Transcription
Mitigating COVID-19 in County JailsPresented by the Wayne State University School of Social WorkCenter for Behavioral Health and JusticeAddressing Behavioral Health andCOVID-19 in Jail Settings and BeyondThursday, March 25, 2021
Mitigating COVID-19 in County JailsPresented by the Wayne State University School of Social WorkCenter for Behavioral Health and JusticeWelcomeThursday, March 25, 2021
Welcome & Zoom HousekeepingSequential Intercept Model: A Brief OverviewRisk Factors for People who are Incarcerated with Behavioral Health Needs During the COVIDPandemicIncarceration, Isolation, and COVID-19: Compounding risks and possible mitigation strategiesAgendaAsk an Expert Panel DiscussionCarmen McIntyre Leon, M.D. Chief Medical Officer, Michigan Department of CorrectionsMelissa Zielinski, Ph.D. Assistant Professor & Clinical Psychologist, Psychiatric Research Institute, University ofArkansas for Medical SciencesNanci Hambrick, MSW Project Coordinator, Center for Behavioral Health and JusticeModerated by:Tyler Logan, MA: Project Coordinator, Center for Behavioral Health and JusticeConclusion and Next StepsThursday, March 25, 2021
ZoomHousekeepingSlides will be made available on the CBHJ Website after today’swebinarThis session will be recorded and made publicly availableQ&A chatbox featureThursday, March 25, 2021
Mitigating COVID-19 in County JailsPresented by the Wayne State University School of Social WorkCenter for Behavioral Health and JusticeSequential Intercept Model: A Brief OverviewPresented by Nanci Hambrick, MSWThursday, March 25, 2021
SAMHSA’S GAINS Center (2013), Developing a comprehensive plan for behavioral health and criminal justice collaboration: The Sequential Intercept Model (3rd ed.). Delmar, NY: Policy Research Associates, Inc.Thursday, March 25, 2021
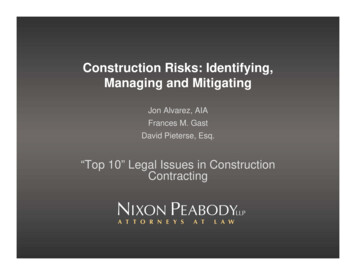
Diversion opportunities across the SIMIntercept 0Intercept 1Intercept 2Intercept 3Intercept 4Intercept 5Community ServicesLaw EnforcementInitial Detention/Initial Court HearingsJails/CourtsReentryCommunity Corrections Mobile crisisoutreach teams Emergencydepartmentdiversion Police officerscan buildpartnershipswith behavioralhealth agencies Standard Dispatch Risk-basedprescreening fortraining totrial servicesmental healthrecognizeand substancebehavioral Data-matchinguse disorders athealth crisis callsinitiativesbookingbetween the Specialized Behavioralcourts,jailandpolice responseshealthcommunitytreatment,including e useTeam traininghealth providerstreatment, is Intervening withrequired by law Specializedfrequent In-reach bytreatmentutilizers andcommunitycourts for highprovidingproviders andrisk/highneedfollow-up afterpartnersindividualsthe crisis.Thursday, March 25, 2021 Transitionplanning by thejail or in- reachproviders Medication andprescriptionaccess uponrelease from jailor prison. Specializedcommunitysupervisioncaseloads ofpeople withbehavioralhealthdisorders. MAT forsubstance usedisorders. Warm hand-offsfrom corrections Access torecoveryto providerssupports,increasebenefits,engagement inhousing, andservices.competitiveemployment.
