Transcription
Joseph Sacco, MDProject Medical DirectorNew York–Reducing AvoidableHospitalizationsJune 3, 2015
2CMS Initiative to Reduce AvoidableHospitalizationsSponsored by Medicare-Medicaid Coordination Office incollaboration with Center for Medicare and Medicare InnovationGoals of the Initiative Reduce frequency of avoidable hospital transfers Increase quality of care and reduce overall health care spending Improve transition process between hospitals and nursing facilitiesAvoidable? There are ways at looking at the diagnosis that resulted in transfer to the hospitaland admission to the ER On those, you could say yes, this seems like it was avoidable – that the problemcould have been managed at the nursing home
3Population FocusLong-stay residents (101 days), VA, Medicare and/orMedicaid enrollees Complements initiatives focused on the short-stay populationMedicare fee-for-service enrollees CMS believes that Medicare beneficiaries enrolled in managed careare already receiving some of these care coordination benefitsThis population of often frail and elderly people may notbenefit from the disruption of a transfer to the hospital
4Initiative ProjectsProjects are four years September 2012 through September 2016Seven projects across the US Alabama, Indiana, Missouri, Nebraska, Nevada, New York, PennsylvaniaTwo projects use “hands off” models New York’s and Alabama use nurses as educators and consultants Five projects use advanced practice nurses to provide supplemental careOur project brings resources to the nursing facilities Registered nurse care coordinator (RNCCs) placed at nursing facility topartner with staff, provide training in tool use and palliative care, and gatherproject data
5New York – Reducing AvoidableHospitalizations (NY-RAH)NY-RAH administered by GNYHA Foundation Collaborating with Icahn School of Medicine at Mount SinaiGoals for NY-RAH Build capacity to use structured communication tools and improvepalliative care Build capacity for electronic transfer of information betweennursing facilities and affiliated hospitalsEarly success Implementing and sustaining interventions Attention to Acute Changes of Condition (ACOC) Increase in rate of advance directives
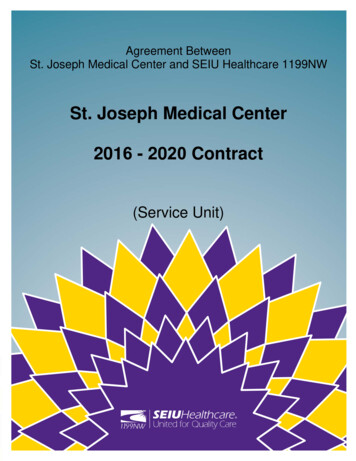
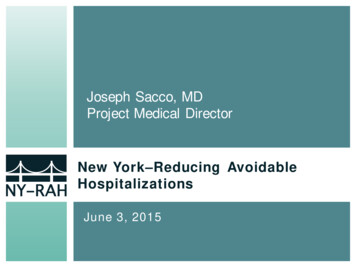
629 NY-RAH Facilities in NYCand Long Island
Facilities and BeneficiariesFacilitiesAmsterdam at brew Home for the Aged at Riverdale176Buena Vida Continuing Care199Palisade Nursing Home Company234Casa Promesa127Peconic Landing At Southold Inc35Cold Spring Hills Center for Nursing and Rehab334Riverhead Care Center LLC96Daughters Of Jacob Nursing Home Co, Inc405Schervier Nursing Care Center294Dr William O Benenson Rehabilitation Pavilion236Silvercrest E C F270Flushing Manor Nursing Home161Smithtown Center For Rehab & Nursing CareGood Samaritan Nursing Home8995St Catherine Of Siena144153Greater Harlem Nursing Home Co200St James Healthcare CenterGurwin Jewish Nursing And Rehabilitation Center373St Mary’s Center Inc40Highfield Gardens Care Center Of Great Neck141Suffolk Center For Rehabilitation And Nrsg95Highland Care Center267Terence Cardinal Cooke H C C384Trump Pavilion for Nursing and Rehabilitation140Workmens Circle Multicare Center423Island Nursing And Rehabilitation Center Inc83Jewish Home Lifecare - Manhattan Division236Long Island State Veterans Home368
8Facility CharacteristicsSize Number of beneficiaries per facility ranges from 30 to 400 Median number of beneficiaries in facility is 175 Seven facilities have 300 beneficiaries Three facilities are specialty nursing facilities for HIV/AIDSresidentsSpecial Five facilities have a ventilator unit (one with 80 vent beds)PopulationsTransfers 5,052 eligible transfers to 70 hospitals in 2014 57% of the transfers were to 10 hospitals
9Why did nursing facilities jointhe project?Getahead ofthe tidePush byhospitalpartnersForwardthinkingnursing facility
10INTErventions to Reduce AcuteCare Transfers (INTERACT)Curriculum of tools Structure is brought to communication among staff Designed for use in a nursing facilityIn order to act appropriately and timely: Nurses need certain information from front-line staff Physicians need certain information from nursesSome facilities have used the tools here and there NY-RAH wants it to become a regular process
11Stop and WatchTool designed for completion by front line staff CNAs Environmental services Families?Why them? They are spending the most time with the resident Most likely to notice changesCompletedStop and WatchNurse
12Stop and Watch Focus: CNA to Nurse Communication
13Stop and Watch
14SBARTool designed for completion by nurses Nursing supervisor Register nurse LPNWhy them? They are going to communicate with the physician Need all the information togetherCompletedSBARPhysician
15What is the SBAR?Nurse to physiciancommunicationSituation What is thesituation thatyou are callingabout? What is goingon?Background Pertinentclinical andotherinformationrelated to thesituationAssessment /Appearance What do youthink may begoing on withthe resident? Is the problemsevere or lifethreatening?Recommendation What is neededand in whattimeframe? What do you needfrom thephysician/practitioner?
