Transcription
Public Partnerships, LLC (PPL)Agency Payroll DepartmentOne Cabot rd. STE. 102Medford, MA 02155Phone (866) 315-3740Fax (866) 578-0533Support Broker’sDocumentsMA Autism Waiver ProgramForms & Instructions Check Run Schedule Timesheets Timesheet Instructions Invoice – Used for the purchase or goods and Items Visit and Daily Services Invoice Invoice Check list Invoice InstructionsEmployer of Record Employer of Record Instructions How to calculate rate?Provider Paperwork Employee vs Independent Contractor Provider Paperwork MatrixAll forms must be signed and returned to PPLprior to issuing paychecks.If you have any questions, please call PPL at (866) 315-3740.
One Cabot rd. STE 102Medford, MA 02155Phone (866) 315-3740Fax (866) 578-0533Electronic Timesheet and Invoice SubmissionNeed Help? Visit .aspx?maasd for acomplete user guideDDS has contracted with PPL to provide Financial Management Services to improve services toyou. Please do your part to correctly complete timesheets so that payment is not delayed.The Autism Waiver Program offers all providers the option to submit timesheets andinvoices online, directly into PPL’s Web Portal. The electronic timesheet and invoice optionhas many great features for users, including: Real‐time Budget validationAbility to access and submit timesheets and invoices 24/7Security for UsersMore environmentally friendly – less paper used!Electronic timesheets are paid on a bi‐weekly check run, and follow the same guidelinesof submission as paper timesheets and invoices. See the attached check run schedule.Timesheets are due by Monday at noon after the close of the pay period.The Autism Waiver Program offers two different methods for online timesheet and invoicesubmission: Option 1) The provider and participant can submit and approve timesheets directly inPPL’s Web Portal. The online tool will provide real time feedback if the timesheet can be processed or if PPL requires anyadditional information or authorizations from DDS Option 2) The Provider can submit online and receive the same real time feedback, thenprint out the completed timesheets and have the participant review and sign the papercopy. The system will already have the timesheet data stored and only need the signature of the participant toprocess a check.Need help? Call Customer Service Toll Free at 1-866-315-3740
Timesheet Instructions for Independent Contractors & AgenciesNeed Help? Call Customer Service Toll Free at 1-866-315-3740DDS has contracted with PPL to provide Fiscal Agent services to improve services toyou. Please do your part to correctly complete timesheets so that payment is notdelayed. Call PPL for help if you need it.Keep these important instructions. Timesheets are paid on a bi-weekly check run. Seethe attached check run schedule. Timesheets are due by Monday at noon after theclose of the pay period. Any timesheets received after the deadline will be processed inan off cycle check run the following Friday.Completed timesheets should be faxed toll free to 1-866-578-0536.Timesheets can also be mailed to the following address: Public