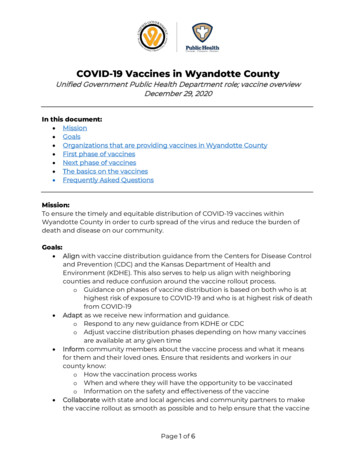
What works according to the data?Intercept 0Intercept 1Intercept 2Intercept 3Intercept 4Intercept 5Community ServicesLaw EnforcementInitial Detention/Initial Court HearingsJails/CourtsReentryCommunity CorrectionsIndividuals with cooccurring substanceuse and mental healthdisorders were over 2times more likely torecidivate than thosewith only a mentalhealth disorder.Delivery of integratedtreatment is hinderedby separate mentalhealth and substanceuse funding and datasystems.Fidelity to the CITModel improvesofficer knowledge andskills and changesbehavior. In themonth after CITtraining, officers were38 times more likely touse the Crisis Center;the increase wassustained 18-monthslater.Across all jails, use ofa standardized mentalhealth screen atbooking improved theidentification ofmental health issues;officer onlyidentification variedfrom 3% - 33%.Across all jails, 47% ofindividuals booking inwere charged with a‘divertible’ offense*.Training correctionsofficers in deescalation techniquesdecreased forcible cellremoval by 50%.Improving dischargeservices (currently,only 30% of individualswith SMI received adischarge service) anddischarging duringbusiness hours (44%Individuals receivingof those with SMI arean in-reach orreleased from jaildiversion service in jailduring non-businesswere twice as likely tohours (5pm –receive a mental8am))will enhancehealth service in thecontinuity of care.community.* Divertible offenses are defined asmisdemeanor, civil ordinance,and/or violation offenses.Thursday, March 25, 2021Enhancing therelationship betweencounty-level CMH andparole/probationofficers may decreasethe number ofindividualsincarcerated forprobation/paroleviolations. Currentlyfour of ten countiesreport such arelationship.
Best Practices Across Intercepts Cross-systems collaboration and coordination of initiatives. Routine identification of people with mental health andsubstance use disorders and/or COVID-19 symptoms. Access to medical treatment for mental health and substance usedisorders. Linkage to benefits to support treatment success, includingMedicaid and Social Security. Information sharing and performance measurement amongmedical, behavioral health, criminal justice, andhousing/homelessness service providers.Thursday, March 25, 2021
Practical Recommendations for Jails Know your population Screen, identify, refer and treat Reduce risk of harm to inmate and staff Identify familiar faces Who is part of the revolving door? Reach out to community providers Invest in collecting data Data driven decisions Data additional funding Partner with your health department and community mental health agency Support in-reach and provide access Share information about who is in your jail daily Smart releases Discharge planning Release people in behavioral health treatment during business hoursThursday, March 25, 2021
Mitigating COVID-19 in County JailsPresented by the Wayne State University School of Social WorkCenter for Behavioral Health and JusticeRisk Factors for People who are Incarcerated withBehavioral Health NeedsDuring the COVID PandemicPresented by Carmen McIntyre, MDThursday, March 25, 2021
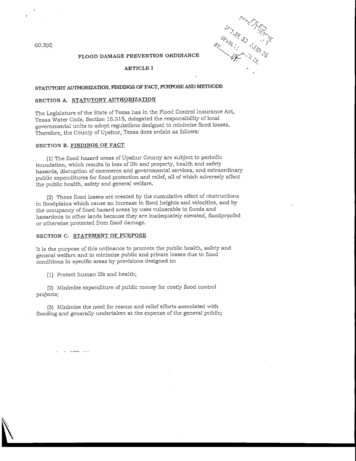
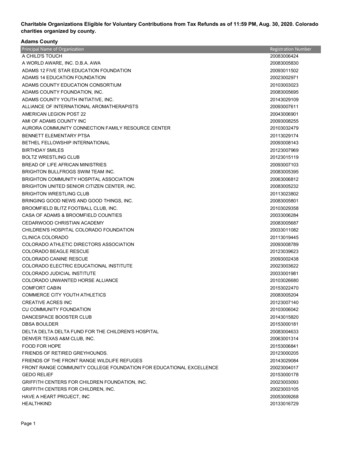
Black/AA Cases70COVID-19Racial DisparitiesLA513242IL291441MI33140102030% deathsThursday, March 25, 202140% cases50% pop607080
MDOC Racial ursday, March 25, 2021AsianAmerican Indian or AlaskanNative
Prevalence of Mental IllnessPrisonCommunity SMI-14% PTSD-48% Schizophrenia-10% ADD-25% Bipolar-16% Major Depression-29% SMI-10% PTSD-6% Schizophrenia-1% ADD-5% Bipolar-4% Major Depression-13%Prins S. J. (2014). Prevalence of mental illnesses in US State prisons: a systematic review. Psychiatric services (Washington, D.C.), 65(7), 862–872.
