Transcription
Because a Better NarrativeChanges EverythingSNarrativePROIncrease Revenue Decrease DenialsBecause a better narrative changes everything.EMS Healthcare SolutionsImprove QA/QIProcess Standardized Narrative FormatSave Critical Time and Money.NOW! Increase Revenue Decrease DenialsNarrativePRO Improveis changing the QA/QIway narrativesare written. It works as an “add-on”program toFormatany ePCR or paper reportProcess StandardizedNarrativeon the market. NarrativePRO containsendless optionsmost complete Narrativeand thorough narrative possible. The bestNarrativePROis NOT foran theauto-generatedIHDWXUH LV WKH ÀH[LELOLW\ RI LWV RSWLRQV QRQH RI ZKLFK DUH PDQGDWRU\ RX PD\ FKRRVH IURP DOO WKH RSWLRQV JLYHQ DGG WR them, or simply use your own words.NarrativePROis very anddetailedin every way, yet basic and simple to understand.SaveCritical han10minutesbutwithtwicethe detailandtoinformation!NarrativePRO is changing the way narratives are written. It works as an “add-on”programany ePCR or paper report onthe market. NarrativePRO contains endless options for th emost complete and thorough narrative possible. The best feature isthe flexibilityBillingof its options,none of which are mandatory. You may Improvechoose from all Patientthe options given,add to them, or simplyImproveReturnCareuse your own words. NarrativePRO is very detailed in every way, yet basic and simple to understand. Imagine writing a fullTheprogramincorporatesseveralto justify7KH ¿QDO QDUUDWLYH LV VHFWLRQHG E\ KHDGHUV LQ pageor morein less than 10minutesareasbut withtwice the detail and information!the need for not only transport by ambulance, butchronological order. This organized narrative greatlythe mobility status of the patient and the reason forimproves the QA/QI process, and critical data can behospitalto hospitaltransfer.These areas are criticalfoundeasily toPatientensure thatprotocol is being followed.ImproveBillingReturnImproveCareThe programincorporates several areas to justify theThe final narrative is sectioned by headers, into billingsuccess.need for not only transport by ambulance, but themobility status of the patient and hte reason forReducePreventLitigationhospital to /hospitaltransfer.EMSThese areasare criticaltobillingsuccess.NarrativePRO’s features ensure that crew memberschronological order. This organized narrativegreatly improves the QA/QI process, and criticalStandardizedNarrativedata can be found easilyto ensure thatFormatsprotocol isbeingfollowed.Whether the narrative is in CHART or SOAP format,input the right information decreasing potential riskfor litigation. There’s no doubt about the quality andReduce/Preventthoroughnessof the report. EMS litigationyou will have a consistent, legible, and easy to readnarrative; each time, every time.NarrativePRO’s features ensure that crew membersinput the right information decreasing potential riskfor litigation. There’s no doubt about the qualityChangingtheway you thinkand thoroughness ofthe report.about narrative writing.Standardized Narrative FormatsWhether the narrative is in CHART or SOAPformat, you will have a consistent, legible, andeasy to read narrative; each time, every time.Real Results, Real People.The addition of NarrativePRO has greatly improved theeffectiveness of our documentation. I would recommend itto anyone!Changing the way you think about narrative-Dollywriting.Giles, Former DirectorPike County Memorial Hospital EMS/ Louisiana, MOReal Results, Real People.“Weallowednew EMT,who SOHDVHG has neverZLWK writtena runreport use2XU ELOOLQJ aRI¿FH LV YHU\ WKH 1DUUDWLYH352 se whonarratives and we have seen a marked reduction in billinghave been in the field for many years.”rejections due to poor documentation.-Larry Chasteen,Administrator“As the QI and Billing person, NarrativePROhas definitelymadeNorth Scott County ambulance District/ Chaffee, MOmy job much easier. Better and more legible documentation andconsistent across all of our staff. We can process claims quickerwith fewer tickets to fix.”Ready to Get Started? Get yourReadyFREEto get 30-Daystarted, call888.943.5604.TrialToday.2055 Walton Road, St. Louis, MO 63114 www.narrativepro.com 888-943-5604888.943.5604 www.EMSHealthcareSolutions.com