Partnerships, LLC,One Cabot rd. STE. 102, Medford, MA 02155. Faxing timesheets may speed thepayment process for you. If possible, please fax your timesheets to PPL. For additionalcopies go tohttp://www.publicpartnerships.com.Important Do’s and Don’tsMUST DOMUST NOT DOUse black inkStay inside the linesWrite numbers and letters clearly. A machine willread your timesheet. Take the time to writeclearly, or ask someone else to write for you.Complete one timesheet per consumer. Use anew timesheet for each consumer you serve.Don’t use pencil or colored inkDon’t use military timeDo not round time. PPL will do this.Use a separate timesheet for each service type.Don’t use one timesheet for two consumers ormore than one service type.Try not to touch the edges of the box whenwriting numbers and letters.Don’t cross out information if you make amistake. Start a new timesheet.Consumers (or designated signatory) andAttendants must sign and date the timesheetFill in ALL required boxes, includingConsumer and Provider Name, ID andService Type.Use 2 lines when a provider starts and stops work2 times in the same dayUse A.M. and P.M. correctly. We show you howon the following page.Don’t use any other timesheet. PPL cannot payattendants if a different timesheet is submitted.Don’t write notes on the timesheet. This willcause our scanners to reject the timesheet andmay delay payment.Don’t forget to fill in all information such asAttendant and Consumer Name, ID, Service Type.Timesheets must be signed and dated by boththe consumer and the attendant.Need help? Call Customer Service Toll Free at 1-866-315-3740
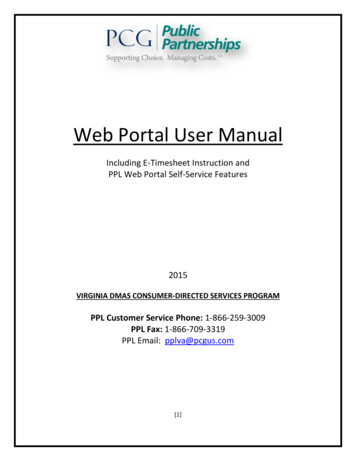
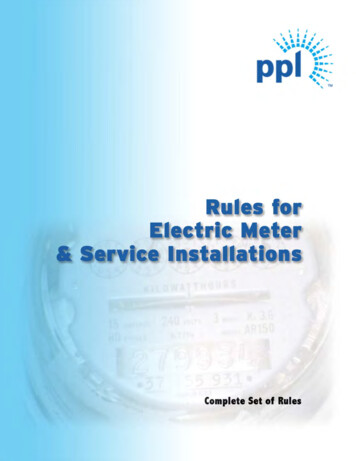
PUBLIC PARTNERSHIPS, LLC Provider TIMESHEET (Financial Management Services for MA DDS Autism Waiver Program)Service Type(fill one)PPL Provider ID:Homemaker-Habilitation - Community IntegrationConsumer's ID Number:14023WProvider's Name:Exp Hab - Education - Senior TherapistExp Hab - Education - TherapistConsumer's Name:Exp Hab - Education - Direct Support Worker FAX: PPL @ 1-866-578-0536}MAIL: PUBLIC PARTNERSHIPS LLC, One Cabot rd. STE. 102, Medford, MA 02155Week 1#CNSMRServedSunMonTueWedThuFri14023Sat/Begin: Sunday (mm/dd/yyyy)T i m e::::::::::::::INAM/PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMT i m e::::::::::::::By signing below, I certify thatI have provided the services tothe consumer during the timesdescribed on this time sheet.Provider Signature:OUTWeek 2/AM/PMTotal HoursAM PM::::::::::::::AM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM amily TrainingBehavioral Consultation - Senior TherapistBehavioral Consultation - Therapist/End: Saturday (mm/dd/yyyy)T i m e::::::::::::::INAM/PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMI certify that the consumerhas received hours of serviceas reported above.T i m eOUT::::::::::::::/AM/PMTotal HoursAM PM::::::::::::::AM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMAM PMDate://Consumer or Responsible Party Signature:USE B L A C K INK, PRINT O N E CHARACTER PER BOX, F I L L C I R C L E S COMPLETELY, DO NOT WRITE ON THE LINES !!!
