Transcription
CHDP Pediatric VisionScreeningChild Health and Disability Prevention (CHDP ) ProgramSystems of Care Division (SCD)California Department of Health Care Services7/14/20171
Learning Objectives Understand the importance of visionscreening during childhood. Become aware of eye problems thataffect vision. Describe and implement the CHDPprogram guidelines for referral andfollow-up. Identify the steps of vision screeningand document results.7/14/20172
Why Perform VisionScreening? Recommended as part of the AmericanAcademy of Pediatrics Bright FuturesPeriodicity Schedule For ages where riskassessment isrequired, see BrightFutures Pre-visitQuestionnaire– Available in all ages7/14/20173
Bright Futures Pre-VisitQuestionnaire for 7-year-old7/14/20174
Why Perform VisionScreening? Primary Care Physicians and Nurses:– The first line of defense to detectpreventable vision loss in children Early detection of amblyopia - “lazyeye”– Leading cause of vision loss among children7/14/20175
Amblyopia Amblyopia is the leading cause ofvision loss among children. Eyes and brain are not workingtogether. One eye sees a blurred view and theother a normal view. The brain onlyprocesses the normal view.7/14/20176
AmblyopiaAmblyopia can onlydevelop duringchildhood. If not treated inchildhood, amblyopiamay result inpermanent vision loss. The most commoncause of vision loss inadults 20-70 years ofage is untreatedchildhood amblyopia.7/14/20177
Amblyopia Common causes are:– Untreated or unequal refractive errors(nearsighted, farsighted, astigmatism)– Strabismus “crossed eyes”– Obstruction (e.g. ptosis, cataract)7/14/20178
Common Causes ofAmblyopia1. Types of refractive errorsa. Myopia “nearsighted”: does not seeobjects well at far distances7/14/20179
Common Causes ofAmblyopia1. Types of refractive errorsb. Hyperopia “farsighted”: does not seeobjects well at close distances7/14/201710
Common Causes ofAmblyopia1. Types of refractive errorsc. Astigmatism: an irregular curve in the eyecausing blurry vision at all distances7/14/201711
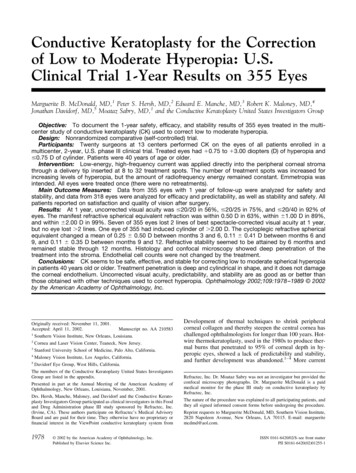
Common Causes ofAmblyopia2. Strabismus “crossedeyes”: misalignment of theeyes– May have double vision– One or both eyes turninginward– One or both eyes turningoutward– One eye turning up ordown7/14/201712
Common Causes ofAmblyopia3. Obstructiona. Ptosis: drooping of an eyelid due to aweak lid muscle. May obstruct vision Look for chin elevation in these children.7/14/201713
Common Causes ofAmblyopia3. Obstructionb. Cataract: condition in which the lens ofthe eye becomes progressively cloudy,resulting in blurred vision.7/14/201714
Screening Early is Best School-aged vision screening may betoo late. Amblyopia is harder to treat after 5years of age. By 7 years of age, some vision lossfrom amblyopia may becomepermanent.7/14/201715
Vision Screening in the UnitedStatesNational Eye Institute (NEI) Amblyopia affects 2-3% of children inthe United States.– About 4.5 million children with preventablevision loss.7/14/201716
Barriers to Screening Poor cooperation of young childrenTakes time to performStaff not adequately trainedPoor reimbursement for physicians7/14/201717
Visual Acuity ScreeningGuidelines7/14/201718
American Academy ofPediatrics Policy StatementPediatrics January 2016 Screening with a tool such as aphotoscreener is recommended forchildren 12 months of age and olderunless they can reliably perform visualacuity screening with eye charts. Visual acuity screening using eyecharts remains the gold standard. It canbegin as early as 3 years of age.7/14/201719
Newborn to 35 Months(0-3 years)Procedures for the Evaluation of the Visual SystemPediatrics January 2016 Take a health history: Are there eye problems inclose relatives? Check vision (tracking), eye movement (motility)and alignment (strabismus) Check pupils and red reflexes (round, equal,bright)NOTE: This assessment can also be done on olderchildren of any age with developmental delays.7/14/201720
Ages 3 through 5 yearsRecommended Chart TypesLEA Symbols7/14/201721
