Transcription
·:{iC0Fp'16ACOFP 53rd Annual Convention & Scientific SeminarsThe Patient Centered Medical HomeRebecca Moore, DO
ACOFP FULL DISCLOSURE FOR CME ACTIVITIESPlease check where applicable and sign below. Provide additional pages as necessary.Name of CME Activity: ACOFP 53rd Annual Convention and Scientific SeminarsDates and Location of CME Activity: April 6-9, 2016, The San Juan Puerto Rico Convention CenterYour presentation: Saturday, April 9, 2016: 7:00am-9:00am: Medicare Wellness, Transition Codes and Patient Centered Medical HomeName of Faculty/Moderator: Rebecca Moore DODISCLOSURE OF FINANCIAL RELATIONSHIPS WITHIN 12 MONTHS OF DATE OF THIS FORMXA. Neither I nor any member of my immediate family has a financial relationship or interest with any proprietary entity producinghealth care goods or services.B. I have, or an immediate family member has, a financial relationship or interest with a proprietary entity producing health caregoods or services. Please check the relationship(s) that applies.Research GrantsStock/Bond Holdings (excluding mutual funds)Speakers’ Bureaus*EmploymentOwnershipPartnershipConsultant for FeeOthers, please list:Please indicate the name(s) of the organization(s) with which you have a financial relationship or interest, and the specific clinical area(s)that correspond to the relationship(s). If more than four relationships, please list on separate piece of paper:Organization With Which Relationship ExistsClinical Area Involved1.1.2.2.3.3.4.4.*If you checked “Speakers’ Bureaus” in item B, please continue: Did you participate in company-provided speaker training related to your proposed Topic? Did you travel to participate in this training? Did the company provide you with slides of the presentation in which you were trained as a speaker? Did the company pay the travel/lodging/other expenses? Did you receive an honorarium or consulting fee for participating in this training? Have you received any other type of compensation from the company? Please specify: When serving as faculty for ACOFP, will you use slides provided by a proprietary entity for your presentationand/or lecture handout materials? Will your Topic1 involve information or data obtained from commercial speaker :Yes:Yes:No:No:DISCLOSURE OF UNLABELED/INVESTIGATIONAL USES OF PRODUCTSX A. The content of my material(s)/presentation(s) in this CME activity will not include discussion of unapproved orinvestigational uses of products or devices.B. The content of my material(s)/presentation in this CME activity will include discussion of unapproved or investigationaluses of products or devices as indicated below:I have read the ACOFP policy on full disclosure. If I have indicated a financial relationship or interest, I understand that thisinformation will be reviewed to determine whether a conflict of interest may exist, and I may be asked to provide additionalinformation. I understand that failure or refusal to disclose, false disclosure, or inability to resolve conflicts will requirethe ACOFP to identify a replacement.Signature:Rebeccca Moore DODate:Rebecca Moore, DOPlease email this form to joank@acofp.org as soon as possibleDeadline: Friday, January 15, 201612/22/15
3/17/2016The Patient CenteredMedical Home(2014 Standards)Rebecca Moore DOAssociate ProfessorFamily MedicineRowan SOMDisclosures NONEObjectives Review the background behind the PatientCentered Medical HomeReview how to become PCMH recognizedReview the standards to achieve PCMH statusDiscuss the benefits of a PCMH model1
3/17/2016Background NCQA developed the PCMH model to helpimprove patient careCollaboration between the the American College ofPhysicians, the American Academy of FamilyPhysicians, the American Academy of Pediatricsand the American Osteopathic AssociationDeveloped a set of standards to help give practicesinformation about organizing care around patients,working in teams and coordinating and trackingcare over time.The standards encourage the use of electronichealth recordsThe standards align themselves with theinformation technology similar to that required tomeet CMS Meaningful Use RequirementsFocus is on patient - centeredness AND the abilityto track care over time and across settingsHow are PCMH 2015 StandardsDifferent for 2011? More integration of behavioral healthcare Additional emphasis on team - based care Focus care management for high-need populations Encourage involvement of patient and families in QI activities Alignment of QI activities with the Triple Aim improved quality, cost and experience of careAlignment with health information technology Meaningful Use Stage 22
3/17/2016ACP PositionPaper –The PCMH-NWho is eligible to participate in aPCMH? Clinicians who hold a curent, unrestricted license as a MD, DO, APRN, or PAOnly clinicians that a patient/family can select as aPersonal Clinician are eligibleThe practice defines a “personal clinician” as A residency group under a supervising clinician orfaculty physician, although residents themselvesare not identified individually for selection aspersonal cliniciansA combination physician and APRN or PA whoshare a panel of patients3