Recording Header Information:1.Complete all header information for the Provider and the Consumer.Include name and ID of Provider and Consumer. The Provider ID is the ID provided toyour employee by PPL. The Consumer ID is will be provided by your support broker.Contact PPL Customer Service if you have any questions regarding these identificationnumbers.2.Use the correct pay period for your region (attached). Write the date inMM/DD/YYYY format.Make sure you write the start and end date for your pay period.3.Record the time of day correctly using A.M. and P.M.A.M. means morning. Morning starts at midnight, and ends at 11:59:59, or 11 o’clock, fiftynine minutes and 59 seconds, or one second before noon.P.M. Afternoon and evening (or night time) is captured by the initials P.M. Afternoon startsat noon, or 12:00, and ends at 11:59:59, or 11 o’clock, 59 minutes and 59 seconds, or onesecond before midnight. The date changes at midnight.4.Indicate the correct service typeConfirm only ONE service type has been bubbled in completely. Each service type has aspecific tax implication which is why it is important to fill each timesheet out based onservice type provided.5.Be sure to sign and date the timesheet.Need help? Call Customer Service Toll Free at 1-866-315-3740
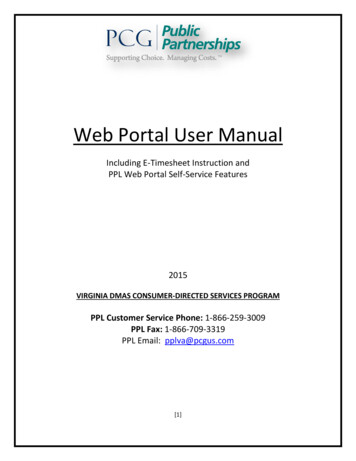
MA DDS Autism Waiver Program InvoiceVendor:Vendor ID#:Vendor Address:WTax IdentificationNumber:City, State, Zip:Consumer First Name:Consumer Last Name:Check here to send check to consumer's parent or legal guardian.Enter name/address here:Ship toShiptoAddress:Address:Consumer ID#:(*Complete this field ONLY if above box is checked / completed)Date of Acquisition/Service (mm/dd/yy)3Service Code 4Item Code 5Quantity ofitemspurchased 7Amount to be Paid 6//.//.Invoice Guidelines1. All attached invoices must be from the vendor identified at the top of this form and have a quote or price check receipt from the vendor as backup documentation accompanying this form.2. Enter one line per service code. If you purchased 2 of the same item, enter all on one line.3. Enter the mm/dd/yy that the quote or price check receipt was produced.4. Enter the service code that matches the service authorized in the consumer's budget.5540Other Services-Assistive Technology/Adaptive Aids5550Vehicle Adaptations5545Home Adaptations5555Individually Directed Goods and Services5. Enter the item code which identifies the type of item being purchased.Item CodeDescriptionItem CodeDescriptionItem CodeDescriptionItem CodeDescription01Adaptive Equipment04Computer Software07Home Saftey10Supplies & Materials02Communication Devices05GPS Unit08Membership & Fees11Vehicle Safety03Computer Hardware06Home Fence09Ramp12Other6. Enter the total amount (including taxes) that the check will be made out for. If you have more than one service code on the quote or price checkreceipt, distribute the taxes evenly among the service codes.7. Enter the number of items that will be purchased.Consumer's Representative must write the consumer ID number on the invoice. Sign the invoice and print thename of either the consumer or representative who signed. Write the date signed next to the signature.PLEASE KNOW THAT FAILURE TO FILL OUT THIS FORM COMPLETELY AND ACCURATELY CAN RESULT IN DELAY OF PAYMENT.Employer SignatureDateSupport Broker SignatureDateFAX OR MAIL INVOICE REQUEST WITH COPY OF QUOTE/PRICE CHECK RECEIPT TO:FAX To: 866-578-0533MAIL To: PPL, MA DDS Autism, One Cabot rd. STE. 102Medford, MA 02155Ver. 10/22/09Ver. 12.30.10
MA DDS Autism Waiver ProgramVisit and Daily Services InvoiceTherapy Form Guidelines:1. Enter one line per service code.2. Enter the begin and end date of the pay period.3. Enter the mm/dd/yy that the service occurred on.4. Enter the service code that matches the service authorized in the consumer’s budget.Consumer’s Representative must write the consumer ID number on the top of this form. Sign the form and print the name of either theconsumer or representative who signed. Write the date signed next to the signature.PLEASE NOTE THAT FAILURE TO FILL OUT THIS FORMCOMPLETELY AND ACCURATELY CAN RESULT IN DELAY OF PAYMENT.Therapist SignatureDateEmployer of Record SignatureDateFAX OR MAIL INVOICE REQUEST WITH COPY OF QUOTE/PRICE CHECK RECEIPT TO: FAX To: 866-578-0533MAIL To: PPL, MA DDS Autism, One Cabot rd. STE. 102, Medford, MA 02155Ver. 12.30.10