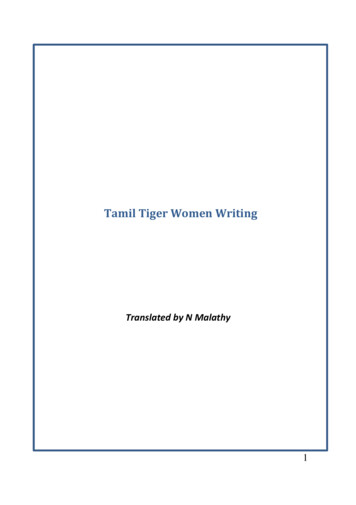
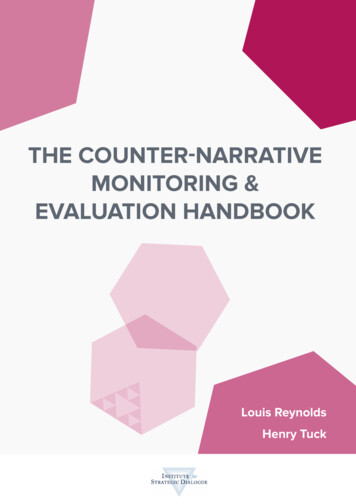
YOUR AMBULANCE COMPANY1255 Main StreetAnytown, Missouri 1234511/30/2017INSERT INSURANCE INFORMATION HERE[CHIEF COMPLAINT / RESPONSE] This crew responded to a call for a 51 year old male that was dispatched by central dispatch for respiratorydistress. Unit responded emergency, with lights and sirens. The chief complaint for the patient is RESPIRATORY DISTRESS. The secondary problemappears to be generalized weakness. Upon arrival to the scene we found the patient sitting on bed at residence. The general impression of the patientwas severe distress. Fire department personnel were on scene. FD assisted with placing patient onto ambulance cot. FD placed patient on oxygenvia a nasal cannula. Patient was assisted up, pivoted, placed onto wheeled stretcher. Patient was secured to stretcher using stretcher straps andstretcher was secured into ambulance. Patient was positioned on stretcher in high-fowlers position. Per the ambulance crew, the patient requiredoxygen, but couldn't self-administer and requires airway monitoring.[HISTORY OF PRESENT ILLNESS / INJURY] History was obtained from patient. This problem began 1 hour ago. This is an occasional problem forthe patient. The last time this occurred was 6 months ago. This problem has gotten worse since onset. Allergies: Penicillin. Changes: Nothing thepatient has done helps. Medical History: congestive heart failure, COPD, and diabetes. Medication List: Albuterol, Insulin, and Lasix. Meds - Prior toour arrival, the patient had used nebulizer treatment. Normal: Patient normally on oxygen continuously. The patient states he went to retrieve his mailand when the patient returned he was extremely short of breath. Patient requests transport to Emergency Department for evaluation.[ASSESSMENT – PRIMARY] Joshua L. Ball, CCEMT-P has performed a complete head to toe ALS assessment on the patient. Patient was consciousand alert.HEAD/NEURO: Clear speech, Neuro assessment intact, No facial droop, No JVD, No loss of consciousness, No memory loss, and Trachea midlineCHEST/RESPIRATORY: Breathing - Tachypneic, Cough - Productive, Dyspnea - COPD history, Equal chest rise and fall, Lung Sounds - Rhonchibilaterally, all lobes. , and Sputum - Frothy whiteABDOMEN: Bowel sounds present, Flat, No complaint of nausea, Non-tender, and SoftPELVIS/GU: No incontinence, and Pelvis stableEXTREMITIES: Capillary refill greater than 2 seconds, Equal grips, Good pulse, motor function, and sensation in all extremities, and No pain inextremitiesOTHER: Fever 100 Degrees, and Skin - Hot and dryMOBILITY: Ambulance staff observed that the patient cannot get out of bed without assistance, ambulate or sit in wheelchair safely and therefore thepatient is bed confined by the definition of Medicare. DIAGNOSTICS: Initial EKG rhythm was and remained sinus tachycardia with no ectopics, perparamedic. 12 Lead EKG shows no ST elevation or depression.V/S: Obtained at 12:00; LOC - Alert, Person, Place, Time, Event; Blood Pressure 150/90, manual, high fowlers; Pulse - 110, regular, radial; Respirations - 24 breathes per minute, labored; Sa02 - 88% with oxygen at 1-6 lpm;Temperature - 101.2, fahrenheit, taken tympanic; GCS - 15; CO2 - 55; Pain - 0; Blood Sugar - 205 mg/dL; Notes - Initial contact with the patient.Obtained at 12:20; LOC - Alert, Person, Place, Time, Event; Blood Pressure - 130/88, NIBP, high fowlers; Pulse - 102, regular, radial; Respirations - 18breathes per minute, labored; Sa02 - 98% with cpap therapy; GCS - 15; CO2 - 45; Pain - 0; Notes - Patient care released to the receiving RN.[RX / TREATMENT] [12:01] OXYGEN: Oxygen was initiated by Joshua L. Ball, CCEMT-P at 15 lpm via non-rebreather mask. The patient's conditionno change. Authorized by protocol (standing order).[12:02] MEDICATION: Joshua L. Ball, CCEMT-P administered Albuterol 2.5 mg nebulized. The patient's condition no change. Medication authorized byprotocol (standing order).