Transcription
Ryan WhiteMedical CaseManagementPractice anddocumentation review1Originally presented March 28, 2013Slides 59-61 amended March 29, 2013
2Important reminders
3Client records are legaldocuments Records may (and have been in the past)subpoenaedBe careful about putting too much detail in casenotes that may open your agency to liabilityAll documentation must be objective andprofessional No happy faces, no subjective statements unlessquoting a clientDate of document must match signatures No pre- or post-dating documents to technicallymeet deadlines
4Client records are legaldocuments Neveridentify someone else’s status, mentalhealth conditions, or substance abuse in yourclient’s record Do not assume that writing “partner” isdeidentifying -- you likely have a release to thatpartner with his or her name on it in the recordas well Remember:Clients have a right to review theirrecords at any time per HIPAA
5Face-to-face contacts Theannual assessment must be completedface-to-face for both Ryan White andMaineCare Semiannual certifications must be completedface-to-face for Ryan White You cannot complete the document over thephone and then have the client sign next timehe or she comes into the officeYou cannot mail to client to sign
6ADAP ADAPis the payer of last resort Clients must apply to MaineCare ADAP coverage is based on clients’ eligibility If a client is eligible for MaineCare but lostit for failing to recertify, client only receivesADAP coverage wrapping around typicalMaineCare coverage (i.e. ADAP pays 3 or 10 copay) If client has no insurance and then gets anykind of insurance, notify ADAP immediately
7CAREWare issues
8Services Ifyou log a care plan and/orassessment and/or semiannualcertification service, you do NOT needto log “1200 Referral and monitoringservice from care plan” for the samecontact (unless you work at FPC) Do not forget to log “1100 ClientCertification” or you will not be able torun reports to show when nextcertification is due
9Annual review Discrepancybetween annual reviewinformation (required to be reported tothe feds) in CAREWare and info onsemiannual certification in chart If housing, insurance, medical care, orincome information changes, youmust update CAREWare
10Household size and income “Household”is defined as the client and anylegal household members (legally marriedspouse, dependent children, dependentadults) More on this later Incomefor all members of the householdmust be included Ryan White definitions of household may bedifferent from MaineCare and HOPWA.Always report the Ryan White information inCAREWare.
11Labs CMsare required to enter CD4sand Viral Loads in CAREWarewhen they are collected forthe semiannual certification
12CAREWare upgrade Thisis the buggiest upgrade we’ve everinstalled Known bugs: Searching by drop downs (e.g. CM assigned)doesn’t workYou can’t sort any of the search terms that don’tfilter correctly in the find listProvider Notes ARE NOT restricted to Providers(think of them as being the same as CommonNotes)Some issues with permissions and custom fields
13CAREWare upgrade Incomeinfo may look a bit strange,because of the way information rolls over
14CAREWare upgrade Anyother questions about theupgrade? If you come across a problem,please send a detailed emailabout it to be forwarded to theHelp Desk
15Semiannual certificationUpdates to form
16Now two processes New client intake 1-page form completed once at intake Focused on demographic data that do notusually change No service in CAREWareSemiannual certification 5-page form completed every six months Enter service # 1100 Client Certification
17
18Updates to semiannualcertification form Someelements rearranged for flow Labs now highlighted to remind CMs toenter in CAREWare Expanded insurance section
19
20Documentation review
21Results from Dec chart reviewsTotal number of records reviewed:Section 1: Client Identification and EligibilityTotal number of records with Section 1 complete:Section 2: Semi-Annual CertificationTotal number of records with Section 2 complete:Section 3: AssessmentTotal number of records with Section 3 complete:Section 4: Consent FormsTotal number of records with Section 4 complete:Section 5: Care PlanTotal number of records with Section 5 complete:Section 6: Case Notes and MonitoringTotal number of records with Section 6 complete:Section 7: Client Record DocumentationTotal number of records with Section 7 complete:Section 8: Discharge SummaryTotal number of records with Section 8 complete:Total number of records with all sections %1838% ** Contractual expectation: 90% of client records audited during the contract year are complete
22Improvement Continuingto have high completionrates in certain areas Client identification & eligibility (96%) Assessment (98%) Discharge (98%) Ratings in care plan section showingprogressive improvement Currently at 67%