Instructions for the purchase of items, goods or adaptationsNeed Help? Call Customer Service Toll Free at 1-866-315-3740DDS has contracted with PPL to provide Fiscal Agent services to improve services to you.Please do your part to correctly complete invoice so that payment is not delayed. CallPPL for help if you need it.Keep these important instructions. Vendor Payments are paid on a bi-weekly check run.See the attached check run schedule. Vendor Payment Requests are due by Monday atnoon after the close of the pay period. Any Request received after the deadline will beprocessed in an off cycle check run the following Friday.Vendor Payment Requests can only be used if your budget allocates funds for:5540554555505555Assistive Technology/Adaptive AidsHome AdaptationsVehicle AdaptationsIndividually Directed Goods and ServicesYou must obtain a written estimate or quote (for example from Home Depot or acontractor) or a price check receipt (from most other stores including Best Buy and WalMart) from the store you will purchase the item from. This estimate or receipt needs toinclude the:Full company nameAddressPhone numberTax Identification NumberThe type of item being purchased and quantityThe total amount of the check for the work or cost of the items (including anysales taxes or shipping costs) that you are purchasingCompleted Request for Vendor Payment Forms should be provided to yourSupport Broker. Your Support Broker will fill out the service code and item code.http://www.publicpartnerships.com.Need help? Call Customer Service Toll Free at 1-866-315-3740
1. Complete all header information for the Vendor and the Consumer.Fill out all vendor and consumer information. Include if you want the check to besent to the consumer’s address, so you can bring the check to the vendor.2. Fill out the date on the purchase order in the Date of Acquisition/Serviceand total amount to be paidYour Support Broker will complete the service code and item code based on thepurchase order that you provide.3. Sign above the Employer Signature line and Date4. Provide the Estimate, Quote or Price Check Receipt and the Request forVendor Payment Form to your Support BrokerYour Support Broker will review, complete and sign the form and submit to PPL forpayment.Need help? Call Customer Service Toll Free at 1-866-315-3740
Public Partnerships, LLC(PPL) Agency PayrollDepartmentOne Cabot rd. STE. 102Medford, MA 02155Phone (866) 315-3740Fax (866) 578-0533CHECK LISTMA Autism Waiver ProgramSupport Brokers Check List forInvoicesINVOICES1) Confirm the family has provided you with the following: The quote or price check receipt from the vendorA completed Form W-9 from the vendor Commonly known national providers do not need tocomplete this form A filled out invoice cover sheet2) As the Support Broker, you have filled out/confirmed thefollowing: The Service Code as it relates to the budget that has beenapproved by the DDS Clinical ManagerThe item code based on the quote (above)Signed the bottom of the invoice cover sheet confirmingservice code / item codes are correct3) Fax the invoice and purchase order together to 1-866-578-0533.Any invoice or purchase order faxed separately will be rejected.All forms must be signed and returned to PPLprior to issuing paychecks to vendors.If you have any questions, please call PPL at (866) 315-3740.
Public Partnerships, LLC (PPL)Agency Payroll DepartmentOne Cabot rd. STE. 102Medford, MA 02155Phone (866) 315-3740Fax(866) 578-0533Employer of RecordPPL’s Payroll ServiceMA DDS AUTISM WAIVER PROGRAMWho Can Be the Employer ofRecord?ParentEmployer of RecordGuardianPerson Selected Needs to: Provide Social Security Number on FormsAssume all employer responsibilitiesComplete tax paperwork and submit to PPLIf guardian, provide PPL copy of guardian paperworkReceive mailings from tax and labor agenciesSign Employee TimesheetsDoes not already have an IRS Employer Identification Number (EIN) intheir nameManaging Payroll ResponsibilitiesFamily Member Does Serve as “The Employer” Define Job, Schedule and PayRate Recruit, Interview, Terminate Supervise and Prioritize Work Provide Necessary Training Complete Initial Paperwork Review, Sign & SubmitTimesheets Respond to Employee InquiriesPublic Partnerships Does Serve as “Payroll Department” Distribute Federal, State andLocal Tax Forms to Employersand Employees Issue Paychecks Per Timesheets Withhold All Necessary Taxes File Monthly, Quarterly andAnnual Tax and Labor Reports Issue Annual W-2 WageStatements Respond to All QuestionIf you have any questions, please call PPL at (866) 315-3740.
