Transcription
ABSITE REVIEW2020Upper GI, Lower GI, and HerniaSuzie Hill, MD PGY-4@suziehillmd@SSATnews
UPPER GI GERD Peptic Ulcer Disease Esophageal dysmotility Gastric Cancer Esophageal Cancer GIST@suziehillmd@SSATnews
GERD 4 tests for work-up Esophageal Manometry24h pH study (or impedance)EGDBarium swallow Medical management: diet modification, H2 blockers, PPIs Anti-reflux surgery: Assess for hiatal hernia Mobilization of esophagus (4cm intra-abd), Collis gastroplasty formore length if needed Reapproximation of diaphragmatic crura posterior to esophaguswith non-absorbable suture Creation of fundoplication (Nissen 360º, Dor anterior 180º,Toupet posterior 270º)www.SSAT.com@suziehillmd@SSATNews@SSATnews
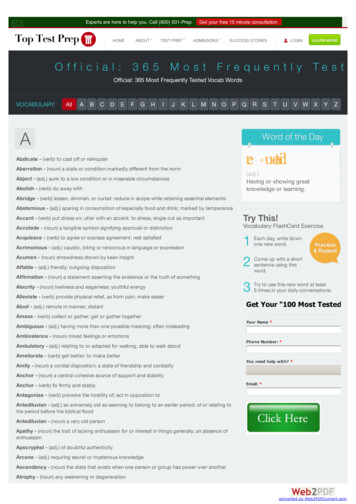
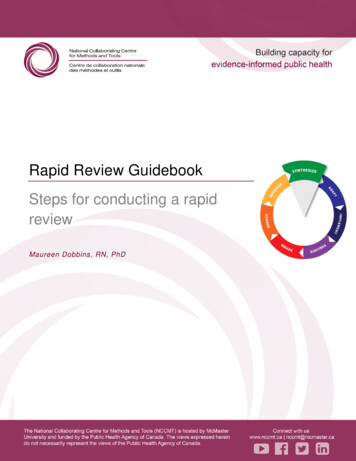
Esophageal DysmotilityDisorder (incidence)Presentation,pathophys, & w/uManometryTreatmentAchalasia(rare overall, MCesophageal dysmotilitydisorder) AperistalsisIncreased LES pressure Diffuse esophagealspasm Nutcracker esophagus Dysphagia,regurgitationFailure of LES torelaxBirdbeak contrastesophagramNon-cardiac chestpain, globus,dysphagiaCorkscrewappearance onbarium swallowPain MC sxBarium usuallynormal but can havecorkscrewappearanceImages from Current Surgical Therapy, 13Ed. ontractionsHigh amplitudecontractions( 180mmHg)or long swallow( 7s) Medical (Nitrates,CCB) usuallytemporary reliefPneumatic dilationof LESPOEMHeller myotomyCCB, nitratesminimally effectiveModified BelseyMark IV myotomybut not veryeffectiveCCBsBotoxLong thoracicmyotomy@suziehillmd@SSATnews
Esophageal Cancer SCC Adenocarcinoma Upper to mid esophagus RF: EtOH, tobacco Propensity for submucosalspread Cisplatin-based neoad tx Mid to lower esophagus 2/3rds of pts will p/wresectable dz Surgical Tx Tis/T1a (just mucosa):ablate T1b: surgery first T2 or N1 : neoad CXRT Stage: PET/CT, EGD bx, EUS R Gastroepiploic a. main bloodsupply to conduitTypeTranshiatalIvor-Lewis3 Hole/En BlocIncisionsNeck AbdChest AbdNeck, Chest, AbdAnastomosisNeckChestNeckLimitationsLimited LNdissectionPts get sicker if leak Highest leak andmorbidity rate@suziehillmd@SSATnews
Peptic Ulcer Disease Dx: EGD, H pylori testing,fasting gastrin level Tx: H pylori (3x therapy – PPI,flagyl, clarithromycin) PPIs (inhibit H/K ATPase inparietal cells and preventsHCl release) Gastric ulcer 3cm mayharbor cancer, need bx! Surgery (less common) Gastric wedge Graham patch / Thal patch Bleeding DU – 3 pt ligation(12, 3, 6 o’clock of GDA) V D ONLY in stable ptAcidhypersecretionImage creditCurrent Surgical Therapy 13 Ed@suziehillmd@SSATnews
Gastric Cancer Work-up EGD bx, EUS, PET/CT Siewart class if GEJ Dx lap? MAGIC trial: progressionfree and overall survivalbenefit to periop epirubicin 5FU cisplatin CLASSIC trial: curative R0resection D2 LNdissection adj CapeOximproved outcomes NCCN: R0 resection (w5cm margins), 15 LNsImage creditClinical Scenarios inSurgical Oncology
