Transcription
1LEGAL ISSUES FOR NURSE ANESTHETISTSLance D. Schreiner, JDTwila Gieser, RN, LNCCZuger Kirmis & Smith
Objectives2 Identify major issues prompting malpractice claims. Identify CRNA risk management issues. Identify tips for improved / defensible documentation.
Topics of Discussion3 Medical Malpractice Major categories of liability/risk Value of documentation Tips for improving documentation Examples and Case Studies
Elements of Malpractice Lawsuit4 Duty Breach Proximate Cause Injury/Damages Economic Noneconomic
Duty and Breach of Duty 5Health Care Provider / Patient relationshipIn performing professional services, a physician hasa duty to exercise such reasonable care, diligence,and skill as are ordinarily possessed, exercised by,and expected of physicians in the same general lineof practice.
Breach of Duty Breach of Duty Failureto follow Standard of Care ExpertTestimony Practice Standards Role of Literature6
Practice Standards vs.Standard of Care (SOC) SOC – what others in the profession would do undersimilar circumstances Practicestandards not relevant unless expert says so Established by “conduct” Complicated process unique to each fact scenario 7AANA Scope and Standards for Nurse AnesthesiaPractice
Proximate Cause 8A proximate cause is a cause which, in naturaland continuous sequence, produces the injury, andwithout which, the injury would not have occurred.It is a cause which had a substantial part inbringing about the injury either immediately orthrough events which follow one another.
Injury/Damages 9EconomicNoneconomic
Issues Prompting Medical Malpractice Claims:10 Failure to Monitor Failure to Document Failure to Follow Standards of Care Failure to Notify/Communicate with the Physician Failure to Advocate
Leading Causes of AnesthesiaRelated Malpractice Claims11 DeathNerve DamageBrain DamageChronic Pain Management
Failure to Monitor12 Incomplete assessments Erroneous interpretation of signs & symptoms Failure to respond to complaints or takinginappropriate or no actions
Failure to Document13 Fail to record all pertinent data Fail to record specific instructions Fail to document patient progress and responseto treatmentAltering a medical record
Failure to Follow Standard of Care14 Fail to follow hospital protocols Fail to check equipment for safe usage Fail to follow physician’s orders
Failure to NotifyFailure to Communicate15 Delay or failure to call physician Fail to listen to patient’s complaints & act on them Failure to follow chain of command to seek higherauthority for treatment
16Miscommunication is the most commoncause of injury or death.JCAHO, 2004
Failure to Advocate17 Fail to question orders when patient conditionwarrants Fail to question incomplete or illegible orders Fail to provide a safe environment Fail to protect patient privacy
Adverse Event? What now?18 Note in chart Describeevent Drugs used Time sequence Who present Be honest with patient & family “I’m Sorry” Statute – NDCC § 31-14-12Notify Risk Management
HIPAA/HITECH and Social Media19 PHIPrivacy RuleWritten and Electronically TransmittedFines and Criminal PenaltiesSocial Media Facebook PDA/CellPhone
20
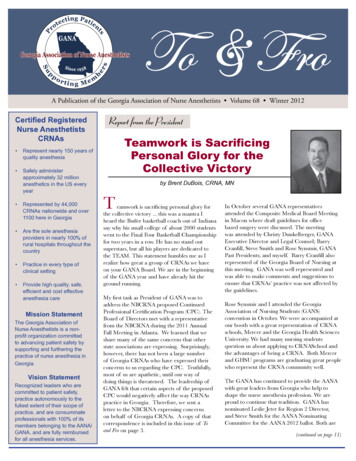
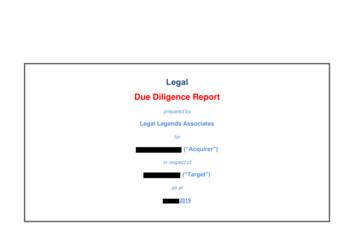
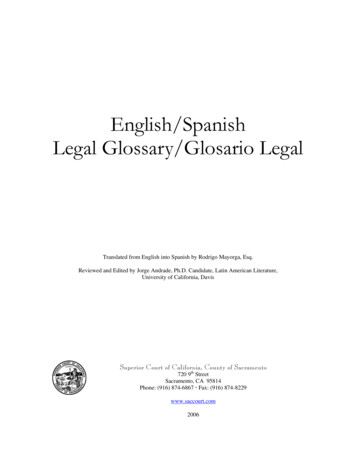
