Bagden: Yes, the Damon System philosophy ispredicated on light forces and minimal friction andbinding. To initiate physiologically determined toothmovement, it is essential to start each case with lightbiologically sensible forces. Nothing larger than an.014 round Damon Copper Ni-Ti is recommendedfor the initial wire. Even if there is minimal crowding,we start with this light round wire in order to gentlystimulate biological cellular activity, which in turn initiates tooth movement. The challenge for most orthodontists is avoiding the temptation to use larger wirestoo soon.Dr. White: Isn’t there a new .013 round DamonCopper Ni-Ti wire now available?Dr. Bagden: Yes. This lighter force wire is particularly useful with extremely crowded dentitions, periodontally compromised patients or those who haveunusual sensitivity (Figure 1). I estimate using the.013 dimension as the initial wire in about 10-15%of my cases.Dr. White: So I’d never want to begin a case with awire larger than an .014 Copper Ni-Ti?Dr. Bagden: Never. Whether a case is minimally orextremely crowded, .013 or .014 Copper Ni-Ti are theonly wires of choice. This is a paradigm shift for manypractitioners and I cannot emphasize its importanceenough.Dr. White: Explain the process of posterior transverse arch adaptation and how it helps resolvecrowding in most dentitions without extractions,molar distalization or rapid palatal expansion.2d2eDr. Bagden: Ourresearch indicatesthat when forces arenot excessive andmolars or bicuspidsare not boundtogether with TPAsor lingual arches,etc., we see whatDwight calls posterior transverse archadaptation. Theadditional archwidth that is gainedby this process produces the spacerequired to resolvemost crowded dentitions without extractions, molardistalization or rapid palatal expansion (Figures 2a-g).The positive effect on the midface is dramatic. Smilesare broader, midfaces are fuller and esthetics are ultimately improved. Dr. Tom Pitts calls this phenomenona patient-centered term, “the magic of the midface.”Figure 1. The DamonSystem has added a newdimension archwire, an.013 Copper Ni-Ti, for useas the initial archwire inspecific cases. All DamonCopper Ni-Ti wires nowcome with preloadedcrimpable stops.Dr. White: So clinicians who think of passive selfligation as simply a way to make archwire changesmore efficient and ask whether they need to changetheir mechanics to use Damon are missing its greatest benefits, wouldn’t you say?Dr. Bagden: Yes, I would. The Damon System is justthat – a system. The simple mechanics prescribed forthe Damon System (what we refer to as the establishedprotocols) have been designed to help us capitalize onall the benefits it has to offer. Using it as a bracket andnot a system is like having an advanced GlobalPositioning System (GPS) in your car and pulling to theside of the road to use a printed map. Like learningGPS navigation, adopting Damon mechanics takes a bitof discipline, but once you get the hang of it and, moreover, learn to trust it, you can achieve superior resultswith far fewer appliances, fewer extractions and withmore efficiency than you have ever thought possible.2f2gpalatal expanders and produces the space required to resolve most crowded dentitions without extractions. The positive effect on the5
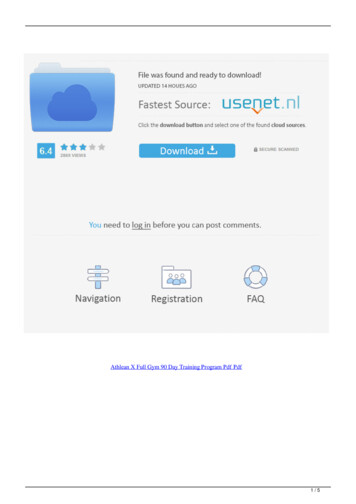
CASE 180% OF CASES ARE 80% COMPLETEIN 8 MONTHSFigures 3a-c. The maxillary posterior transversearch adaptation in this case resulted in an 11 mmchange at the first premolars and a 14 mm changeat the first molars.Dr. White: What specifically doyou mean when you say you’reusing fewer appliances with theDamon System?Case 1 illustrates my experience with theDamon System that 80% of my casesare 80% complete in 8 months. Female,14 years old, presented with a skeletalClass III and an anterior crossbite.Dr. Bagden: One of the things thatI get most excited about with theDamon System (and I know mypatients and staff love this, too) isthe posterior transverse arch adaptation we get without the use of rapidpalatal expanders or W-arches(Figures 3a-c). I’ve seen up to 14 mmof width gain without an RPE.In addition, the anchoragedemands of the Damon System arefar lower than with conventionalsystems; thus, we have been able tonearly abandon the use oftranspalatal arches (TPAs) andNance-holding arches. In fact,using them is a hindrance. One ofthe biggest mistakes I see cliniciansmake is binding molars togetherwith TPAs and lingual arches, etc.,which precludes the posteriortransverse arch adaptation. Theposterior transverse arch adaptationmust not be inhibited by any ofthese appliances. We have alsonearly