Transcription
BCA’s Favorite Behavioral Health Diagnosis CodesA Work-in-ProgressTable of Contents:ICD-10-CM Section IV Guidelines2-Page InsertICD-10-CM Chapter 5 Guidelines1-Page InsertPsychiatric & Related DiagnosisPages 1 - 3Substance AbusePages 4 - 6Social DeterminatesPage 3 Brown Consulting Associates, Inc. - www.codinghelp.com -Last updated October 29, 2018
ICD-10-CM Official Guidelines, Effective October 1, 2018 [Required/HIPAA Legislation]Section IV. Diagnostic Coding and Reporting Guidelines for Outpatient ServicesThese coding guidelines for outpatient diagnoses have been approved for use by hospitals/ providers in coding and reportinghospital-based outpatient services and provider-based office visits. Guidelines in Section I, Conventions, general coding guidelinesand chapter-specific guidelines, should also be applied for outpatient services and office visits.Information about the use of certain abbreviations, punctuation, symbols, and other conventions used in the ICD-10-CM Tabular List(code numbers and titles), can be found in Section IA of these guidelines, under “Conventions Used in the Tabular List.” Section I.B.contains general guidelines that apply to the entire classification. Section I.C. contains chapter-specific guidelines that correspond tothe chapters as they are arranged in the classification. Information about the correct sequence to use in finding a code is alsodescribed in Section I.The terms encounter and visit are often used interchangeably in describing outpatient service contacts and, therefore, appeartogether in these guidelines without distinguishing one from the other.Though the conventions and general guidelines apply to all settings, coding guidelines for outpatient and provider reporting ofdiagnoses will vary in a number of instances from those for inpatient diagnoses, recognizing that:The Uniform Hospital Discharge Data Set (UHDDS) definition of principal diagnosis does not apply to hospital-based outpatientservices and provider-based office visits.Coding guidelines for inconclusive diagnoses (probable, suspected, rule out, etc.) were developed for inpatient reporting and do notapply to outpatients.A. Selection of first-listed conditionIn the outpatient setting, the term first-listed diagnosis is used in lieu of principal diagnosis.In determining the first-listed diagnosis the coding conventions of ICD-10-CM, as well as the general and disease specific guidelinestake precedence over the outpatient guidelines.Diagnoses often are not established at the time of the initial encounter/visit. It may take two or more visits before the diagnosis isconfirmed.The most critical rule involves beginning the search for the correct code assignment through the Alphabetic Index. Never beginsearching initially in the Tabular List as this will lead to coding errors.1. Outpatient Surgery: When a patient presents for outpatient surgery (same day surgery), code the reason for the surgeryas the first-listed diagnosis (reason for the encounter), even if the surgery is not performed due to a contraindication.2. Observation Stay: When a patient is admitted for observation for a medical condition, assign a code for the medicalcondition as the first-listed diagnosis. When a patient presents for outpatient surgery and develops complicationsrequiring admission to observation, code the reason for the surgery as the first reported diagnosis (reason for theencounter), followed by codes for the complications as secondary diagnoses.B. Codes from A00.0 through T88.9, Z00-Z99The appropriate code(s) from A00.0 through T88.9, Z00-Z99 must be used to identify diagnoses, symptoms, conditions, problems,complaints, or other reason(s) for the encounter/visit.C. Accurate reporting of ICD-10-CM diagnosis codesFor accurate reporting of ICD-10-CM diagnosis codes, the documentation should describe the patient’s condition, using terminologywhich includes specific diagnoses as well as symptoms, problems, or reasons for the encounter. There are ICD-10-CM codes todescribe all of these.D. Codes that describe symptoms and signsCodes that describe symptoms and signs, as opposed to diagnoses, are acceptable for reporting purposes when a diagnosis has notbeen established (confirmed) by the provider. Chapter 18 of ICD-10-CM, Symptoms, Signs, and Abnormal Clinical and LaboratoryFindings Not Elsewhere Classified (codes R00-R99) contain many, but not all codes for symptoms.E. Encounters for circumstances other than a disease or injuryICD-10-CM provides codes to deal with encounters for circumstances other than a disease or injury. The Factors Influencing HealthStatus and Contact with Health Services codes (Z00-Z99) are provided to deal with occasions when circumstances other than adisease or injury are recorded as diagnosis or problems. See Section I.C.21. Factors influencing health status and contact with healthservices.F. Level of Detail in Coding1.ICD-10-CM codes with 3, 4, 5, 6 or 7 characters: ICD-10-CM is composed of codes with 3, 4, 5, 6 or 7 characters. Codeswith three characters are included in ICD-10-CM as the heading of a category of codes that may be further subdivided bythe use of fourth, fifth, sixth or seventh characters to provide greater specificity.2.Use of full number of characters required for a code: A three-character code is to be used only if it is not furthersubdivided. A code is invalid if it has not been coded to the full number of characters required for that code, including the7th character, if applicable.
