Transcription
The Basics of Positioning Patientsin Surgery
Objectives1. Describe the most commonly usedsurgical positions.2. State techniques for preventinginjury to surgical patients.3. Describe collaborative process forpositioning patients.
Introduction When our patients enter the surgicalsuite their safety and well-being are inthe hands of the perioperative team. Itis our responsibility to ensure each andevery patient is positioned correctly forhis/her procedure This education is being implemented tocreate a safe environment for ourpatients and staff
Intraoperative Positioning Policy OPER P-04Applies to: Downtown and Community Campuses RNs, anesthesiologists, surgeons, residents, surgicaltechnologists, medical students, NPs, PAs, CRNAs, anesthesiatechs Corresponding Procedures PROC OPER P-04A - Lateral PositioningPROC OPER P-04B - Lithotomy PositioningPROC OPER P-04C - Prone PositioningPROC OPER P-04D - Supine PositioningPROC OPER P-04E - Trendelenburg/Reverse Trendelenburg Positioning
Goals of PositioningProviding adequate exposureMaintaining patient dignityOptimal ventilation & airway managementProviding adequate accessAvoiding poor perfusionProtecting fingers, toes, genitalsProtecting muscles, nerves, bony prominences
Positioning Injuries General/Regional anesthesia– Physiologic changes– Reduced movement/sensation
Positioning InjuriesPressure Force placed onunderlying tissueShear Folding of underlyingtissueFriction Force of two surfacesrubbing against oneanother
Positioning InjuriesMoistureHeat Produces maceration Increases MetabolismColdNegativity Reduces O2 delivery Increases Pressure
Positioning InjuriesNerves Stretching or compression Transient or permanent damageMost common sites Brachial plexus Peroneal Facial
Positioning Injuries Brachial plexus– Shoulder– Arm– Hand
Positioning Injuries Brachial plexus injury due to:– Arm boards extended beyond90 degrees– Arm boards higher or lower thanthe OR bed– Lateral rotation of the patient’s head– Leaning against the shoulder or arm– Shoulder braces
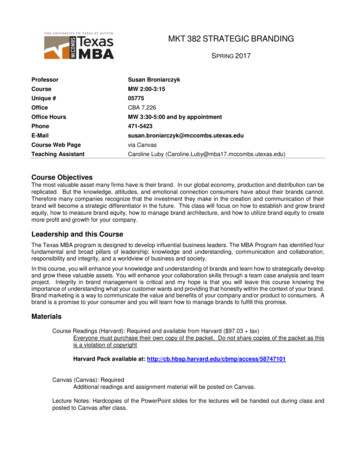
Positioning Injuries Common peroneal–Lower leg–Foot–ToesSciaticCommon PeronealTibial
Positioning Injuries Common peroneal injury dueto:– Direct compression– Patients who are thin– Hyperextension of knees– Pressure behind knee– Graduated compression stockings too tight– Foot drop/Lower-extremity paresthesia
Positioning InjuriesPulmonary HypoxiaRespiratory compromiseDecreased O2 saturationPulmonary edemaCongestionAtelectasis
Positioning InjuriesOcular Corneal abrasion Central retinal artery occlusionRisk factors Prone Length of procedure Blood loss
Increased Risk for PositioningInjuriesObese or underweightPoor nutritional statusAdvanced age ( 70 years)Preexisting conditionsHistory of skin breakdown/pressure ulcersSmoking (vasoconstriction)
Positioning Process Collaborative process– Selection of equipment– Preoperative assessment– Positioning– Documentation– Postoperativeevaluation
Preoperative Assessment Age/Height/Weight/Body mass index (BMI)Nutritional statusBlood pressureSkin integrityROM/Physical limitationsInternal/External devicesPreexisting conditionsMedical historyDiagnostic studiesPsychological/Cultural considerationsLength of surgery
Selection of EquipmentInspectedandmaintainedCheckedprior toprocedureCompetentsurgicalpersonnel
Selection of Equipment Pressure relieving surface– Disperses weight– Prevents “bottoming out”– Relieves shear andfriction
Selection of everseTrendelenburg
Positioning Check Assess the patient:– Body alignment, tissue perfusion, andskin integrity– Checking pressure points duringsurgery, is especially important incases that are greater than 2 hours.This is always dependent on theability to access the patient withoutcompromising the surgical procedureor sterile field.
Safety Care should be taken to prevent laying ofinstruments and power cords on the patientduring the case. Scrubbed members of the surgical team shouldnot lean against the patient during surgery.