Nurses, Negligence and Malpractice21By Eileen M. Croke, EdD, ANP, LNC-CAmerican Journal of Nursing, September2003, Volume 102, Number 9
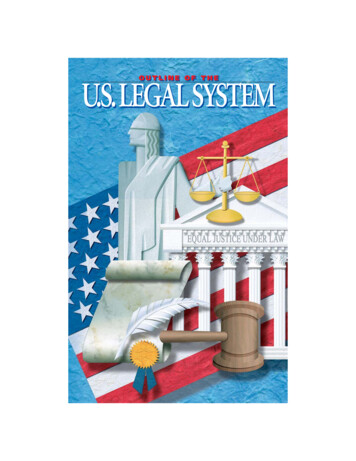
Malpractice Payments by Nursing Category22
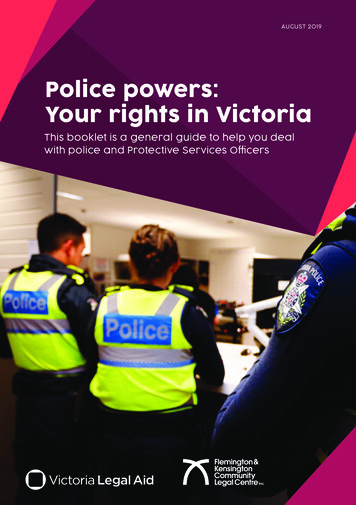
Incidence of Nursing Negligence Allegations by Setting23
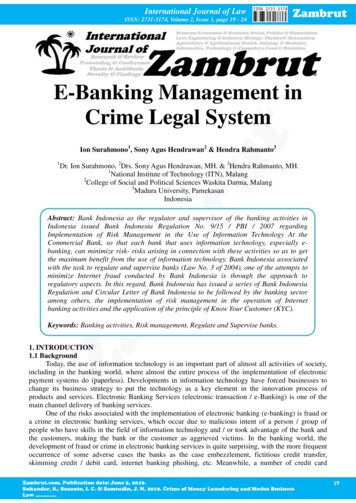
Distribution of Malpractice Cases by Practice Area24
AANA Scope and Standardsfor Nurse Anesthesia Practice25"There shall be complete, accurate, and timelydocumentation of pertinent information on thepatient’s medical record.“"Document all anesthetic interventions and patientresponses. Accurate documentation facilitatescomprehensive patient care, provides informationfor retrospective review and research data, andestablishes a medical-legal record."
AANA Standards forNurse Anesthesia Practice26 Standard I: Perform a thorough and complete preanesthesiaassessment. Standard II: Obtain informed consent for the plannedanesthetic intervention. Standard III: Formulate a patient-specific plan for anesthesiacare. Standard IV: Implement and adjust the anesthesia care planbased on the patient’s physiological response.
AANA Standards forNurse Anesthesia Practice (cont’d)27 Standard V: Monitor the patient’s physiologic condition asappropriate for the type of anesthesia and specific patient needs.Monitor ventilation continuously Monitor oxygenation continuously Monitor cardiovascular status continuously Monitor body temperature continuously on all pediatric patientsreceiving general anesthetic Monitor neuromuscular function & status continuously Monitor & assess patient positioning & protective measures
AANA Standards forNurse Anesthesia Practice (cont’d)28 Standard VI: There shall be complete, accurate, and timelydocumentation of pertinent information on the medical record. Standard VII: Transfer the responsibility for care of the patient toother qualified providers in a manner which assures continuity ofcare and patient safety. Standard VIII: Adhere to appropriate safety precautions, asestablished within the institution, to minimize risk of fire, explosion,electrical shock and equipment malfunction. Document on therecord that the anesthesia machine and equipment were checked.
AANA Standards forNurse Anesthesia Practice (cont’d)29 Standard IX: Precautions shall be taken to minimize the risk ofinfection to the patient, the CRNA, and other healthcare providers. Standard X: Anesthesia care shall be assessed to assure itsquality and contribution to positive patient outcomes. Standard XI: CRNA shall respect and maintain the basic rights ofpatients.
Current Issues in Anesthesia30 Awareness AANAPosition Statement Number 2.12 UnintendedAwareness Under General Anesthesia http://www.aana.com/Resources.aspx?id 24804 Captain of Ship
Best Defense .31Sound PracticesGood Documentation
Value of Documentation32 Permanent medical and legal document Communicate with healthcare team Safety: allergies, medications, treatments Reimbursement issues Accreditation / licensing
Value of Documentation (cont.)33 Research Quality Improvement / Peer Review Risk Management / Legal Issues Regulatory Standards
True or False34If it wasn’t documented, it wasn’t done.
Electronic Health Record (EHR)35 Goals Moreprecise Portable Improve Quality of Care or Not?