GIST Work-up EGD showing submucosalmass EUS ( /- FNA) CT AP TKI-therapy Neoad. imatinib ifdownsizing facilitatesnegative margins Assess response with CT(tumor changes fromheterogenous/hypervasc homogenous,hypoattenuating, andcystic) High risk for recurrence adjuvant imatinib MC sites of mets are liver peritoneum 3 major factors predictingmets are tumor origin,size, and mitotic rate R0 resection (often cando wedge) Low incidence of nodalmets so often astrointestinal@suziehillmd@SSATnews
LOWER GI Diverticulosis LGIB Volvulus IBD Colon Cancer Rectal Cancer Anal Cancer@suziehillmd@SSATnews
Diverticulosis False diverticula (only mucosa protrudes) Often asx 10-20% have diverticulitis 15% have bleeding Diverticulitis management principles: Broad-spectrum abx Surgery is individualized pt decision(1st attack usually the worst) Sig colectomy, take to upperrectum where taenia disappear Low colostomy reversal rates,try to use DLI if possible Everyone needs cscope 6w postattack to r/o ca Can result in fistula (colo-colonic, -enteric, vesical, -vaginal, -cutaneous)Image credit to Current Surgical Therapy13 Ed.@suziehillmd@SSATnews
Lower GI Bleed 60% diverticulosis (75% stopspontaneously but then 25%rebleed) Other causes: Angiodysplasias (MC R Colon, highrebleed rate of 80%)Ischemic colitis (up to 16% of LGIBcases, usu from reperfusion injury)Neoplasia ( 10%, cecal/R-sidedmore occult bleeding, L-sided/rectalmore obvious bleeding)Hemorrhoids (5-20%)UGIBIBD W/u r/o UGIB first Nuc 99Tm: 0.1-0.5 mL/min CTa: 0.3-1 mL/min Angio: 0.5-1.5 mL/min Colonoscopy Tx Angioembolization Colonoscopy maneuvers Indication for surgery: if 6upRBC requirement in 24h Resection (ideally segmentalcolectomy, poor outcomes wTAC)@suziehillmd@SSATnews
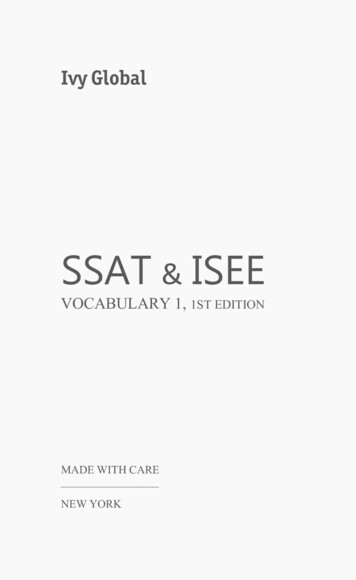
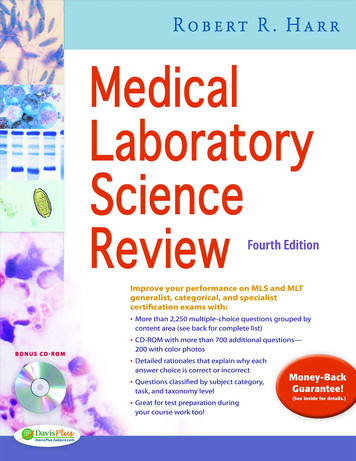
VolvulusImage credit to Radiopedia@suziehillmd@SSATnews
IBD-----------------@suziehillmd@SSATnews
Colon Cancer Work-up Bx of primary lesion Cscope to r/o synchronouslesions CT AP, CXR Serum CEA Resection principles Ligation at vessel take-off R colon (ileocolic) T colon (usu. extended right orleft, take middle colic) L colon (L colic at IMA origin) Sigmoid colon (sigmoid a) Need 12 nodes Polypectomy adequate if T1lesion, 2-3mm margin, noneuro/LVI Treatment principles Can perform isolatedmetastectomy Adjuvant FOLFOX for stageIII/IV (or stage II if 12 LNharvest) No indication for XRT K-ras wildtype: can useVEGF inhibitor (Avastin) orEGFR inhibitor (cetuximab) Surveillance w qy CEA cscope@suziehillmd@SSATnews
Familial Colon Ca SyndromesTPC-end ileos. or TPC-IPAA*@suziehillmd@SSATnews
Rectal Cancer Work-up Rigid procto for distancefrom anal verge Cscope to r/o synchronouslesions MRI pelvis to evaluate MRF,sphincter involvement, T/Nstatus CT CAP to evaluate Mstatus CEA Treatment Principles Stage II/III dz getsneoadjuvant CXRT (5FU 50.4Gy to pelvis) Lower 1/3rd (0-5cm ): APR Upper 2/3rd (5-15cm): LAR Transanal excision if T1 3cm 1/3rd circumferencemobile and non-fixed well-differentiatedno neuro/LVIno evidence of LNinvolvement If p/w obstruction, divertingloop colostomy first@suziehillmd@SSATnews