23Problem areasClient record documentation Down to 69% (from 84% in June) Income verification Consent forms Case notes & monitoring Care plan
24Client record documentation
25Forms must be completed Ifa client identifies no needs in anarea, the zeroes still need to befilled out on the acuity scale If you use a second page of a careplan only for signatures, the blankboxes above must have a linedrawn through them
26Forms must be completed
27Forms must be completed
28Forms must be completed
29Forms must be completed
30Why be so picky? From Maine’s Notary Guide:Blanks may affect the validity of a documentNever use “white out” products to alter adocument. If language needs to be altered,the signer should cross out or line through thelanguage and initial all altered areas in thedocument. Althoughforms are not notarized, they arelegal documents and must be held to thesame standard
31Income verification
32Continuing issues Requiredfor entire legal household If client has a legal spouse, thespouse’s income must bedocumented as well Required to be verified every sixmonths Document must be less than oneyear old
33What’s a “legal spouse”? Same-sexspouses previouslymarried in other states Same-sex spouses recently marriedin Maine Separated spouses who are not yetdivorced
34Income verification Ifclient fails to provide incomeverification within 30 days, he orshe must be discharged from RyanWhite case management perHRSA requirements
35Consent forms
36Releases for MaineCare Youdo not need a release to MaineCareto discuss services they pay for that youprovide e.g. “Did you see John Doe on Thursday?” YouDO need a release to MaineCare todiscuss: a client’s coverage and eligibilitythe client’s adherence to medication/medpickupsthe client’s use of the ER
37Other issues Makesure release forms arecompletely filled out Draw a line through blank areas,just like any other document Fill in all dates Clearly indicate the intent of therelease
38Case notes & monitoring
39Recurring issue Leavingparts of the case notetemplate blank Fillin blank areas, just like anyother document Ifno referrals made or no followup necessary, write “none”
40Most common issue Insufficientstatement of howthe contact supports treatmentadherence Lengthier does not mean moreaccurate
41Examples of good treatmentadherence statements transition to new PCPViral load increasingfollow up for PCP blood workclient experiencing difficulty getting prescriptionsthrough new mail-order pharmacyCoordination and monitoring of housing needs helpsclient stay focused on adherence to treatment.Coordination of insurance enables client to access medswithout interruption.Addressing barriers to care enables client to maintainfocus on adherence to treatment.Stable living situation allows client to attend to HIV selfcaregood dental hygiene decreases risk of opportunisticinfection
42More examples good vision allows clients to read medicine bottlesTo go over goals to ensure client is getting enoughservices to stay adherent to meds.maintaining a good diet helps with keeping clientadherent to meds.to obtain stable housing for medicationadherence, to obtain job so that client is able toget some income to afford basic necessities andto see his provider to get medications to stayhealthyContinued connection to PCP enhances healthoutcomes
43More examples Adequatefood/nutrition enhances healthoutcomes Access to dental care enhances overallhealth. Transportation to attend medicalappointment Good mental health/social supports improvesoverall wellbeing, and decreases depressionand despair, which improves treatmentadherence Accessing/ maintaining benefits ensures thatclient is able to access services and care
44Care plans
45Care plan issues1.2.3.Care plan goals do not match needsidentified on assessmentCare plans in chart not reviewed in personor by phone and signed by CM Usually relates to client who wasdischarged (see next slide)Client has not achieved at least 4 shortterm goals Usually due to goals not being specificenough or issue on next slide
46Review care plans at discharge Whendischarging a client,review the care plan to showthe status of goals at the timeof discharge
47Care plan goals Mustcorrespond to an identified needon the assessment If a new need arises, use theAssessment Update form to document Make sure it is clear from the narrativein the section why this is a need Althoughthis will not keep a chart frompassing a review, it is a common issuenoted in state audits
48Problems with goals Manycare plans with exact samegoals carried over for a year ormore Many care plans with exact samegoals for all clients on a caseload Care plan goals not specificenough Care plan goals not achievable
49SMART Goal WritingFor client care plans and agency action plans
50SMART Goals Specific Measurable Achievable Relevant Time-bound
51Specific Aspecific goal has a muchgreater chance of beingaccomplished than a generalgoal. Who is doing the activity? What is the action/activity?