Ages 3 through 5 yearsRecommended Chart TypesHOTV Letters7/14/201722
Age-Dependent Pass/FailGuidelines New AAP guidelines– 3 years old: the critical line to passscreening is the 20/50 line.– 4 years old: the critical line to passscreening is the 20/40 line.– 5 years and older: the critical line to passscreening is the 20/32 line for Sloan andLEA/HOTV (or 20/30 in Snellen chart).7/14/201723
36 to 47 Months (3 years) Must be able to identify the majority ofthe 20/50 line with each eye. Screening is typically done at 10 feet. Opposite eye must be fully covered.7/14/201724
48 to 59 Months (4 years) Must be able to identify the majority ofthe 20/40 line with each eye. Screening is typically done at 10 feet. Opposite eye must be fully covered.7/14/201725
60 Months and Older(5 years) Must be able to identify the majority ofthe 20/32 line (or 20/30 in Snellenchart) with each eye. Use LEA symbols, HOTV letters forchildren who do not know their letters. Use Sloan letters for children who knowtheir letters.– Preferred over Snellen letters chart– Snellen letters chart have a 20/30 line7/14/201726
60 Months and Older(5 years) Recommended screening distance is 10feet using a 10-foot chart. Fully cover opposite eye. Repeat screening every 1-2 years. Risk assessment should be done whenscreening is not required.FOR SCREENING AT 10 FEET7/14/201727
60 Months and Older(5 years) Sloan Letters Chart– Preferred over Snellen Letters.7/14/201728
American Association for PediatricOphthalmology and Strabismus(AAPOS) Vision Screening Kit Acuity charts forthreshold or critical linescreening:– Sloan letters– LEA symbols or HOTVletters Occluderpatches/glasses/paddle 10 foot measuring cord Matching response card Informational DVDs7/14/201729
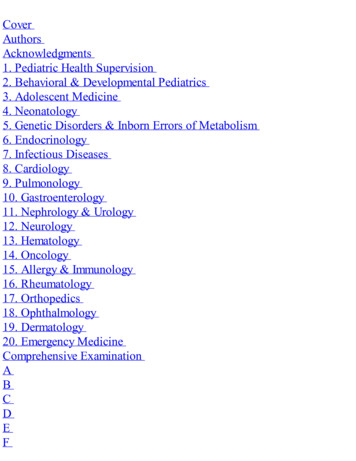
Threshold and Critical LineOptionsThreshold7/14/2017Critical Line30
Threshold Screening Reading down theeye chart as far aspossible. Threshold line is thesmallest line childcan pass. Can identify 2-linedifference betweenthe eyes.7/14/201731
Critical Line Screening:FASTER Only read a single “critical” line with each eye. Each chart has two boxed “critical lines” - onefor each eye. The top line of large optotypes(symbols/letters) is for practice before startingscreening.7/14/201732
Vision Screening Charts NotRecommended7/14/201733
Occlusion of Non-tested Eye Adhesive patchesare best. For all screeningmethods,completely coverthe eye not beingscreened toprevent peeking.7/14/201734
OccludersAcceptableNot RecommendedOnly for age10 years andolder7/14/201735
Key Points Use eye charts with lines of optotypes ormatching cards with lines (crowding bars)around each optotype to obtain the mostaccurate visual acuity assessment. Crowding bars aroundthe optotype makeindividualsymbols/letters moredifficult to identify whenamblyopia is present.7/14/201736
Key Points Screening linemarked at 10 (or20)-feet on the floor. Screening line isdirectly in front ofeye chart. Vision screeningarea– Out of traffic area– Have adequatelighting7/14/2017SCREENING LINE10 or 20 FEETSCREENING LINE37
Key Points Eye chart should be at child’s eye level. Each eye should be screenedseparately (monocularly). Either critical line or thresholdscreening may be used.7/14/201738
Automatic Referral for EyeExamChildren with the following disorders should bypassscreening and should be referred directly to an eyespecialist:1. Recognized eye disorders (e.g. strabismus, ptosis)2. Known neurodevelopmental disorders:7/14/2017 Hearing impairment Motor abnormalities (e.g. cerebral palsy) Down Syndrome Cognitive impairment Autism spectrum disorder Speech delay39
Automatic Referral for EyeExam3. Systemic diseases present (e.g. diabetes,sickle cell disease, hypertension)4. Taking medications known to cause eyedisorders (e.g. some anti-depressants andsteroids)5. First-degree relative with strabismus oramblyopia6. Prematurity: less than 32 weeks of gestation7. Parent believes child has vision problem7/14/201740
