Transcription
AESCULAP PATIENT INFORMATIONYOUR NEW ARTIFICIAL TOTAL KNEE JOINT
Dear Patient,The knee joint receives the most stress compared to otherjoints in the body. The natural structure of the knee jointenables a wide range of motion patterns. The knee jointfunction can be imparied by overloading, disease, and injurywhich lead to surgical implantation of an artificial kneereplacement.The implantation of a knee endoprosthesis is one of themost common orthopaedic surgical procedures.In the following pages, a summary was prepared of all theimportant information for every patient before and afterknee surgery. This brochure is intended as supplement tomedical advice and consultation with your physician, andhelp you find answers to questions about knee surgery.The medical professionals at your hospital will advise andprovide you with intensive care during the process, as wellas do everything they can to support you during this relevanttime and recovery process. Being well prepared, and havinga support system will help enable you to maximise recovery.
CONTENTSI The Knee Joint1. Knee structure and knee mechanics2. Reasons for knee replacement3. Diagnosis and conservative treatmentmethodsII Implants1. Development2. Anchorage options and materials3. Metal sensitivity4. The artificial knee joint5. Complete resurfacingIII The Surgical Intervention1. Preparation for surgery2. Important tools3. The day of admission to the hopsital4. The surgical procedureIV After the Surgery1. First steps2. Rehabilitation3. Follow-upsV Living with an artificial knee joint1. Daily life2. The implant passport3. Tips and tricks4. SportVI Materials and substances included in the deviceVII Aesculap AG - an introduction to the manufacturer
ITHE KNEE JOINTSTRUCTURE OF THE KNEE JOINTThe knee joint, along with its ligaments and muscles, is the largest joint in the human body. It allows us to stand, remainupright, and above all it allows us to walk. Our knees ensure our ability to move and provide us with stability.1. Knee structure and knee mechanicsKnee StructureKnee MechanicsThe knee joint is formed by the mobile connection betweenthe lower leg (tibia) and the thigh (femur). In a healthy knee,both the femur and tibia joint are surrounded by a layer ofcartilage that acts as a bearing or articulating surface. Inaddition, the outside and inside edges of the tibia plateaucontain a crescent shaped menisci that are made of cartilage.The articulating surface of the joint absorbs pressure in thejoint, and protects the joint surfaces of both femur and tibia.Joint fluid is found in the joint space and acts as a lubricantto help reduce friction on the articulating surface of jointsduring movements. Joint fluid ensures the various partsof the knee work together. If any part of the knee joint isaffected by disease, the entire system will be affected.The stability of the knee joint is the result of a complexsystem of ligaments. There are both medial and lateralligaments that provide stability for the knee joint. Anadditional source of stabilisation include the anterior andthe posterior cruciate ligaments. The joint also includes theknee cap (Patella), which is a bone encased in the tendonwhich connects to the quadriceps muscle. The knee capstabilises the knee joint from the front during movement.The knee joint has a sliding joint axis that can be moved infive different directions. This essentially means rolling andsliding movements of the femur over the tibia. For example,when the knee is bent, slight outward and inward rotationsare made possible. When the knee is fully extended, thesemovements are blocked by the ligaments for stability.