eliminated compliancesensitive functional appliancessuch as Twin Blocks or activatorsand I rarely ever need headgear. Theone appliance that I now use morefrequently is the Flip-Lock Herbst*,which actually gives a Frankel-typeeffect with the rods acting as buccalshields. The most recent designs arefast and effective. All in all, theAt 8 months, the case is 80% completewith the stainless steel archwire in place.The arch form is symmetrical, toothpositioning is excellent and the case isset up to finish in a short period of time.Figures 4a-b. Giventhis young man’s flatmidface, extractiontherapy would havebeen detrimental tohis facial esthetics.With the DamonSystem, he was treated to a beautifulresult without extractions or rapid palatalexpansion.*Herbst is a registered trademark of Dentaurum, Inc.6tremendous reduction in the number and types ofappliances we use has made my practice far moreefficient than ever before.Dr. White: I’ve heard you state that you don’textract for space, only for the face. Could youexplain that?Dr. Bagden: The posterior transverse arch adaptation that we get with the Damon System almost alwaysproduces enough space to resolve crowding, even inextremely crowded dentitions. I now use profiles andlip musculature – soft-tissue criteria rather than hardtissue analysis – as my guides in determining betweenextraction and nonextraction therapy (Figures 4a-b).I find using the Ricketts E-plane is particularly helpfulin making these decisions. If extractions will help theprofile of the patient (such as in bimaxillary protrusive cases) or extractions are needed for tooth-sizeirregularities, missing teeth, etc., then we’ll extract.Facial esthetics is the primary determining factor.Dr. White: How would you describe the quality ofthe results you’re experiencing with the passiveDamon System?Dr. Bagden: The goal is always to deliver the highestquality care. The Damon System allows me to do thatby getting cases to a place where we candetail them to a beautiful finish faster thanany other system. I quantify it this way: 80%of my cases are 80% complete in 8 months(Case 1). This phenomenon gives the bodyample time to reorganize itself and to allowthe system to deliver the things we associatewith the highest quality result: e.g., rootparallelism, proper contacts, appropriateintercuspation, midline correction andproper torque.
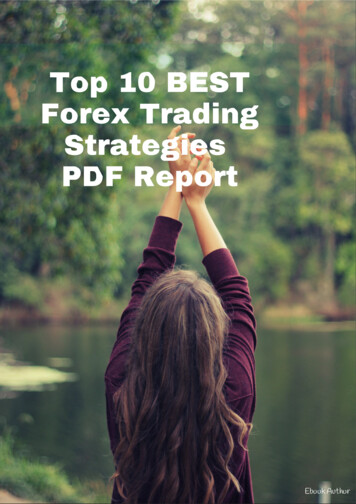
PRETREATMENTCENTRIC RELATIONCENTRIC OCCLUSION ILLUSTRATES ANTERIOR CROSSBITE.INITIAL BONDINGMAXILLARY ARCH FULLY BONDED. GELB APPLIANCE USED IN MANDIBLE TO DISARTICULATE THE JAWSAND CORRECT THE ANTERIOR CROSSBITE.80% COMPLETE IN 8 MONTHS.7
Dr. White: What about adult periodontal cases?Dr. Bagden: As dramatic as it may sound, I have actually seen periodontal situations improve in the nonextraction Damon cases. By not having to move teethgreat distances – as is done in extraction cases – and bymaintaining incisor and canine positions, an experienced Damon practitioner can comfortably treat adultperiodontal patients to great success (Case 2).Dr. White: Do you have any specific protocol forplacing Damon brackets?Dr. Bagden: Accurate bracket placement is essentialfor good orthodontics and this is as true with theDamon System as it is with any other appliance. Thenew Damon 3 (D3) brackets are easier to positionthan their predecessors (Figure 5). The rhomboidshape of the D3 bracket, combined with its water-solubleFace Paint , provides the visualcues and bracket-to-tooth contrast we need to place thebrackets quickly and accurately.For the most part, positioningis the same as for an Orthos bracket; however, I still tend toplace all canine brackets about1 mm mesial to the crown-longaxis of the tooth in order toachieve the desired contactpoint between the laterals andcanines (Figure 6). With thetraditional Damon 2 brackets, IFigure 5. The rhomboid shape of the Damon 3 bracket,follow the same dictate withcombined with water-soluble Face-Paint, provides thethe canines, although using thevisual cues and bracket-to-tooth contrast needed toplace brackets quickly and accurately.bracket pad rather than thebracket itself as the guide toplacement.Dr. White: With the rapidalignment you see in theinitial stage of treatment, Iassume the use of archwirestops is important.Figure 6. To achieve the desired contact pointbetween the laterals and canines, place all caninebrackets at the
Dr. Ron Roth, world-renowned orthodontic educator and clinician, died January 23, 2005. Dr. Roth served as adjunct and clinical professor of orthodontics at several universities and was a founder and director of the Roth/Williams Ce