3/17/2016 Physicians, APRN and PA’s who practice in thespecialty of internal medicine, family medicine orpediatrics with the intention of serving as apersonal clinician for their patients.Physician-led practices applying with identifiedAPRNs or Pas: Patients may choose the APRN or PA as theirPCP orARPNs or PAs share a panel of patients as aprimary care team with the physicianClinicians who do not qualify: Non-primary care specialty clinicians and APRNsand PAs who do not have a panel of patientsSpecial Circumstances Practices that do not have a physician with apanel of patient at the site may achieve NCQARecognition with the following considerations: It is allowed according to the scope ofpractice determined by state law Practices are reviewed against the samerequirements as physician-lead practices4
3/17/2016What about practices withmultiple sites? Organization must have at least three sitesshare an electronic record systemstandardized policies and procedures acrossall practice sitesYou and/or your practice are eligibleto apply for PMH recognition.Now what?5
3/17/2016PCMH 1: Enhanceaccess and ContinuityElement A: Patient-CenteredAccess** Provide same - appointments for routine and urgent care(Critical factor)Provide routine and urgent-care appointments outsideregular business hoursProvided alternative types of clinical encountersAvailability of appointmentsMonitoring no-show ratesActing on identified opportunities to improve access6
3/17/2016Element B: 24/7 Access toClinical Advice Providing continuity of medical record informationfor care and advice when the office is closedProviding timely clinical advice by telephone whenthe office is not open (Critical Factor)Providing timely clinical advice using a secure,interactive electronic system when the office is notopenDocumenting after-hours clinical advice in patientrecordsElement C: Electronic Access More than 50 percent of patients have online access to their health informationwithin four business days of when the information is available to the office includes problem list, diagnosis, diagnostic test results, allergies, med listMore than 5 percent of patients view, and are provided the capability to downloadtheir health information or transmit their health information to a third partyClinical summaries are provided within 1 business day for more than 50% ofoffice visitsA secure message was sent to more than 5% of patientsPatients have two-way communication with the practicePatients can request appointments, prescription refills, referrals and test resultsPCMH 2: Team-BasedCare7
3/17/2016Element A: Continuity Assisting patients/families to select a personal clinician anddocumenting the selection in practice recordsMonitoring the percentage of patient visits with a selectclinician or teamHaving a process to orient new patients to the practiceCollaborating with the patient/family to develop/implement awritten care plan for transition from pediatric care to adultcareElement B: Medical HomeResponsibilities The practice is responsible for coordinating patient care across multiplesettingsInstructions on obtaining care and clinical advice during office hours andwhen the office is closedThe practice functions most effectively as a medical home if patientsprovide a complete medical history and information about care obtainedoutside the practiceThe care team gives the patient/family access to evidence-based care andself-management supportThe scope of services available within the practice including howbehavioral health needs are addressed The practice provides equal access to all of theirpenitents regardless of source of payment The practice gives uninsured patients informationabout obtaining coverage Instructions on transferring records to the practice,including a point of contact at the practice8
3/17/2016Element C: Culturally andLinguistically Appropriate Services Assessing the diversity of its populationAssessing the language needs of its populationProviding interpretation or bilingual services tomeet the language needs of its populationProviding printed materials in the languages of itspopulationElement D: The PracticeTeam** Defining roles for clinical and nonclinical team members Identifying the team structure and the staff who lead andsustain team based care. Holding scheduled patient careteam meetings or a stretch communication process focusedon individual patient care. (Critical factor) Using standing orders for services Training and assigning members of the care team tocoordinate care for individual patients. Training and assigning member so of the care team tosupport patients/families/caregivers in selfmanagement, self-efficiency and behavior change.Training assigning members of the care team tomanagement eh patient populations.Holding scheduled team meetings to address practicefunctioning.Involving care team staff in the practice’s performanceevaluation and quality improvement activities.Involving patients/families caregivers in qualityimprovement activities or on the practice’s advisorycouncil.9