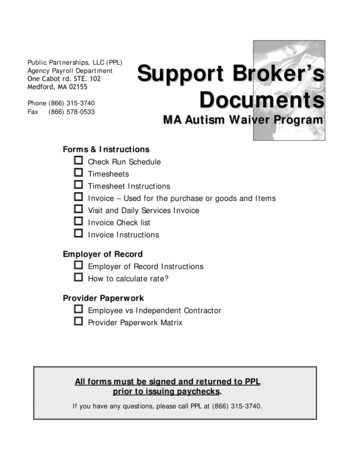
Public Partnerships, LLC (PPL)Agency Payroll DepartmentOne Cabot rd. STE. 102Medford, MA 02155PhoneFax(866) 315-3740(866) 578-0533Employee Rate CalculationPPL’s Payroll ServiceMA DDS AUTISM WAIVER PROGRAMHow to calculate Hourly Employees Rate?EMPLOYEE'S HOURLY RATE ON BUDGETHourly Employee Negotiated RateEmployer TaxesFICA (Social Security & Medicaid)State Unemployment Tax (est)Federal Unemployment TaxTax Rate7.65%2.89%0.80%Minimum Billing RateMedicaid Billing RateCheck divisible by 4 - Medicaid billing rateWorkers Compannual 11.13 13.92 16.70 19.48 22.27 10.00 12.50 15.00 17.50 20.00 0.77 0.29 0.08 0.96 0.36 0.10 1.15 0.43 0.12 1.34 0.51 0.14 1.53 0.58 0.16 11.13 11.13 2.78 13.92 13.92 3.48 16.70 16.70 4.18 19.48 19.48 4.87 22.27 22.27 5.57 563.00 563.00 563.00 563.00 563.00Hourly Employee's Taxes and Take Home PayEmployee Pay-Stub TaxesFederal Income Tax (est)State Income Tax (est)FICA (Social Security & Medicaid)Net Pay (est)Tax Rate15%5.85%7.65% 1.50 0.59 0.77 1.88 0.73 0.96 2.25 0.88 1.15 2.63 1.02 1.34 3.00 1.17 1.53 7.15 8.94 10.73 12.51 14.30Each employer has the opportunity to negotiate their employee’s hourly wagebased on the service being delivered and qualifications of the provider.The employee and the employer are both responsible for paying taxes. PPL willwithhold the required state and federal taxes from employees’ paychecks anddeposit based on state and federal requirements.The gross wages above are not the only wages that can be negotiated butprovides a matrix of the take home pay of the employee and the Medicaid BillingRate that will need to be entered into the consumer’s budget.If you have any questions, please call PPL at (866) 315-3740
Public Partnerships, LLCFiscal/Employer AgentOne Cabot rd. STE. 102Medford, MA 02155Toll Free NumbersPhone: 1-866-315-3740Administrative Fax: 1-866-578-0533EMPLOYEE OR INDEPENDENT CONTRACTOR?When a worker performs services and receives some form of payment, an important question is whetherthe payment is subject to employment taxes. The answer depends on whether the person is anemployee or independent contractor. Employees have taxes withheld every paycheck; independentcontractors do not have taxes withheld by PPL but are responsible for declaring their earnings at the endof the year.Below are the services available to individual providers in the MA DDS Autism Waiver Program. Based onthe service description the provider will be an employee or an independent memaker - IndividualXHabilitation - Community Integration - IndividualXExpanded Habilitation Services - Education-Senior Therapist-IndividualXExpanded Habilitation Services - Education-Therapist-IndividualExpanded Habilitation Services - Education-Direct Support WorkerXIndividualXRespite - IndividualXRespite – Caregiver’s HomeXFamily Training - IndividualXOccupational Therapy – IndividualXPhysical Therapy - IndividualXSpeech Therapy - IndividualXBehavioral Consultation – Senior Therapist - IndividualXBehavioral Consultation –Therapist - IndividualPaperwork to completeEmploymentVendorIn order to determine whether an individual is an employee or an independent contractor, the IRSstresses that evidence of the degree of control and independence must be considered. An IndependentContractor must exercise independent judgment, define assignments, setting priorities and schedules.The IRS states, “A general rule is that you, the payer, have the right to control or direct only the result ofthe work done by an independent contractor, and not the means and methods of accomplishing theresult.”The items below are helpful in determining if the worker is an employee or an independent contractor. If youselect even 1 box from the employee list than your provider is an employee.EMPLOYEE Is assigned tasks by employer Does not set priority of tasks Receives work schedule & breaks Does not determine workplace Does not provide own equipmentINDEPENDENT CONTRACTOR Professionally licensed or certified byoccupation Exercises independent judgment todetermine work tasks, work schedule,priorities & equipment needEach status requires a different tax form. Simply put, a W-4 Form is used if the worker is an employeeand Employment paperwork must be completed, and a W-9 Form is used if the worker is anindependent contractor and a Vendor Packet must be completed.Please call us at 866-315-3740 if you have any questions.