[12:04] PROCEDURE: Joshua L. Ball, CCEMT-P initiated c-pap therapy. The patient's condition no change. Medication authorized by protocol(standing order).[12:05] IV: Joshua L. Ball, CCEMT-P initiated an IV 0.9% NaCl with an 18 g IV in the left ac at a rate of KVO with a total infusion of 100 cc's. Thepatient's condition no change. Authorized by protocol (standing order). No swelling at insertion site. No redness at insertion site. Insertion site cleanedusing an aseptic technique[12:06] MEDICATION: Joshua L. Ball, CCEMT-P administered Solu-Medrol 125 mg IVP. The patient's condition no change. Medication authorized byprotocol (standing order).[ASSESSMENT – SECONDARY] An ongoing assessment was performed by Attendant 1 every 5 minutes. Patient states they are breathing easier now.Patient states the oxygen is helping.HEAD/NEURO: No changes from prior assessmentCHEST/RESPIRATORY: No changes from prior assessmentABDOMEN: No changes from prior assessmentPELVIS/GU: No changes from prior assessmentEXTREMITIES: Capillary refill now less than 2 seconds and Nail beds back to normal colorOTHER: No changes from prior assessment[TRANSPORT] Patient was transported without incident and without delay. Patient was transported via ALS to emergency department. Patient movedfrom stretcher to emergency department cot via two person sheet lift. IV line still patent, no swelling or discoloration at insertion site. All of patient'sbelongings were turned over to the hospital staff and/or patient. Patient care and report given to emergency department nurse. The person taking overcare had no questions. The person taking over care was given a patient report that included the patient's medical history, medications, allergies, andinsurance information.DOCUMENTATION: Patient signed consent on computer form. Nurse signed for patient transfer of care on computer. Patient signed for HIPAApamphlet on computer form.Report By: Joshua L. Ball, CCEMT-PDriver: Jamie Miller EMT-PAttendant One: Joshua L. Ball, CCEMT-P
SEMS Healthcare SolutionsNarrativePRO by EHS now includes "DRAATT"The clinical narrative is the centerpiece of your patient care report (PCR).A good narrative provides a complete and accurate account of the events ofa call, and the actions taken during the call. A well-written clinical narrativeshould also convey details of an ambulance run in a clear, chronologicalmanner and capture all relevant information about the patient’s condition,treatment, and transport.Unlike the SOAP and CHART formats which were developed by physiciansto assist with clinical narratives in the hospital setting, DRAATT is anEMS-specific, chronological clinical narrative format.Because a better narrative changes everything.888.943.5604 www.EMSHealthcareSolutions.com
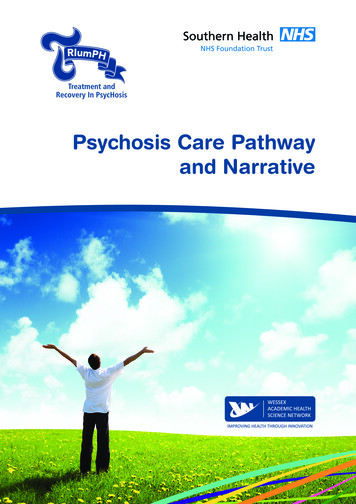
DRAATT stands for:Dispatch Response Arrival Assessment Treatment Transport.Specifically designed to capture all aspects of an EMS call,from dispatch to transfer of care.NarrativePRO byNow includesthe DRAATT formatDeveloped byDRAATT is an EMS- specific,chronological narrative formatthat is featured inNAAC represents theindustry’s “Gold Standard ofExcellence” in compliance,ethics and integrity in all facetsof ambulance compliance.
SEMS Healthcare SolutionsWE’VE GOT NEWS!An amazing combination. EHSand iPCR have teamed up.NarrativePRO by EHS andiPCR are integrated, allowingyou to complete your ePCRNEMSIS data and Narrativewith just one click of a button.Because a better narrative changes everything.888.943.5604 www.EMSHealthcareSolutions.com
A COMBINATION YOUHAVE BEEN WAITING FORNarrativePRO byDocumentation will never be the same again!Compliant narrative formats in CHART, SOAP or DRAATT!Complete your patient care report along with the narrative at the same time!
The clinical narrative is the centerpiece of your patient care report (PCR). A good narrative provides a complete and accurate account of the events of a call, and the actions taken during the call. A well-written clinical narrative should also convey details of an ambulance run in a clear, chronological