Age-Dependent ReferralCriteriaNew AAP Guidelines: 3 years old: Missing 3 or more symbols on the20/50 line, or any line above the 20/50 line,with either eye 4 years old: Missing 3 or more symbols on the20/40 line, or any line above the 20/40 line,with either eye 5 years and older: Missing 3 or more symbolson the 20/32 (20/30) line, or any line above the20/32 (20/30) line, with either eye Two line difference between the eyes, evenwithin the passing range (e.g. 20/20 and 20/32)7/14/201741
Follow-Up Maintain referral log to track status of referral. Follow-up with parent/guardian as needed.42
Untestable Children If child is unable to cooperate during thescreening, make a second attempt the sameday (i.e. later during the same visit). If sameday rescreening is not possible, reschedule assoon as possible, but no later than 6 months. Schedule follow up appointment prior to thepatient leaving provider office. If you cannot screen a child, then refer to anophthalmologist or optometrist experienced inthe care of children for an eye examination.7/14/201743
CHDP Vision ScreeningCertification Requirements Screeners must attend VisionScreening Training led by CHDP staff(or another agency approved by localCHDP). Renew certification every four years.7/14/201744
Instrument-Based VisionScreening Instrument-based screening is theprocess of using an instrument such asa photoscreener, autorefractor or otherdevice, to screen for risk factors forvision problems. Does not replace visual acuityscreening with eye charts. Endorsed by American Academy ofPediatrics (AAP).7/14/201745
Instrument Screening isUseful For: All children ages 1-3 years– Usually unable to perform visual acuityscreening Some children ages 3-5 years– Acuity chart screening is preferred, but – Instrument-based screening is an acceptablealternative. Older children who are non-verbal,developmentally delayed or otherwiseunable to perform screening with acuitycharts.7/14/201746
What is the DifferenceBetween Vision Screeningwith Eye Charts and VisionScreening with Devices? Vision screening with eye charts measurethe actual visual acuity (e.g. 20/20). Vision screening devices DO NOTmeasure visual acuity directly.– Screening instruments test for eye conditionsor risk factors that are known to causedecreased vision or amblyopia.7/14/201747
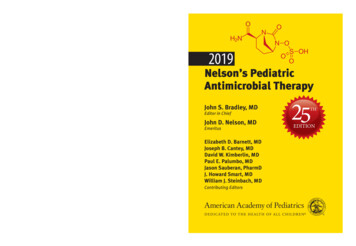
Common VisionScreening InstrumentsRighton RetinomaxiScreenWelch Allyn SureSightWelch Allyn“Spot”PlusOptix S12R7/14/201748
Acknowledgments These guidelines are based onrecommendations from the AmericanAcademy of Pediatrics (AAP) and theNational Expert Panel of the NationalCenter for Children’s Vision and EyeHealth (NCCVEH) at Prevent Blindness. These slides have been adapted from theAmerican Association for PediatricOphthalmology and Strabismus (AAPOS)with their permission.7/14/201749
References and Links Visual System Assessment in Infants, Childrenand Young Adults by Pediatricians– American Academy of Pediatrics Policy Statement– Pediatrics. January 2016. Volume 137. Issue 1 Procedures for the Evaluation of the VisualSystem by Pediatricians– American Academy of Pediatrics Clinical Report– Pediatrics. January 2016. Volume 137. Issue 17/14/201750
References and Links Bright Future and Preventative Medicine Coding Fact Sheet– American Academy of Pediatrics– AAP.org Professional Resources PracticeTransformation Coding at the AAP– Updated January 2016 Vision Screening for Children 36 to 72 Months:Recommended Practices– National Expert Panel to the National Center forChildren’s Vision and Eye Health– Optometry and Vision Science. January 2015.Volume 92. No. 1– CHDP 2016 Vision Health Assessment Guidelines7/14/201751
Parent believes child has vision problem. 7/14/2017 41 New AAP Guidelines: Age-Dependent Referral. Criteria 3 years old: Missing 3 or more symbols on the 20/50 line, or any line above the 20/50 line, with either eye 4 years old: Missing 3 or more symbols on the 20/40 line, or any line above the 20/40 line, with either eye 5 years and older: Missing 3 or more symbols on the 20/32 .