3/17/2016PCMH 3: Identify andManage Patient PopulationsElement A: PatientInformation Date of numbersEmail address OccupationDates of previous clinical visitsLegal guardian/health care proxyPrimary caregiverPresence of advance directions(NA for pediatric practices)Health insurance informationName and contact information ofother health care professionalsinvolved in patient’s careElement B: Clinical Data An up-to-date problem list with current and activediagnoses for more than 80% of patientsAllergies for more than 80% of patients (includemedications allergies and adverse reactions)Blood pressure with the date of update for morethan 80% for patients 3 yrs and olderHeight/length for more than 80% of patientsWeight for more than 80% of patients10
3/17/2016 System calculates and displays BMI (NA for pediatricpractices)System plots and displays growth charts and BMI percentilefor ages 0-20 years (NA for adult practices)Status of tobacco use for patients 13 years and older formore than 80% of patientsList of prescription medications with the date of updates formore than 80% of patientsMore than 20% of patients have family history recorded asstructured dataAt least one electronic progress note created, edited andsigned by an eligible professional for more than 30%Element C: ComprehensiveHealth Assessment Documentation of age and gender appropriateimmunizations and screeningsFamily/social/cultural characteristicsCommunication needsMedical history of patient and familyAdvance care planning (NA for pediatric practices)Behaviors affecting healthPatient and family mental health/substance abuseDevelopmental screening using a standardized tool(NA for adult-only practices)Depression screening for adults and adolescentsusing a standardized tool.Assessment of health literacy11
3/17/2016Element D: Use Data forPopulation Management** At least two different preventive care servicesAt least two different immunizationsAt least three different chronic or acute careservicesPatients not recently seen by the practiceMedication monitoring or alertElement E: Implement EvidenceBased Decision Support A mental health or substance use disorder (Critical Factor) A chronic medical condition An acute condition A condition related to unhealthy behaviors Well child or adult care Overuse/appropriateness issuesPCMH 4: CareManagement and Support12
3/17/2016Element A: Identify Patients forCare Management Behavioral health conditionsHigh cost/high utilizationPoorly controlled or complex conditionsSocial determinants of healthReferrals by outside organizations (ex: insurers, healthsystem, ACO), practice staff or patient/family/caregiverThe practice monitors the percentage of the total patientpopulation identified through its process and criteria (CriticalFactor)Element B: Care Planning andSelf-Care Support** Incorporates patient preferences andfunctional/lifestyle goalsIdentifies treatment goalsAssesses and addresses potential barriers tomeeting goalsIncludes a self-management planIs provided in writing to the patient/family/caregiverElement C: MedicationManagement Reviews and reconciles medications with patients/families for more than50% of care transitions (Critical Factor)Reviews and reconciles medications with patients/families for more than80% of care transitionsProvides information about new prescriptions to more than 80% ofpatients/familiesAssesses patient/family understanding of medications for more than 50%of patients with date of assessmentAssesses patient response to medications ad barriers to adherence formore than 50% of patients with date of assessmentDocuments over-the-counter medications, herbal therapies andsupplements for more than 50% of patients/families, with the date ofupdates13
3/17/2016Element D: Use ElectronicPrescribing More than 50% of eligible prescriptions written by thepractice are compared to the drug formularies andelectronically sent to pharmacies.Enters electronic medication orders into the medical recordfor more than 60% of patientsPerforms patient-specific checks for drug-drug and drugallergy interactionsAlerts prescribers to generic alternativesElement E: Support Self-Careand Shared Decision Making Uses an EHR to identify patient-specific education resources and providethem to more than 10% of patientsProvides educational materials and resources to patientsProvides self-management tools to record self-care resultsAdopts shared decision making aidsOffers or refers patients to structured health education programs, such asgroup classes and peer supportMaintains a current resource list on five topics or key community serviceareas of importance to the patient population including services offeredoutside the practice and its affiliatesAssess usefulness of identified community resourcesPCMH 5: Care Coordinationand Care Transitions14