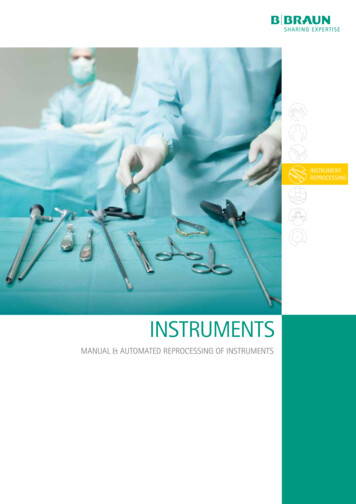
The right knee joint from the front1. Femur2. Femoral condyles with cartilage coverage13. Posterior cruciate ligament (PCL)4. Lateral meniscus5. Anterior cruciate ligament ACL)6. Medial meniscus227. Lateral collateral ligament38. Medial collateral ligament57469. Patellar tendon1010. Tibial plateau with cartilage coverage89The patella is not shown for clear view of illustration
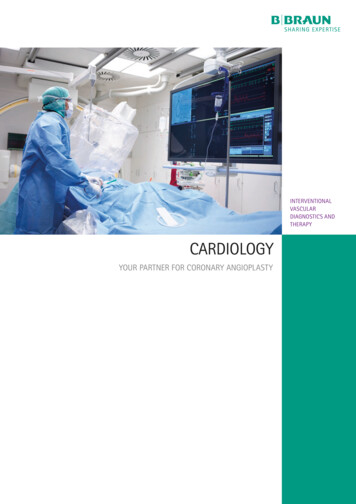
Osteoarthritis of the knee jointFront ViewFrontal View of Right Knee2. Reasons for knee replacementNowadays, knee replacement is one of the most commonsurgical orthopaedic procedures being performed, and isconsidered a standard procedure.The knee joint is under great daily stress since it bears theweight of the entire body. Therefore, an intact cartilage layeron the femoral condyles and tibial plateau is required forsmooth and pain-free movement in the knee joint.Several factors can lead to the erosion of or damage to theprotective cartilage layer:Pronounced bow-leggedness can lead to the developmentof osteoarthritis of the medial joint spaceFrontal View of KneeThe joint space hasnarrowed, because thecartilage has worn away.This causes the bones,femur condyles and tibiaplateau, to be pushedtogether.Side view of kneeWear affects not only thefemoral condyles and thetibia plateau, the dorsal(backside) surface of thepatella will also experiencewear.Pain associated with wear and tear of the knee joint, known asosteoarthritis, is the most common and frequently occuringcondition. Osteoarthritis can be a result of age related wearof the joint, which can lead to pain and restricted movement.Other causes of wear include congenital or improper stressacquired with age as a result of leg deformation (bowleggedness or knock-knee), previous injuries, or inflammationin the knee joint. In many cases, knee osteoarthritis willinitially lead to damage of the cartilage menisci, which isthen no longer able to sufficiently protect the joint surfacesfrom the pressure of the body weight. As a consequence, thejoint surfaces of the femoral condyles and the tibial plateau
are subsequently affected. The protective cartilage layerbegins to erode at the point of greatest stress, until it iscompletely worn away and the bone is exposed. Sincecartilage is not supported by blood vessels, this is incontrast to numerous other body tissues. This means ithas a low capacity to heal itself after injuries or diseaserelated disorders. Once the cartilage is worn away, the jointcartilage will not grow back. Therefore, any movement in thejoint will be painful. In such cases, the synovial membraneproduces a large amount in the tissue, which is only slightlylubricating, and leads to join effusion or water in the knee.As a result, the patient will experience severe pain.An artificial knee replacement will be necessary if the kneewas damaged to the extent that joint-preserving surgery isno longer an option.3. Diagnosis and conservative treatment methodIn a current clinical scenario, surgeons use X-ray imaging,which illustrates the condition of the bone, as well asvarious clinical evaluation methods to learn restrictions inthe knee joint during natural movement.Wear and tear of the knee joint manifests itself through painwhile walking and in situations of stress on the joint. As aresult of this pain, a person suffering from this condition willoften adopt an adaptive posture, which leads to abnormalstress and changes to the muscle and tendon structures.At first, joint replacement can be avoided through a targetedconservative treatment process. Initially, medications maybe prescribed to alleviate pain, and then next throughtherapeutic excercise or physical therapy to treat currentlimitations in movement. However, the pain often reachesa level where daily activity is affected to the point wherethe quality of life is significantly reduced, and disruption insleep also occurs.After surgery, following preparations will be made at thehopsital: ConsultationsDate of SurgeryAppointment for X-raysSelection and review of suitable prosthesisPre-operative planning and sizing based on X-rays
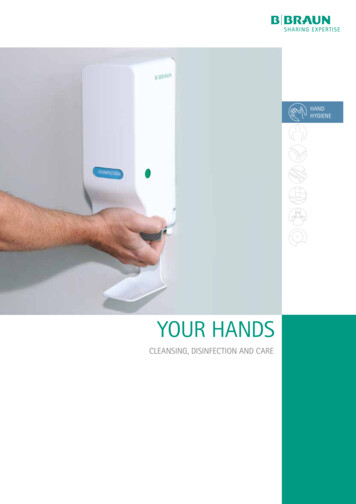
IIIMPLANTSARTIFICIAL KNEE JOINTSThe artificial knee joints replaces the worn parts of the kneejoint and has a similar form to the human knee.In general, there are two classic types of knee resurfacingtreatments, which are known as mobile bearing and fixedbearing knee implant systems. The technical differencebetween the two systems is the movement of the bearing(meniscus replacement) between the femoral and tibialcomponents.The mobile bearing can rotate on the metal plate of thetibial components. In contrast, in a fixed bearing system, theartificial bearing is firmly clicked into the metal componentsand is therefore fixed.Both types have proven valuable in recent decades and havebeen proven equally reliable and functional. Both systemsoffer good mobility, allow the knee to be bent to a significantdegree, and offer sufficient stability.Depending on the extent to which the knee joint has beendamaged by osteoarthritis, different types of prosthesis canbe considered.The following illustrates the different types of resurfacingknee prostheses:Unicondylar (left), Total Knee Replacement (middle) HingedKnee Replacement (right)More than one part of the knee joint (medial and lateral)are damaged by osteoarthritis and must be replaced. Thecollateral ligaments are completely preserved.During resurfacing of both the sides of the knee, a metalprosthesis caps the natural femoral condyles. The prothesisis made to mirror the natural geometry of the femoralcondyles. The tibia is also capped with a metal prosthesisand an artificial meniscus as the bearing surface.The anterior curciate ligamant is removed during theoperation. In addition, there are prosthesis variants thattake on the function of the posterior cruciate ligament aswell. Your surgeon will decide which option is preferredbased on the present situation.