Provider ID CriteriaPublic Partnerships, LLC (PPL)Agency Payroll DepartmentOne Cabot rd. STE. 102Medford, MA 02155PPL’s Payroll ServiceMA DMR AUTISM WAIVER PROGRAMIdentifying the correct provider ID on your timesheets is crucial to PPL’s payrollsystem withholding taxes correctly.Please check all that apply and PPL will produce the necessary provider IDs foryou. As an individual provider you will have at least one provider ID and mighthave two.Individual ProviderIf you are an individual that will provide independent contractor services and will nothave taxes withheld by PPL, check: Individual, Independent Contract IDIf you are an individual that will provide employee services and will have taxeswithheld by PPL, check: Individual, Employee IDPPL will provide you with your provider ID(s) once PPL has processedall the necessary paperwork.
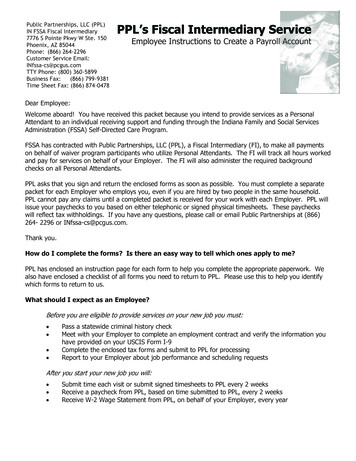
Public Partnerships, LLCMA DDS Autism Waiver Program Payment ScheduleFiscal Year 2014 (July 1, 2013 - June 30, 2014)One Cabot rd. STE. 102Medford, MA 02155Phone: (866) 315-3740NOTE: The schedule below reflects a bi-weekly check run. Checks are mailed and EFTs are sent to thebank on the Friday after the Finish date of the bi-weekly check run.TS Fax: (866) 578-0536Email: PPLMA Autism@pcgus.comFax: (866) 578-0533Invoices Received by PPL Will be mailed on:TimesheetsStart (Sunday)Finish (Saturday)June 30, 2013July 13, 2013July 15, 2013July 19, 2013July 14, 2013July 27, 2013July 29, 2013August 2, 2013July 28, 2013August 10, 2013August 12, 2013August 16, 2013August 11, 2013August 24, 2013August 26, 2013August 30, 2013August 25, 2013September 7, 2013September 9, 2013September 13, 2013September 8, 2013September 21, 2013September 23, 2013September 27, 2013September 22, 2013October 5, 2013October 7, 2013October 11, 2013October 6, 2013October 19, 2013October 21, 2013October 25, 2013October 20, 2013November 2, 2013November 4, 2013November 8, 2013November 3, 2013November 16, 2013November 18, 2013November 22, 2013November 17, 2013November 30, 2013December 2, 2013December 6, 2013December 1, 2013December 14, 2013December 16, 2013December 20, 2013December 15, 2013December 28, 2013December 30, 2013January 3, 2014December 29, 2013January 11, 2014January 13, 2014January 17, 2014January 12, 2014January 25, 2014January 27, 2014January 31, 2014January 26, 2014February 8, 2014February 10, 2014February 14, 2014February 9, 2014February 22, 2014February 24, 2014February 28, 2014February 23, 2014March 8, 2014March 10, 2014March 14, 2014March 9, 2014March 22, 2014March 24, 2014March 28, 2014March 23, 2014April 5, 2014April 7, 2014April 11, 2014April 6, 2014April 19, 2014April 21, 2014April 25, 2014April 20, 2014May 3, 2014May 5, 2014May 9, 2014May 4, 2014May 17, 2014May 19, 2014May 23, 2014May 18, 2014May 31, 2014June 2, 2014June 6, 2014June 1, 2014June 14, 2014June 16, 2014June 20, 2014June 15, 2014June 28, 2014June 30, 2014July 3, 2014June 29, 2014July 12, 2014July 14, 2014July 17, 2014Due by NoonCheck Run Date