G. ICD-10-CM code for the diagnosis, condition, problem, or other reason for encounter/visit: List first the ICD-10-CM code forthe diagnosis, condition, problem, or other reason for encounter/visit shown in the medical record to be chiefly responsible for theservices provided. List additional codes that describe any coexisting conditions. In some cases the first-listed diagnosis may be asymptom when a diagnosis has not been established (confirmed) by the physician.H. Uncertain diagnosis: Do not code diagnoses documented as “probable”, “suspected,” “questionable,” “rule out,” or “workingdiagnosis” or other similar terms indicating uncertainty. Rather, code the condition(s) to the highest degree of certainty for thatencounter/visit, such as symptoms, signs, abnormal test results, or other reason for the visit. Please note: This differs from thecoding practices used by short-term, acute care, long-term care and psychiatric hospitals.I. Chronic diseases: Chronic diseases treated on an ongoing basis may be coded and reported as many times as the patient receivestreatment and care for the condition(s)J. Code all documented conditions that coexistCode all documented conditions that coexist at the time of the encounter/visit, and require or affect patient care treatment ormanagement. Do not code conditions that were previously treated and no longer exist. However, history codes (categories Z80- Z87)may be used as secondary codes if the historical condition or family history has an impact on current care or influences treatment.K. Patients receiving diagnostic services onlyFor patients receiving diagnostic services only during an encounter/visit, sequence first the diagnosis, condition, problem, or otherreason for encounter/visit shown in the medical record to be chiefly responsible for the outpatient services provided during theencounter/visit. Codes for other diagnoses (e.g., chronic conditions) may be sequenced as additional diagnoses.For encounters for routine laboratory/radiology testing in the absence of any signs, symptoms, or associated diagnosis, assignZ01.89, Encounter for other specified special examinations. If routine testing is performed during the same encounter as a test toevaluate a sign, symptom, or diagnosis, it is appropriate to assign both the Z code and the code describing the reason for the nonroutine test.For outpatient encounters for diagnostic tests that have been interpreted by a physician, and the final report is available at the timeof coding, code any confirmed or definitive diagnosis(es) documented in the interpretation. Do not code related signs and symptomsas additional diagnoses.Please note: This differs from the coding practice in the hospital inpatient setting regarding abnormal findings on test results.L. Patients receiving therapeutic services onlyFor patients receiving therapeutic services only during an encounter/visit, sequence first the diagnosis, condition, problem, or otherreason for encounter/visit shown in the medical record to be chiefly responsible for the outpatient services provided during theencounter/visit. Codes for other diagnoses (e.g., chronic conditions) may be sequenced as additional diagnoses.The only exception to this rule is that when the primary reason for the admission/encounter is chemotherapy or radiation therapy,the appropriate Z code for the service is listed first, the diagnosis or problem for which the service is being performed listed second.M. Patients receiving preoperative evaluations onlyFor patients receiving preoperative evaluations only, sequence first a code from subcategory Z01.81, Encounter for pre-proceduralexaminations, to describe the pre-op consultations. Assign a code for the condition to describe the reason for the surgery as anadditional diagnosis. Code also any findings related to the pre-op evaluation.N. Ambulatory surgeryFor ambulatory surgery, code the diagnosis for which the surgery was performed. If the postoperative diagnosis is known to bedifferent from the preoperative diagnosis at the time the diagnosis is confirmed, select the postoperative diagnosis for coding, sinceit is the most definitive.O. Routine