COLUMBUS TOTAL KNEE REPLACEMENTThe Columbus knee arthroplasty system is a bicondylar jointsurface replacement with a fixed or rotating gliding surfacefor primary treatment. It also includes revision componentsfor use in revision surgery.The Columbus knee endoprosthesis comprises of a CoCrMofemur and tibia component, as well as a UHMWPE meniscuscomponent. Metal components can be cemented orcementless with Plasmapore . All the CoCrMo componentsfor cemented application are also available in the AS(Advanced Surface) version for people with metal allergies.A gold colored Advanced Surface (AS) made from Zirconiumnitride is applied to the standard implant through a physicalvapor process. A total of seven layers are applied to seal themetallic parts of the implant components.Where required, a UHMWPE patella replacement can also beimplanted. There is a left and right knee version for all femurcomponents.
COLUMBUS TOTAL KNEE REPLACEMENTMetal components are manufactured from CoCrMo alloyaccording to ISO 5832-4 or ISO 5832-12.Cementless femur and tibia componentsThe inner surfaces of the cementless femur and tibiacomponents have an additional coating of a porous puretitanium (Ti) layer (PLASMAPORE ) in conformance with ISO5832-2.Cemented femur and tibia componentsThe inner surfaces of the femur and tibia components aremechanically roughened for cement/implant adhesion.Cement pockets with a depth of 1 mm are provided on thecementing surfaces of the femur and tibia components.DDAS TechnologyUCPSThe meniscus components and patella are made fromPolyethylene (UHMWPE) according to ISO 5834-2. Itincludes X-Ray markers made of Stainless steel accordingto ISO 5832-1 (Patella), Tantalum according to ASTM F560or ISO 13782 (meniscal components) and Titanium alloyaccording to ISO 5832-3 (meniscal components).Patella
IIITHE SURGICAL INTERVENTION1. Preparation for the surgeryPersonal necessities:AllergiesToiletriesInform your surgeon in advance prior to your surgery ofany known allergies. It is important to inform your doctorabout all allergies which include, but are not limited to drugreactions, synthetic substances, and metal allergies.PyjamasOther illnessesTrainers and slippersIf you are receiving medical treatment for other illnesses,you should inform your surgeon prior to the operation.This will insure the surgical team can make all necessaryarrangements in advance of your treatment.AnaestheticIn addition to a general anaesthetic, there is also generallythe possibility that a local anaesthetic (Spinal anaesthetic)or peripheral nerve block ("pain catheter“) may beadministered. The decision as to which form will be used,will be determined by the anesthesiologist in charge, andwill generally be based on any concomitant diseases.Bath robeCasual ClothesFlat, non-slip shoesRequired medicationsBooks, magazinesContact details of family and friendsSmall amount of cashClinic requirements:X-raysExamination fileReferralsHealth insurance cardAllergy record2. Important toolsWhen someone is admitted to the hospital, the questionof what is needed for the hospital stay always arises. Thefollowing list may help when preparing for your stay.Detailed list of medications including dosages,quantity, and times of medication administrationImplant passport of prior operations (e.g. hipoperations or heart pacemakers
3. The day of admission to the hospitalGenerally, a patient is admitted to the hospital on the dayof the operation. After your personal information has beenrecorded. You will be taken to the ward. The anesthesiologistwill discuss the anesthesia with you and confirm if you aretaking other medications, or have any other illnesses. Thenurses and caregivers will be there to answer any otherquestions.4. The surgical procedureunder the skin will be gently moved aside and the knee jointwill be exposed. The damaged cartilage, misshappen bone,and the meniscus will then be removed.The surgical incision will always be made from the front,but there are various procedures with different skin incisionpoints and different soft tissue preparation. Less invasiveprocedures are becoming increasingly popular nowadays,as they preserve individual muscle and tendon structures.However, it is not the length of the visible skin incision thatis important, but rather the careful handling of the softtissue under the skin.Access to the jointAfter the anesthesia is administered, and preparations arecomplete, the knee to be operated on will be washed, and anincision will be made in the skin. The soft tissue and musclesUnder normal circumstances the surgery lasts between 6090 minutes depending on the individual case.