Public Partnerships, LLCFiscal/Employer AgentOne Cabot rd. STE. 102Medford, MA 02155Toll Free NumbersPhone: 1-866-315-3740Administrative Fax: 1-866-578-0533SELECTING THE CORRECT PROVIDER IDWhen you are building a budget, it is very important that the correct provider ID is selected.You will use the employment or vendor agreement to ensure that you enter the rate that theprovider and family have agreed to pay, for each service that will be delivered. The family shouldprovide you with a copy of the agreement.The letter –E, -C, or –A at the end of each provider ID will indicate each provider for the correcttype of service. All Agency services must have a provider with a –A selected. Individuals providing Respite or Homemaker services must have a provider ID with an –E All other Individuals must have a –C provider ID selected.Please follow the matrix below when authorizing Providers in individual’s budgetsServiceHomemakerHabilitation - Community IntegrationExpanded Habilitation Services - Education-Senior TherapistExpanded Habilitation Services - Education-TherapistExpanded Habilitation Services - Education-Direct Support WorkerRespiteRespite – Caregiver’s HomeFamily TrainingOccupational TherapyPhysical TherapySpeech TherapyBehavioral Consultation – Senior TherapistBehavioral Consultation – PPL’s financial management system will validate if taxes are withheld from a paycheck based on theprovider ID and the type of service.For example, Sally Sample is providing Community Integration and Respite services. When youbuild the budget, you will select provider ID ‘wSAMP001-C’ for the Community Integrationauthorization and provider ID ‘wSAMP001-E’ for the Respite authorization.Please call us at 866-315-3740 if you have any questions.
Public Partnerships, LLCFiscal/Employer AgentOne Cabot rd. STE. 102Medford, MA 02155Toll Free NumbersPhone: 1-866-315-3740Administrative Fax: 1-866-578-0533Massachusetts Autism Waiver ProgramEMPLOYEE CHANGE OF NAME/ADDRESS FORMADDRESS/NAME CHANGE(Please Print)New Name:Former Name:Former AddressStreet:City:New AddressStreet:State:Zip:City:State:Zip:Employee SSN:Name of Consumer for whom you work:Consumer’s ID #:If you are completing this form because of a name change, please give this form and a copy ofyour new Social Security card to your employer. We will need a copy of this card, along withthis form, signed and completed, before the change will take effect.Employee SignatureDatePPL encourages you to call us toll free at 866-315-3740 if you have anyquestions.NOTE: Information provided on this form is confidential and is treated as such. Completion ofthis data is voluntary and will not affect your employment status. Identification can be declaredat any time prior to, or if applicable, after hire.
Public Partnerships, LLC (PPL) Agency Payroll Department One Cabot rd. STE. 102 Medford, MA 02155. Phone (866) 315-3740 . Fax (866) 578-0533 . . MAIL: PUBLIC PARTNERSHIPS LLC, One Cabot rd. STE. 102, Medford, MA 02155 USE B L A C K INK, PRINT O N E CHARACTER PER BOX, F I L L C I R C L E S COMPLETELY, DO NOT WRITE ON THE LIN ES !!! .