outpatient prenatal visitsSee Section I.C.15. Routine outpatient prenatal visits.P. Encounters for general medical examinations with abnormal findingsThe subcategories for encounters for general medical examinations, Z00.0- and encounter for routine child health examination,Z00.12-, provide codes for with and without abnormal findings. Should a general medical examination result in an abnormal finding,the code for general medical examination with abnormal finding should be assigned as the first-listed diagnosis. An examination withabnormal findings refers to a condition/diagnosis that is newly identified or a change in severity of a chronic condition (such asuncontrolled hypertension, or an acute exacerbation of chronic obstructive pulmonary disease) during a routine physicalexamination. A secondary code for the abnormal finding should also be coded.Q. Encounters for routine health screeningsSee Section I.C.21. Factors influencing health status and contact with health services, ScreeningSee also Disease Specific Guidelines (e.g., diabetes, HTN etc. in Section A in your ICD-10 book or on CDC website.End of HIPPA ICD-10-CM Section IV Guidelines
ICD-10-CM Official Guidelines, Effective October 1, 2018 [Required/HIPAA Legislation]See section I.C.19.e for coding of adverse effects and poisoning, and section I.C.20 for external cause code reporting.5. Chapter 5: Mental, Behavioral and Neurodevelopmental disorders (F01 – F99)a. Pain disorders related to psychological factorsAssign code F45.41, for pain that is exclusively related to psychological disorders. As indicated by the Excludes 1 noteunder category G89, a code from category G89 should not be assigned with code F45.41.Code F45.42, Pain disorders with related psychological factors, should be used with a code from category G89, Pain, notelsewhere classified, if there is documentation of a psychological component for a patient with acute or chronic pain.See Section I.C.6. Painb. Mental and behavioral disorders due to psychoactive substance use1) In RemissionSelection of codes for “in remission” for categories F10-F19, Mental and behavioral disorders due to psychoactive substance use(categories F10-F19 with -.11, -.21) requires the provider’s clinical judgment. The appropriate codes for “in remission” are assignedonly on the basis of provider documentation (as defined in the Official Guidelines for Coding and Reporting), unless otherwiseinstructed by the classification.Mild substance use disorders in early or sustained remission are classified to the appropriate codes for substance abuse in remission,and moderate or severe substance use disorders in early or sustained remission are classified to the appropriate codes for substancedependence in remission.2) Psychoactive Substance Use, Abuse and DependenceWhen the provider documentation refers to use, abuse and dependence of the same substance (e.g. alcohol, opioid, cannabis, etc.),only one code should be assigned to identify the pattern of use based on the following hierarchy: If both use and abuse are documented, assign only the code for abuse If both abuse and dependence are documented, assign only the code for dependence If use, abuse and dependence are all documented, assign only the code for dependence If both use and dependence are documented, assign only the code for dependence.3) Psychoactive Substance Use, UnspecifiedAs with all other unspecified diagnoses, the codes for unspecified psychoactive substance use (F10.9-, F11.9-, F12.9-, F13.9-, F14.9-,F15.9-, F16.9-, F18.9-, F19.9-) should only be assigned based on provider documentation and when they meet the definition of areportable diagnosis (see Section III, Reporting Additional Diagnoses). These codes are to be used only when the psychoactivesubstance use is associated with a physical, mental or behavioral disorder, and such a relationship is documented by the provider.c. Factitious DisorderFactitious disorder imposed on self or Munchausen’s syndrome is a disorder in which a person falsely reports or causes his or herown physical or psychological signs or symptoms. For patients with documented factitious disorder on self or Munchausen’ssyndrome, assign