Course of the operationI. Preparation of the tibiaV. Preparation of the shaftfor the tibial implantII. Measurement andadjustment of the jointspaceVI. Implant of the finaltibia implantIII. Preparation of thefemurImplant of the final femurIV. Sample positioning ofthe size specific implantInsertion of the new bearing
Preparation and ImplantationI.II.The femur and tibia bone is prepared using the adaptedmolds to fit the prosthesis. For this purpose, the tibia isprepared with a saw at a right angle to the axis of theleg.Then, the joint space is measured, taking the soft tissue(joint capsule and ligaments) into consideration. Ifa shortening of the ligaments in the joint occured forexample, this can be corrected in order to make theknee joint more stable.III. The size of the femur will be determined, and it will beprepared for the prosthesis with a saw.IV. Once the implant bed is created accordingly, thecorrect fit and good mobility of the knee joint will betrialed and tested using sample prosthesis.V.After confirmation that the prosthesis is an exact fit,the anchoring points in the bone will be drilled or cut.VI. In the final step, the original prosthesis are positionedand fixed.The functionality of a new joint is then checked and theincision in the knee is gradually sutured. Tubes are insertedinto the wound to allow for wound drainage.
IVAFTER THE OPERATION1. First stepsGenerally, weight will be put on your new artificialjoint one or two days after the surgery, under theinstruction of medical personnal. At the hopsital, youwill learn to bend and stretch your joint again withthe help of a physiotherapist. You can make yourfirst attempt at walking with the help of crutches.Little by little, additional therapeutic measures willbe added and you will learn how to walk and thebest way to climb stairs and to sit down.2. RehabilitationAfter approximately 3-5 days, you will be dischargedfrom the hospital and in some cases moved torehabilitation, if available. The goal is for you togradually be able to put your weight on the artificialjoint and prepare you for normal daily activities andeveryday routine. Your mobility will be improvedthrough intensive excercise and your muscles builtup accordingly. The subsequent treatment can takeplace on either an outpatient or inpatient basis atthe rehabilitation facility. The nature and scope ofthe activities will be planned together by you andthe medical staff at the hospital.3. Follow-upsFollow-up visits should be held at regular intervalsto ensure long term success. In some instancesX-rays are used to access the integration of theprosthesis components in and to the bone, as wellas joint functionality.
VLIVING WITH AN ARTIFICIAL KNEE JOINT1. Daily Life2. Patient Implant CardThe long term success of the knee replacement is influencedby the follow-up care and your behaviour after the surgery.After the rehabilitation, you will return to regular daily lifewith all the normal stress on the joint. Approximately 6-8weeks after the operation, your muscles will be built upagain and be strong enough that you will contribute to thestability of the joint. You must therefore avoid putting a lotof stress on the prosthesis during this time.This is an important part of travel, especially at the securitygates in airports, as body scanners can detect metalcomponents in the body. The ID card states that you havean implant, it identifies and documents the componentsthat have been implanted in you through the attachedstickers. Your follow-up appointments are also recorded inthe document. Keep the ID card in a secure place or carry itwith you.Side Effects & RisksAs with any surgery, there are side effects and risks associated with the procedure which may include: Loosening, wear, and breakage of implant componentsMisalignment of jointsBony changes including bone lossJoint dislocationInfectionBlood clots in the leg or lungsHeart attacks or strokesAllergy reactions to the implantImplant fractureBlood vessel or nerve damageSkin or muscle sensitivity or scarringWound and bleeding complicationsJoint stiffnessLoss of knee mobility or functionality and/or inability to perform everyday physical tasks