Anal Cancer Anal SCC Nigro protocol5FU mitomycin XRTRecurrent dz salvage APR,palliationMC mets to lung, liverRF for recurrence – size 5cm, 2/3rds circumference of analcanal involved Anal IntraepithelialNeoplasm (AIN) Precursor lesion for SCCHRA, local ablationCheck for HPV 16/18 Anal melanoma WLE Historically answer was APR Paget’s (adenoca.) Must cscope to r/o colonadenoca. APR 5FU Bowen’s (SCC insitu): WLE@suziehillmd@SSATnews
HerniasTypes of RepairComponent Separation@suziehillmd@SSATnews
Types of Hernias Ventral Hernias EpigastricUmbilicalLumbar, SpigealianParastomal Groin Hernias Inguinal Femoral (McVay) Obturator Incisional 11-20% of laparotomyincisions Ports 10mmImage credit to Nuem Blog@suziehillmd@SSATnews
Ventral Hernia RepairPrinciples Weight loss, smokingcessation x4w, glucosecontrol, improvednutrition 2cm: Primary repair 2cm: Mesh@suziehillmd@SSATnews
Component Separation Complete LOAElevate lipocutaneousflaps 2cm lateral to lineasemilunaris at edge ofrectus Incise EO fascia separate EO/IO Incise 1cm lateral to lineaalba to release posteriorrectus sheath anddevelop out to lineasemilunarisImage credit to Dimick,Clin Scenarios in Surgery, 2E@suziehillmd@SSATnews
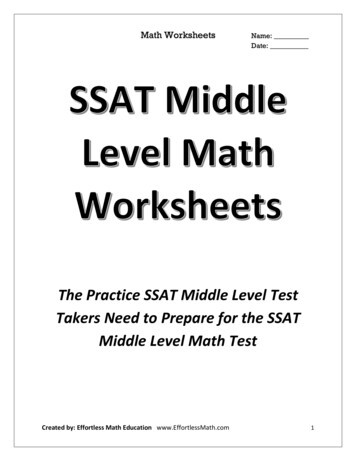
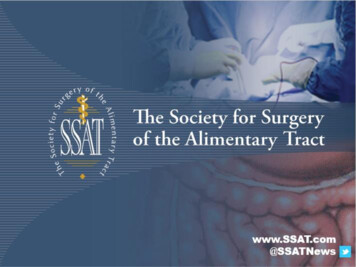
InguinalHerniasMC injuredduring openrepairMC injuredduring laprepairImage credit to SchwartzPrinciples of Surgery, 11Ed.@suziehillmd@SSATnews
Image Credits Cameron JL, Cameron AM. Current Surgical Therapy. 13th Ed. Philadelphia, PA. Elsevier. 2020. Khatri, V. Clinical Scenarios in Surgical Oncology. Philadelphia, PA. Lippincott Williams & Wilkins. 2005. Gold JS, Gonen M, et al. Development and Validation of a Prognostic Nomogram for recurrence-freesurvival after complete surgical resection of localised primary gastrointestinal stromal tumour: aretrospective analysis. Lancet Oncol . 2009 Nov;10(11):1045-52. Hacking C, Alwalid OAA. Sigmoid volvulus versus cecal volvulus. d-volvulus-versus-caecal-volvulus?lang us. Accessed Dec 29,2020. Steele SR, Hull TL, Read TE, et al. The ASCRS Textbook of Colon and Rectal Surgery. 3rd Ed. SpringerInternational Publishing. 2016. Trevino J, Farooqi S. Inguinal Hernia Imaging and Reduction. Published Aug 15, . Accessed Dec 29, 2020. Dimick JB, Upchurch GR, Sonnenday CJ, Kao LS. Clinical Scenarios in Surgery, Decision Making andOperative Techniques. 2nd Ed. Philadelphia, PA. Wolters Kluwer. 2019. Brunicardi FC, Anderson DK, Billiar TR et al. Schwartz’s Principles of Surgery. 11th Ed. McGraw Hill. 2019
ABSITE REVIEW 2020 Upper GI, Lower GI, and Hernia Suzie Hill, MD PGY-4 @suziehillmd @SSATnews. UPPER GI GERD Esophageal dysmotility Esophageal Cancer Peptic Ulcer Disease Gastric Cancer GIST @suziehillmd @SSATnews. www.SSAT.com @SSATNews GERD 4 tests for work-up Esophageal Manometry 24h pH study (or impedance) EGD Barium swallow Medical .