3/17/2016Element A: Test Tracking andFollow-Up Tacks lab tests until results are available, flagging and following up onoverdue results (Critical Factor) Tracks imaging tests until results are available, flagging and following upon overdue results (Critical Factor) Flags abnormal lab results, bringing them to the attention of the clinicianFlags abnormal imaging results, bringing them to the attention of theclinician Notifies patients/families of normal and abnormal lab and imaging testresults Follows up with the inpatient facilities about newborn hearing and bloodspot screening (NA for adults) More than 30% of radiology orders areelectronically recorded in the patient recordMore than 30% of radiology orders areelectronically recorded in the patient recordElectronically incorporates more than 55% of allclinical lab test results into structured fields inmedical recordMore than 10% of scans and tests that result in animage are accessible electronicallyElement B: Referral Trackingand Follow Up ** Considers available performance information onconsultants/specialist when making referralrecommendationsMaintains formal and informal agreements with a subsetof specialist based on established criteriaMaintains agreements with behavioral healthcareprovidersIntegrates behavioral healthcare providers within thepractice siteGives the consultant or specialist the clinical question, therequired timing and the type of referral15
3/17/2016 Give the consultant or specialist pertinent demographic andclinical data, including test results and the current care plan Has the capacity for electronic exchange of key clinicalinformation and provides the electronic summary of carerecord to another provider for more than 50% of referrals Tracks referrals until the consultant or specialist’s report isavailable, flagging and following up on overdue reports.(Critical Factor) Documents co-management arrangements in te patient’smedical records Asks patients/families about self-referrals and requestingreports from clinicians.Element C: Coordinate Careand Transitions Proactively identifies patients with unplanned hospitaladmissions and emergency department visitShares clinical information with admitting hospitals andemergency departmentsConsistently obtains patient discharge summaries fromthe hospital and other facilitiesProactively contacts patients/families for appropriatefollow-up care within an appropriate period following ahospital admission or emergency department visitsExchanges patient information with the hospitalduring a patient’s hospitalizationObtains proper consent for release of informationand has a process for secure exchange ofinformation and for coordination of care withcommunity partners,Exchanges key clinical information with facilitiesand provides an electronic summary-of-care recordto another care facility for more than 50% oftransitions of care16
3/17/2016PCMH 6: Performance Measurementand Quality ImprovementElement A: MeasurePerformance At least two immunization measuresAt least two preventive care measuresAt least three chronic and acute are clinicalmeasuresPerformance data stratified for vulnerablepopulations (to assess disparities in care)Element B: Measure ResourceUse and Care Coordination At least two measures related to care coordination At least two utilization measures affecting health carecosts17
3/17/2016Element C: MeasurePatient/Family Experience The practice conducts a survey (using any instrument) to evaluatepatient/family experiences on at least three of the following categories: AccessCommunicationCoordinationWhole-person care/self-management supportThe practice uses the PCMH version of the CAHPS Clinician and GroupSurvey Tool The practice obtains feedback on the experiences of vulnerable patientgroups The practice obtains feedback from patients/families through qualitativemeansElement D: Implement ContinuousQuality Improvement** Set goals and act to improve performance on at least three measures formElement A Act to improve at least three clinical quality measures from Element ASet goals and analyze at least one measure from Element BAct to improve at least one measure from Element BSet goals and analyze at least one patient experience measure fromElement C Act to improve at least one patient experience measure from Element CSet goals and address at least one identified disparity in care/service foridentified vulnerable populationsElement E: DemonstrateContinuous Quality Improvement Measuring the effectiveness of the actions it takesto improve the measures selected in Element DAchieving improved performance on at least twoclinical quality measuresAchieving improved performance on oneutilization or care coordination measuresAchieving improved performance on at least onepatient experience measure18