3. Tips and tricks4. SportEven in the hopsital, you will learn how to use your jointagain with light physiotherapy exercises. Once you haveleft the hospital, exercises such as swimming (with freestyle or side stroke) or walking on a well-built path, shouldbecome habitual. You can even go for short bike rides (onflat terrain).Once the prosthesis components have been ingrown intothe bone, a high level of stability is achieved. However,an artificial joint is not like a natural joint so there arerestrictions, especially with sports. Sport activities arepositive in every respect, but "moderation“ should always beof paramount importance.You should avoid:Simple pushing movements, such as jumping from a higherlevel or jerky stress that occur in rapid, repetitive cycles orwhich require a wide range of movement should preferablybe avoided. Abrupt, jerky or impulsive movements Sports that require quick acceleration and suddenstops (tennis, alpine skiing, mounterring etc.) Excessive and long periods of standing Crossing your legs Extreme bending, eg. when crouching or kneeling Heavy and over-proportional weight gain Lifting heavy loadsRecommendations for making daily life easier: Good, flat and non-slip footwear Regular gait Shoes with velcro or elastic laces Removing tripping hazards, e.g. carpet edges,objects lying aroundSports that are suitable: CyclingSwimmingHikingNordic walkingCross-country skiingLight gym workDancing (standard or latin dancing)Sports that are less suitable: Ball games and team sports such as football,handball, basketball, etc.Martial artsSquashTennisAlpine skiing
The information given here is not a blanket recommendationand can vary from patient to patient. Your age, your sportingexperience and your general state of health affect the overallsituation. If you are unsure of which activities are suitable,please consult your doctor.With normal use and activity, a knee replacement can lastup to 10 years.Excessive activity or obesity may accelerate wear and couldcause knee replacement to loosen and become painful.By adopting the right lifestyle for you, there is no reasonwhy your knee should not provide you with a good qualityof life.
VIMATERIAL AND SUBSTANCES INCLUDED IN THE DEVICEComponentMaterialColumbus Femur CR cemented Cobalt chrome alloy (CoCrMo)Columbus AS Femur CRCementedColumbus Femur PSCementedColumbus AS femur PSCementedColumbus CR/PS TibiaCementedColumbus AS CR/PS TibiaCementedProduct CodeNN001K-NN911KCobalt chrome alloy (CoCrMo) withmultilayer coating system made fromchromium nitride-chromium carbonnitride-zirconium nitride (Crn-CrCN-ZrN)Cobalt chrome alloy (CoCrMo)NN001Z-NN911ZCobalt chrome alloy (CoCrMo) withmultilayer coating system made fromchromium nitride-chromium carbonnitride-zirconium nitride(CrN-CrCN-ZrN)Cobalt chrome alloy lt chrome alloy (CoCrMo) withNN070Z-NN079Zmultilayer coating system made fromchromium nitride-chromium carbonnitride-zirconium nitride (CrN-CrCN-ZrN)Cobalt chrome alloy (CoCrMo)NN470K - NN479KColumbus CRA/PSA TibiaCementedColumbus AS CRA/PSA Tibia Cobalt chrome alloy (CoCrMo) withNN471Z - NN479ZCementedmultilayer coating system made fromchromium nitride-chromium carbonnitride-zirconium nitride (CrN-CrCN-ZrN)SizeF1 - F8 and F2N F7NF1 - F8 and F2N F7NF1 - F8 and F2N F6NF1 - F7T0 - T5 andT0 - T4 T0 - T5 andT0 - T4 T0 - T5 andT0 - T4 T1 - T5 andT1 - T4
ComponentColumbus DD GlidingSurfaceColumbus UC GlidingSurfaceColumbus PS GlidingSurfaceFixation screw for PS Glidingsurface (AS)Patella 3-PEGColumbus Tibia StemsColumbus AS Tibia StemsColumbus ObturatorMaterialUltra-high, molecular low pressurepolyethylene acc. to ISO 5834-2Ultra-high, molecular low pressurepolyethylene acc. to ISO 5834-2Ultra-high, molecular low pressurepolyethylene acc. to ISO 5834-2Cobalt chrome alloy (CoCrMo) withmultilayer coating system made fromchromium nitride-chromium carbonnitride-zirconium nitride (CrN-CrCN-ZrN)Ultra-high ,molecular low pressurepolyethylene acc. to ISO 5834-2Cobalt chrome alloy (CoCrMo)Product CodeNN200 - NN255SizeT0/0 - T4/4 , T5NN400 - NN455T0/0 - T4/4 , T5NN500 - NN555T0/0 - T4/4 , T5NN497Z - NN499Z 10/12, 14/16,18/20NX041 - NX045P1 - P5NX060K - NX087K10mm, 12mm,14mm: 52mm,92mm, 132mm10mm, 12mm,14mm: 52mm,92mm, 132mmNX060Z - NX087ZCobalt chrome alloy (CoCrMo) withmultilayer coating system made fromchromium nitride-chromium carbonnitride-zirconium nitride (CrN-CrCN-ZrN)Cobalt chrome alloy (CoCrMo)NN261K - NN264K 12mm, 14mm:T0 - T3 , T4 - T5