52Measurable Establishconcrete criteria formeasuring progress toward theattainment of each goal you set. How much change is expected? Will there be an increase ordecrease? Can you measure it?
53Achievable Canit be done? Can you accomplish it in theprescribed timeframe? Do you have the necessaryresources?
54Relevant Doesthe action relate to whatyou want to accomplish? Is it important and meaningful? Does it relate to broader, longterm goals for theclient/program/organization?
55Time-bound Whatis the timeline for change? When will this be accomplished?
56Action Planning Everyagency continues to fall belowperformance targets for completerecords Every agency fell below theperformance target for hours per FTEper week for at least one quarter thisyear Most fell below the performancetarget every quarter
57Hours per FTE per week Since2008, the Ryan White Part BProgram has been tracking hours perFTE per week Expectation is that MCMs will spendhalf of their RW-funded time on directclient service The other half is for paperwork,CAREWare entry, meetings, etc.
58Why? Itis not unreasonable to expect that half of acase manager’s RW-funded time be spent ondirect service If this is not happening, there are importantquestions to ask: Is the CM spending time on non-RW activities?Is the CM not accurately reporting RW time?Should the budget be adjusted to pay for lessdirect RW time?
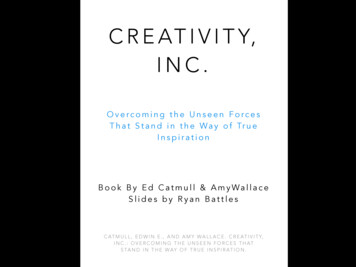
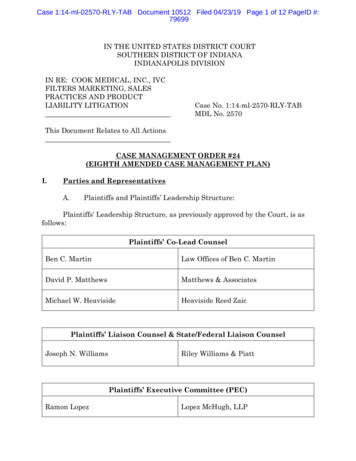
59How we calculate it Allclient time logged in CAREWare for theperiod Jan. 1-Dec. 31, 2012 Travel time to and from clientappointments logged in CAREWare forthe period Jan. 1-Dec. 31, 2012 Divided by 44* weeks (to get hours perweek) Hours per week divided by FTE incontracts (to get percent of FTE)* Reduced from 52 to account for 12 holidays and 28 vacation/sick days
CM% 231%1331%1426%1522%1612%60 5out of 16 RW-fundedmedical case managers meetthe standard for calendaryear 2012 Median 38% That means, in a regular 40-hourwork week, 15 hours were spent meeting with clients by phoneor in person having collateral contact onbehalf of clients driving to and from clientappointments
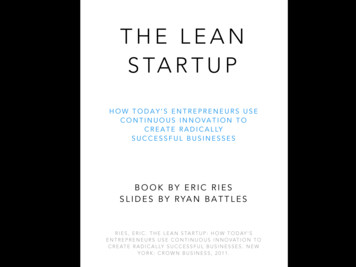
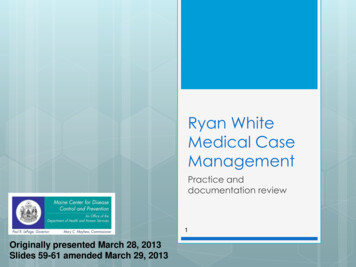
CM% 233%1333%1428%1527%1615%61Adding Training Time Add20 hours per year to totalhours for training (per contractstandard), regardless of FTE Same 5 out of 16 RW-fundedmedical case managers meetthe standard for calendar year2012 Median 39% 16 out of 40 hours
62Action Planning Continuedissues with recordreviews and hours per FTE showthat current improvementstrategies aren’t working Now what?