Because of COVID-19 13% started orincreased substanceuse 11% seriouslyconsidered suicideJun-19 .9Thursday, March 25, 2021
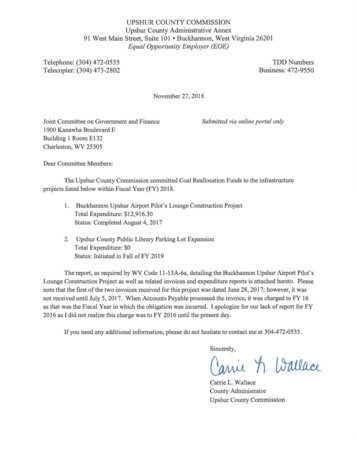
Understanding NSI Risk of self-harm by conditionConditionsAll yearsWithin 1st YearAfter 1st YearDepression14.123.111.7Bipolar Disorder11.6189.7Alcohol Abuse812.86.7Anxiety7.813.66Eating e Abuse6.28.65.4Singhal, A., Ross, J., Seminog, O., Hawton, K., & Goldacre, M. J. (2014). Risk of self-harm and suicide in people with specific psychiatric and physical disorders: comparisons between disordersusing English national record linkage. Journal of the Royal Society of Medicine, 107(5), 194–204.
Mental Illnessas a COVID-19Risk Patients with a severe mental illness have a higher risk forsevere clinical outcomes of COVID-19. (Lee, Lancet 2020) ADHD, bipolar disorder, major depression,schizophrenia Schizophrenia second only to age in increasing the riskfactor for dying of COVID-19. (Goff, JAMA Psychiatry 2021) Persons with schizophrenia also at higher risk forchronic health conditions associated with poor COVID19 outcomes.Thursday, March 25, 2021
PTSD and COVID-19Trauma exposure, especially chronic victimization, is associated with perpetration of crime.Childhood and adult victimization of women associated with higher incidence of SMI, PTSD, and more extensivecriminal history and substance abuse.History of sexual and physical victimization much higher in incarcerated populations than general population.Trauma continues in prison, particularly physical and emotional victimization.Chronic or early childhood trauma associated with inflammation and chronic health conditions, increasing COVID19 poor outcomes.Persons with ICU admissions for COVID-19, and prolonged isolation/quarantine, at higher risk for PTSD.Thursday, March 25, 2021
Mitigating COVID-19 in County JailsPresented by the Wayne State University School of Social WorkCenter for Behavioral Health and JusticeIncarceration, Isolation, and COVID-19:Compounding risks and possible mitigation strategiesPresented by Melissa J. Zielinski, Ph.D.Thursday, March 25, 2021
INCARCERATION, ISOLATION, AND COVID-19:COMPOUNDING RISKS AND POSSIBLE MITIGATION STRATEGIESMelissa J. Zielinski, Ph.D.Assistant Professor Clinical PsychologistUniversity of Arkansas for Medical SciencesMarch 25, 202120
OUTLINE Incarceration as a socially isolative process Compounding effect by COVID-19 Examples Policy data Practical strategies for attempting to mitigate harm21
INCARCERATION AS A SOCIALLY ISOLATIVE PROCESS22
INCARCERATION AS A SOCIALLY ISOLATIVE PROCESSLeast IsolationDormitory HousingGroup podsMost IsolationDouble-occupancy cellsSolitary ConfinementStatus may change over time23Status may change due to COVID precautions
INCARCERATION AS A SOCIALLY ISOLATIVE PROCESS24
INCARCERATION AS A SOCIALLY ISOLATIVE PROCESS25
COMPOUNDING IMPACT OF COVID-1926
Dallaire et al., 2021COMPOUNDING IMPACT OF COVID-1927
COMPOUNDING IMPACT OF COVID-19 Lockdowns Movement restrictions Medical isolation Quarantining28
COMPOUNDING IMPACT OF COVID-19 Anticipate that there will be negative effects of lockdown Almost all people subjected to prolonged isolation experience negativeeffects. This is true even for people who do not have pre-existing mentalhealth diagnoses. Negative effects may persist even after isolation ends.29