ComponentColumbus AS ObturatorMaterialCobalt chrome alloy (CoCrMo) withmultilayer coating system made fromchromium nitride-chromium carbonnitride-zirconium nitride(CrN-CrCN-ZrN)Columbus CRA/PSA Tibia Hemi Cobalt chrome alloy (CoCrMo)Spacers with screwColumbus AS CRA/PSA TibiaCobalt chrome alloy (CoCrMo) withHemi Spacers with screwsmultilayer coating system made fromchromium nitride-chromium carbonnitride-zirconium nitride(CrN-CrCN-ZrN)Product CodeSizeNN261Z - NN264Z 12mm, 14mm: T0- T3 , T4 - T5NN560K - NN596K T0 - T5NN563Z - NN596Z T0 - T5Please NoteImplants partly include metal components, so that metaldetectors could respond.Therefore, please carry yoour patient card with you,especially during Air travel, in order to pass the securitychecks.If there are any complications, please contact your hospital.MRI WarningScanning a patient who has this implant may result inpatient injury.Incident ReportingAny serious incident occuring in relation to the deviceshould be reported to B. Braun Australia Pty Ltd and to theTherapeutic Goods Administration.The implant has not been evaluated for safety andcompatibility in the MRI environment.Phone: 1800 206 045It has not been tested for heating, migration or imageartifact in the MRI enviorment.www.tga.gov.auwww.bbraun.com.au
VII B. BRAUN AESCULAP AG - AN INTRODUCTION TO THEMANUFACTURERThe name Aesculap is synonymus with surgical expertise.With over 150 years of experience, Aesculap continuessetting standards in surgery up to the present day.Worldwide it connects the knowledge of its approximately12500 employees, of whom approximately 3,840 work atthe company‘s headquarters in Tuttlingen, and developsproducts and solutions for all core surgical processes.Whether it‘s surgical instruments, suture material,microneedles, implants or sterile containers - throughconsistent research and development Aesculap strives forinnovations that make medical devices advances possible.Aesculap joint implants are products with the qualitystandard: Made in Germany. In this matter, the namese.motion , Columbus and EnduRo system stand for kneeendoprosthesis systems that have been used in more than300,000 implants.As part of the B. Braun Group, which is still a family business,the Aesculap division combines tradition and modernitythrough its comprehensive wealth of experience gatheredfrom its more than 40 years in the joint endoprosthesisindustry.As the largest German manufacturer of orthopaedicimplants, Aesculap is committed to close cooperation withdoctors and hospitals and aims to continue developing highstandards of patient safety.Its production site in Tuttlingen, Germany is one of the mostmodern joint implant manufacturing sites in Europe, wherethe components for artificial hip and knee prosthesis, spinalimplants, and screws, plates and nails for bone fractures aremanufactured. The production line at the Tuttlingen site hasits own, state-of-the-art biomechanics laboratory wherethe implants are subjected to a wide range of stress tests well beyond the regulatory standards.Through Sharing Expertise, Aesculap gives its partnersa promise to share medical knowledge, experience andhealthcare information through dialogue, and to use thisinformation effectively and constantly expand upon it.Further information can be found on the B. Braun website:www.bbraun.com
NOTES
B. Braun Australia Pty Ltd Level 5, 7-9 Irvine Place, Bella Vista NSW 2153 Australia Tel.1800 251 705 info@bbraun.com www.bbraun.com.auB. Braun New Zealand PO Box 37353, Parnell, Auckland 1052, New Zealand Customer Care 0800 227 286 Fax (09) 373 5601 www.bbraun.co.nzBANZ AE E0445 10/21 2021 B. Braun Australia
AESCULAP PATIENT INFORMATION. YOUR NEW ARTIFICIAL TOTAL KNEE JOINT. Dear Patient, The knee joint receives the most stress compared to other . joints in the body. The natural structure of the knee joint . enables a wide range of motion patterns. The knee joint function can be imparied by overloading, disease, and injury which lead to surgical implantation of an artificial knee replacement .