63How to write an action plan Currentaction plan form has two columns: Issues to be addressed (filled in by MaineCDC) Specific steps agency will take toaddress the issue in the next threemonths An explanation for performance is not aspecific step to change the outcome inthe next quarter
64How to write an action plan Choose one idea to implement immediately toget you from your current state to your desiredstateWhat action(s) will you take to implement theidea?What do you expect to happen as a result of youractions? (i.e. what are the outcomes?)How will you know if you’ve made animprovement? (i.e. how will you measuresuccess?)If no improvement, revisit the idea or select a newidea to test
65ExerciseAction Planning
66Group 1 Brainstormabout how to improve recordcompletion Pick a strategy Come up with an action plan
67Group 2 Brainstormabout how to improve hoursper FTE per week Pick a strategy Come up with an action plan
68More on record reviews
69State audits vs. agency audits Formany years, agency-conductedaudits result in higher percentagesof complete records than stateconducted audits Audit lists are selected randomly Why the differences?
70Review criteria vs. other problems Achart can pass the review and stillhave many significant issues, includingpossible legal ramifications State audit results include notes onitems that did not cause the chart tofail review but should still be reviewedand, if possible, corrected
71Examples Missingcase notes or missing service entries Late services (assessment, care plan,certification) Identifying someone else’s (usually apartner’s) HIV status Case notes indicating that contacts that arerequired to be face-to-face occurred byphone Allsemiannual certifications and the assessmentare required to be conducted face-to-face
72Examples Releasesnot being specific enough Releases being too specific Case notes containing too much detail Risk of identifying another person’s(usually client’s partner) HIV status, mentalhealth conditions, and/or substanceabuse without permission Unnecessary in most cases Wastes time
73What Maine CDC looksfor in audits
741. Client identification &eligibility Chart includes client contact information? Compared to what’s in CAREWare. Discrepanciesnoted without affecting section rating.Chart includes acceptable documentation ofHIV/AIDS diagnosis? Must include client’s full legal name. Sources:Medical records Confidential detectable viral load results Confidential HIV antibody test results Statement from the client’s medical provider verifyingthe client’s HIV status
752. Semiannual certification Chart includes Semi-Annual Certification in last 6months?Chart includes all required Semi-Annual Certificationsfor past year?Current Semi-Annual Certification signed by client?Current Semi-Annual Certification includes incomeverification?Current income verification present for all members ofclient's legal household?Current Semi-Annual Certification includes insuranceverification? Copies of insurance cards Printout from MIHMS portal
763. Assessment Assessmentdone within last year? From audit date or dischargedate
774. Consent forms Allrequired releases on file? A release for every collateral contact in casenotes, including specific people identified All releases are completely filled out, signed,and dated? No blanks All releases clearly indicate the intent of thecontact/release of information?
785. Care plan Chartincludes Care Plancreated/updated in last 6 months? Care Plan signed within the last year? Chart includes all required Care Plansfor past year?
795. Care plan Care Plans in chart are reviewed with client inperson or by phone and signed by CM? Review section of form is filled in, includingoutcomes of goals CM signs review sectionCare Plan goals are needs identified on theAssessment? Compares acuity areas fromassessment/assessment updates to goal areas oncare plansClient achieved at least 4 short-term goals in thepast year?
806. Case notes & monitoring Each Case Note entry includes date and casemanager’s name?Each Case Note indicates care plan goal thatcontact supports?Referrals are documented? If none, write “none”Collateral contacts are documented?Case Notes indicate how contact supportstreatment adherence?Prevention contacts are documented at leastonce per year? Usually in assessment, otherwise in case notes
817. Client record documentation Allforms are complete, with N/A notesin sections that are not filled in? Whole sections of forms must be leftblank or there must be numerousrepeated blanks to receive a “No.”Other blanks will be noted, but willnot affect the chart rating.
828. Discharge summary Dischargesummary completed? If applicable No blanks on form
83ExerciseMock chart review
CAREWare upgrade This is the buggiest upgrade we’ve ever installed Known bugs: Searching by drop downs (e.g. CM assigned) doesn’t work You can’t sort any of the search terms that don’t filter correctly in the find list Provider Notes ARE NOT restricted to Providers (think of them as being the same as Com