16SBAR SBAR is widely used in acute care settings Most nursing home EMRs have an SBAR format that can beadapted and serve the same purpose
17“Know It All” CardsReference tool for management of 78symptoms Complements the SBAR process Common complaint among physicians: “I don’t haveenough information to make a proper recommendation”Assists nurse with determining accuratehistory of resident and situation Goal is to have complete information prior to contactingphysician NY-RAH wants: ”Have you completed the SBAR?”
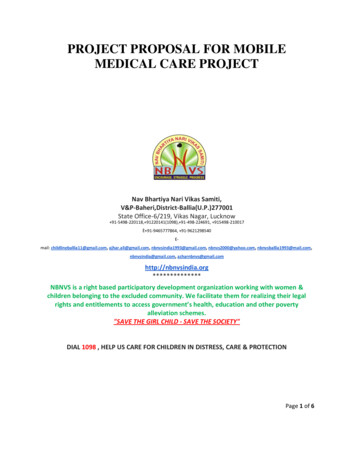
19Progress w ith NY-RAH Tool UsePercent of ACOCs with a NY-RAH Tool* Used60%55%50%45%40%35%30%25%20%Apr. May June July Aug. Sept. Oct. Nov. Dec. Jan. Feb. Mar.20142015A N Y- R AH tool c om pr ises any of the following tools : Stopand Watc h, SBAR , or Know- It- All Before You C all c ards
20Progress w ith Palliative Care Robus t palliat ive c ar e polic ies and c ar e plan meet ing polic ies have beenadopt ed or impr oved upon at a major it y of f ac ilit ies
21Other NY-RAH FeaturesAction PlansMOLST & eMOLST Completed in Year 2 to identifystrengths and improvementareas Updates in Year 3 to assessprogress Medical Orders for LifeSustaining Treatment (paper orelectronic) form expected to behonored across care settings Previously little used for/bypatients in New York City areaQI “Deep Dive”Electronic Solutions Summarizing findings of QITools for an area of focus Making recommendations forimprovement to avoid transfers Use of Summary of Caredocument via “DirectMessaging” that meetsMeaningful Use 2 requirementsfor hospitals
22Focus Areas for 2015ClinicalInterventionPalliativeCare Coaching staff on further use of NY-RAH toolsContinuing “Deep Dive” processWorking on barriers to treating residents in facilityExamining patient experience during necessary transfer Increasing MOLST and eMOLST use Introducing Palliative Care Order set Analyzing residents with long hospital stays aspalliative care opportunities
23Project Challenges Some nursing facilities think there is little room forimprovement Concern about liability if hospital transfer is not done Staff are already very busy Staff already have so much to document
24Lessons Learned Using data is unfamiliar to leadership at somenursing facilities Hospitals and nursing homes don’t understand eachothers’ processes Nursing homes are willing to adapt under the rightcircumstances Staff are already busy so everyone has to see thebenefit of something new
Cold Spring Hills Center for Nursing and Rehab 334 Daughters Of Jacob Nursing Home Co, Inc 405 Dr William O Benenson Rehabilitation Pavilion 236 Flushing Manor Nursing Home 161 Good Samar