COMPOUNDING IMPACT OF COVID-19 Common reactions include: Physiological reactions, such as low appetite, trembling hands, heart palpitations,sweaty hands, lethargy, and sleep disturbances. Confusion and impaired concentration. Hallucinations, paranoid ideas, and aggressive fantasies. Emotional reactions, such as mood swings, panic, anxiety, rage, depression, and irritability.30
COMPOUNDING IMPACT OF COVID-19 Certain people are at especially high risk when isolated: People with existing mental illness Pregnant and postpartum women Older adults31
PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM32
PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM33
PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM Provide opportunities for meaningful social interaction Within the facility Via expanded access to technology34
Dallaire et al., 2021PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM35
PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM Counteract sensory deprivation Lighting consistent with human sleep-wake cycle Continuous access to amenities (radio, television) Continuous access to enrichment activities, personal items Snacks between meals to provide sensory variation36
PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM Prioritize relief from confinement Daily time outside cell Access to outdoor exercise Daily updates/orienting information Control over environment, however small37
PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM Remember your partners If you are used to having volunteers, ask them for help Written materials, activities, etc.38
PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM39
PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM40
PRACTICAL STRATEGIES FOR ATTEMPTING TO MITIGATE HARM41
COPIES OF RESOURCE SHEETS MJZielinski@uams.edu42
Panel DiscussionDr. Carmen McIntyre Leon, M.D.Chief Medical Officer, MichiganDepartment of CorrectionsMelissa Zielinski, Ph.D.Assistant Professor & ClinicalPsychologist, PsychiatricResearch Institute, Universityof Arkansas for MedicalSciencesThursday, March 25, 2021Nanci Hambrick, MSWProject Coordinator, Center forBehavioral Health and Justice
Conclusion & Next StepsNext Webinar: April 22nd at 1PM (EST)FeedbackToolkit UpdatesPeer FacilitationThursday, March 25, 2021
Brad RaySheryl KubiakProgram DirectorCenter for Behavioral Health andJusticeWayne State UniversityBradRay@wayne.eduDean, School of Social WorkCenter for Behavioral Health andJusticeWayne State UniversitySpk@wayne.eduTyler LoganBianca BurchProject CoordinatorCenter for Behavioral Health andJusticeWayne State UniversityTyler.Logan1@wayne.eduProject CoordinatorCenter for Behavioral Health andJusticeWayne State UniversityBianca.Burch@wayne.eduStacey CampbellProgram AssistantCenter for Behavioral Health andJusticeWayne State UniversityStacey.Campbell@wayne.eduThursday, March 25, 2021
Presented by the Wayne State University School of Social Work Center for Behavioral Health and Justice Presented by Carmen McIntyre, MD Thursday, March 25, 2021. COVID-19 Racial Disparities 14 14 32 33 29 51 41 42 70 0 10 20 30 40 50 60 70 80 MI IL . MSW Project Coordinator, Center for B