6 C’s of Documentation36 CorrectChronologicalClearConciseCompleteConsistent
Concise Documentation37 Avoid “double,” “triple” documentation Use approved abbreviations per policy & procedures (P&P) JCAHO “Do Not Use List”
38
Say what?39AFAWGAs far as wire goes HL the HLHeparin lock the Hickman Line SALTSame as Last Time
Complete and Consistent Documentation40 Make sure patient’s name and facility numberare on each page of each recordSign and date every entryUse “I”Use “quotes”Specifically identify individual namesDocument unusual incidents
Complete and ConsistentDocumentation (Cont.)41 Medications Lookalike/sound alike drugs (www.jcaho.org) High alert medications (www.ismp.org) Confused drug names (www.ismp.org) Use your spell checkLegibleGrammarProof
Just the facts .42
Risk Management43 Licensure responsibilities NursePractice Act AANA Scope & Standards of Practice Continuing education Mandatory Reporting
44
National Practitioner Data Bank45 Mandatory reporting Settlements Judgments Disciplinaryactions Limitations on hospital privileges Entity who pays or disciplines reportAvailable only to hospital and licensing boards
Malpractice Insurance To buy or not to buy?46 Individual Policy Employer’s Policy
Reducing Potential Liability47 Maintain open, honest, respectful relationships &communication with patients, families and colleagues.Maintain competency in your area of practice.Know your state’s practice act and employer’s policies& procedures—follow them.Practice within the bounds of professional licensure.
Reducing Potential Liability (con’t)48 Know your strengths & weaknesses.Thorough pre-op evaluation and follow up ofabnormal test results. Never alter the medical record. Listen to your gut evaluate & re-evaluate.
49Most errors in medical and nursingjudgment can be successfully defendedwhen you are sincere, dedicated &credible.
50The anesthesia record is usually the only continuous,contemporaneously prepared record of the entireoperative procedure.It can be the best defense for you or your colleagues.
Case Examples51
52
53
More Case Examples54
What Happens if I’m sued?55 Anatomy of a lawsuit—complaint to trial What to expect if you are deposed What to do if you are named in a suit
Self Anesthetizing?56
Work as a nurse, but 57Document like a reporter andThink like a lawyer!
Links58 www.ahrq.gov www.guideline.gov www.iom.edu www.ismp.org www.jcaho.org www.ndbon.org www.aana.com
References:59 Austin, Sally. “7 Legal Tips for Safe Nursing Practice.” Nursing 2008, March 2008, p. 3439.AANA Scope & Standards for Nurse Anesthesia Practice, 2007 Cahill, Matthew. Nurses’ Legal Handbook, 3rd Edition. Springhouse Corporation, 1996. Croke, Eileen & Adrienne Mayberry. “Issues Leading to Malpractice Show Little Change: AReview of the Literature.” Journal of Legal Nurse Consulting, Vol. 7, No. 2, April 1996.Davidson, James. “A Look at Leading Malpractice Risk Issues,” Journal of the AmericanAcademy of Physician Assistants, Vol.6, No. 3, p. 23-24, March 1996.Guido, Ginney. Legal Issues in Nursing, 2nd Edition, Appleton & Lange, Stamford, agazine Artlices/article.cfm?AID 11747“Top 10 Documenting Tips,” April 5, 2004.
References (continued):60 http://www.corexcel.com “The Best Defense is a Good ewsletters/newletter23.htm “What Does thatMedication Order Say?”http://www.medscape.com/view article 1432561 “Does Your Staff Know Howto Prevent 121.pdf ND Nurse Practice Act, 2003.Hader, Amy, Brown, Evan. “Patient Privacy and Social Media”, AANA Journal,August 20, 2010, Vol. 78, No. 4.Iyer, Patricia. Nursing Documentation: A Nursing Process Approach. 2nd Edition,Mosby Company, St. Louis, MO, 1995.
References (continued):61 Kosier, Barbara. Fundamentals of Nursing, 5th Edition, Addison Wesley, MenloPark, CA.Loeb, Stanley. Mastering Documentation, Springhouse Corporation,Springhouse, PA, 1995.Marcucci, Catherine. Avoiding Common Anesthesia Errors, 1st Edition, LippincottWilliams & Wilkins, 2008ND Nurse Practice Act, North Dakota Board of Nursing, 2003.Reising, Deanna & Allen, Patricia. “Protecting Yourself from MalpracticeClaims.” American Nurse Today, February 2007, p. 39-43.------, Nursing Malpractice, 2nd Edition, Lawyers and Judges PublishingCompany, Inc., Tucson, AZ, 2001.
AANA Scope & Standards for Nurse Anesthesia Practice, 2007 Cahill, Matthew. Nurses’ Legal Handbook, 3rd Edition. Springhouse Corporation, 1996. Croke, Eileen & Adrienne Mayberry. “Issues Leading to Malpractice Show Little Change: A Review of the Literature.” Journal of Legal Nurs