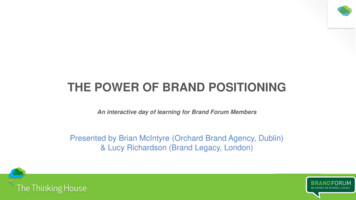
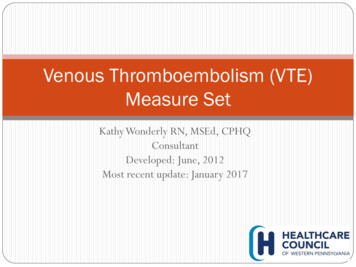
Supine Most commonly used surgical posi;on Common injuries related to the supineposi;on are pressure ulcers on theocciput, scapulae, thoracic vertebrae,elbows, sacrum, and heels Arms should either be secured at thesides or extended on arm boards Safety strap should be placed acrossthe thighs, approximately 2 inchesabove the knees with a sheet orblanket placed between the strap andthe pa;ent’s skin Pa;ent's heels should be elevated offthe underlying surface when possible
Supine
Supine
Trendelenburg
Reverse Trendelenburg
Sitting/Modified-Sitting
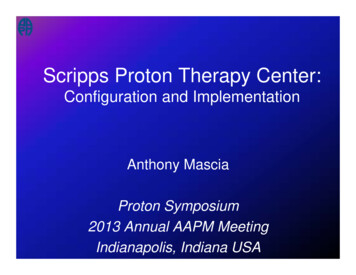
LowHighStandardExaggeratedHemiLithotomy
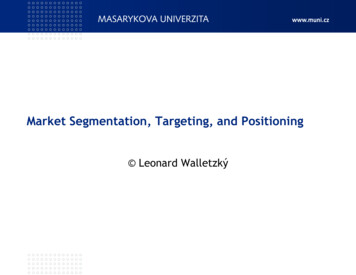
Lithotomy
LithotomyCommon peronealFemoralObturator
Prone
Prone
Jackknife
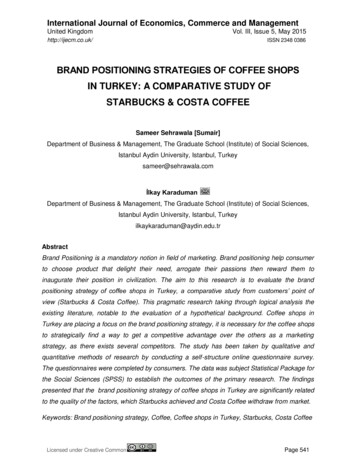
Lateral
Lateral
Obese yIssuesSkin Issues Type II diabetes HTN Artherosclerosis Sleep apnea Airway compromise Difficult intuba;on Aspira;on Hypoxia Intra-abdominal pressure Increased cardiac output Increased pressure on pulmonary artery Risk of inferior vena cava compression Difficult assessments Skin breakdown Moisture
Obese PatientsSpecialEquipmentPosi;on Procedure bedsExtra-wide/long safety strapsSide aRachmentsPressure relieving surfaces SiSng/Modified-siSng Lateral Supine with wedge under right side
Robotic Positioning– Prior to draping, the patient’s positioning should be testedfor sliding, limb impingement, respiratory and circulatoryproblems.– Periodic checks throughout the procedure to assess forpositional shifts are required. This is always dependent onthe ability to access the patient without compromising thesurgical procedure or sterile field.– After the team docks the robot and periodically throughoutthe procedure, safety checks should be performed to ensureproper positioning of the robotic arms and that they are notin contact with the patient.– Eye goggles can be used to protect the eyes from therobotic arms, if they are going to be in close proximity tothe face.
Documentation Preoperative assessmentNames/titles of participantsPatient positionUpper extremitiesLower extremitiesEquipment/PaddingSpecific actionsPositioning checksRepositioningPostoperative assessment
Postoperative Assessment Nerve injury Pressure injury Reposition Transfer of care
References1. Guideline for positioning the patient. In:Guidelines for Perioperative Practice.Denver, CO: AORN, Inc; 2017.
Most commonly used surgical posi;on Common injuries related to the supine posi;on are pressure ulcers on the occiput, scapulae, thoracic vertebrae, elbows, sacrum, and heels Arms should either be secured at the sides or extended on arm boards Safety strap should be placed across the thighs, approximately 2 inches