3/17/2016Element F: Report Performance Individual clinician performance results with thepracticePractice-level performance results with thepracticeIndividual clinician or practice-level performanceresults publiclyIndividual clinician or practice-level performanceresults with patientsElement G: Use Certified EHRTechnology The practice uses an EHR system (or modules) that has beencertified and issued a CMS certification IDThe practice conducts a security risk analysis of its EHS system andimplementing security updates as necessary and correction identifiedsecurity deficienciesThe practice demonstrates the capability to submit electronicsyndromic surveillance data to public health agency electronicallyThe practice demonstrates the capability to identify and report cancercases to a pu bloc health central cancer registry electronicallyThe practice demonstrates the capability to identify and reportspecific cases to a a specialized registry (other than a cancerregistry) electronically The practice reports clinic quality measures to Medicare and medicaidagency, as required for Meaningful Use The practice demonstrates the capability to su bit data to immunizationregistries or immunization information systems electronically Then practice has access to a health information exchange The practice has bidirectional exchange with a health informationexchange The practice generates lists of patients,, and based on their preferredmethod of communication, proactively reminds more than 10% ofpatients/families/caregivers about needed preventive/follow-up care THIS ELEMENT IS NOT SCORED, BUT REQUIRED19
3/17/2016How do I show thedocumentation? The guidelines and survey tool suggest theappropriate way to attestMay be by screen shotsMay be percentagesEach element may have different timelinesrequired one month vs three month vs six monthsHow do you apply for PCMH? Go to NCQA website and order the PCMH online application Address the PCMH online application system and order aPCMH survey tool dex.htmYou will receive email confirmation from NCQAone survey tool per locationSign the program agreement and Business AssociateAgreementSubmit the online applications to NCQASubmit the application fee to NCQAWhat’s next? Complete the survey toolRespond to the questionsComplete the worksheets providedAttach the required documentationSubmit20
3/17/2016Why is the survey tool soimportant? It helps break down the requirements into theseparate standards and elementsHelps track the requirements neededHelps add up your pointsCan you upgrade after you have alreadybeen recognized for specific PCMH level? Yes you can!A practice that has Level 1 or 2 recognition statusmay apply for an Add-On Survey within the 3 yearrecognition period. Can move up to Level 2 or 3based on the points.So what are theBenefits?21
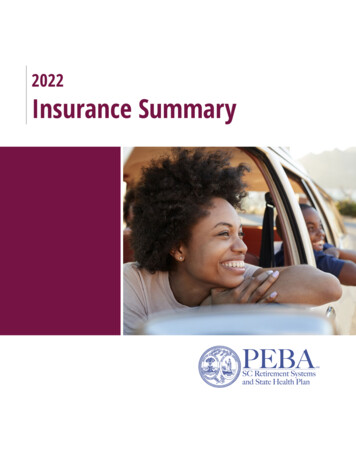
3/17/2016Blood Pressure Under Control LastTime Checked, by Medical HomeHas Heart Disease, Hypertension, and/or DiabetesPercentMedical homeNo medical home11388859082 84 82 797175 7884 RSWESWIZUKUSBase: Has heart disease, hypertension, and/or diabetes and blood pressure checked in past year.Source: 2011 Commonwealth Fund International Health Policy Survey of Sicker Adults in Eleven Countries.Rated Quality of Care in Past Year as “Excellent”or “Very Good,” by Medical HomePercentMedical homeNo medical home11390888379727772656862595646 49454460574438 : 2011 Commonwealth Fund International Health Policy Survey of Sicker Adults in Eleven Countries.Medical, Medication, or Lab Test Errorsin Past Two Years, by Medical HomePercent*Medical homeNo medical home383029272323231518151515 ESWIZUKUS* Reported medical mistake, medication error, and/or lab test error or delay in past two years.Source: 2011 Commonwealth Fund International Health Policy Survey of Sicker Adults in Eleven Countries.22
3/17/2016Doctor–Patient Relationship andCommunication, by Medical HomePercent reporting positive doctor–patientrelationship and communication*Medical home90No medical 18230AUSCANFRGERNETHNZNORSWESWIZUKUS* Regular doctor always/often: spends enough time with you, encourages you to ask questions,and explains things in a way that is easy to understand.Base: Has a regular doctor/place of care.Source: 2011 Commonwealth Fund International Health Policy Survey of Sicker Adults in Eleven Countries.Hospital or Surgery Discharge Gap inPast Two Years, by Medical HomePercent*Medical home9082666368605763No medical ERNETHNZNORSWESWIZUKUS* Last time hospitalized or had surgery, did NOT: 1) receive instructions about symptoms and when to seekfurther care; 2) know who to contact for questions about condition or treatment; 3) receive written plan for careafter discharge; 4) have arrangements made for follow-up visits; and/or 5) receive very clear instructions aboutwhat medicines you should be taking.Source: 2011 Commonwealth Fund International Health Policy Survey of Sicker Adults in Eleven Countries.There is Evidence. Early evidence suggests that PCMH improves thequality of care and returns savingsFields, Leshen, Patel 2010 - Article foundreduced use of the hospital, emergency roomvisits and overall savingsReid 2009 - Followed an integrated grouppractice and found significant improvement inpatient/provider experiences and in the quality ofclinical care23
3/17/2016The End Questions?24
The standards encourage the use of electronic health records The standards align themselves with the information technology similar to that required to meet CMS Meaningful Use Requirements Focus is on patient - centeredness AND the ability to track care over time and across settings. How are PCMH 2015 Standards Different for 2011?