the appropriate code from subcategory F68.1-, Factitious disorder imposed on self.Munchausen’s syndrome by proxy (MSBP) is a disorder in which a caregiver (perpetrator) falsely reports or causes an illness orinjury in another person (victim) under his or her care, such as a child, an elderly adult, or a person who has a disability. Thecondition is also referred to as “factitious disorder imposed on another” or “factitious disorder by proxy.” The perpetrator, notthe victim, receives this diagnosis. Assign code F68.A, Factitious disorder imposed on another, to the perpetrator’s record. For thevictim of a patient suffering from MSBP, assign the appropriate code from categories T74, Adult and child abuse, neglect andother maltreatment, confirmed, or T76, Adult and child abuse, neglect and other maltreatment, suspected.See Section I.C.19.f. Adult and child abuse, neglect and other maltreatmentEnd of HIPPA ICD-10-CM Chapter 5 Guidelines
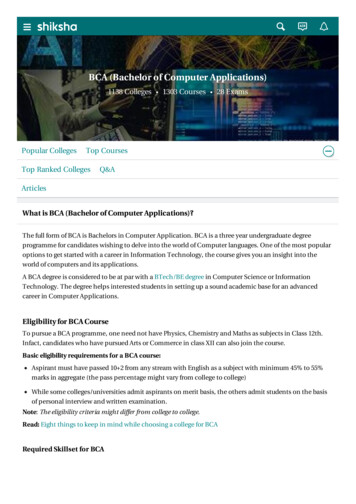
PSYCHIATRIC DX CODE SHEETADHD - Features are predominately (choose)ADHD; inattentive typeADHD; hyperactive typeADHD; combined (inattentive and hyperactive types)ADHD; other type, which is not considered as above three typesAnxiety and Related Dxs F40 F41 F43 and F93?Anxiety; generalizedAnxiety, mixed (with prominent features of other disorder )Panic disorder; w/o agoraphobia (panic attack) DEF in notewith agoraphobiaSeparation anxiety (of childhood )Other specified anxiety disorder (doc in record, but no code)Social phobia (anxiety) disorder, generalizedAcute stress reactionPost-traumatic Stress DisorderPTSD; acutePTSD; chronicavoidAnxiety; unspecifiedAdjustment Disorders F43.2Adjustment disorder; with depressed mood (grief reaction)with anxietywith mixed mood (anxiety & depression)with disturbance of conductwith mixed disturbance (emotion/conduct)with other symptoms not noted in available codesavoidAdjustment disorder unspecifiedBipolar Disorders F31CodeF90.0F90.1F90.2F90.8Major Depressive Disorders (MDD)MDD, single episode code choicesCode"Single episode" is the first-ever episode. DSM-5, pg 162: Dx code for MDD based onsingle vs recurrent and severity.MDD, single episode; (The patient's 1st Dx of MDD - may last months/years)HCC 58F32.0MDD, single episode; mild severityHCC58F41.1 MDD, single episode, moderate severityF32.1HCC 58F41.3 MDD, single; severe, WITHOUT psychotic symptomsF32.2HCC 58F41.0 MDD, single; severe, WITH psychotic symptomsF32.3HCC 58F40.01 MDD, single episode; in PARTIAL remissionF32.4HCC 58F93.0 MDD, single episode; in FULL remissionF32.5F41.8 MDD, single episode; severity cannot be specifiedavoid NoF32.9MDD, recurrent episode code choices (more common than single episode)F40.11F43.0 An "episode" likely to last many mos/years. DSM-5, pg 162: "recurrent" interval of 2consecutive months between separate episodes in which criteria for MDD are not met.HCC 58F43.11 MDD, recurrent episode; mildHCC 58F43.12 MDD, recurrent episode; & moderate severityHCC 58F41.9 MDD, recurrent; severe, WITHOUT psychotic symptomsHCC 58MDD, recurrent; severe, WITH psychotic symptomsHCC 58F43.21 MDD, recurrent episode in PARTIAL remissionHCC 58F43.22 MDD, recurrent episode in FULL remissionHCC 58F43.23 MDD, other reccurrent depressive disorder (specified)F43.24 MDD, recurrent episode, unspecifiedavoid HCC 58F43.25Other Depressive Episodes (Added 2016)F43.29 Premenstrual dysphoric disorderNoF43.20 Other specified depressive episode (specified in record)NoObsessive-compulsive disorder (OCD) F42Consider: manic, depressed or mixed, & mild, moderate or severe. Mixed obsession thoughts and actsIf "severe" select code based on presence/absence of psychosis. Hoarding disorderHCC 58F31.11 Excoriation (skin-picking) disorderBipolar, current episode is manic & mildHCC 58F31.12 Other obsessive-compulsive dis. (documented, but not listed above)Bipolar; current episode is; manic & moderateHCC 58F31.13 Obsessive-compulsive disorder, unspecifiedmanic & severe WITHOUT psychotic sordersF34manic & severe and WITH psychotic featuresHCC58F31.31 Cyclothymic disorderBipolar, current episode depressed & mildHCC 58F31.32 Dysthymic disorder DSM5 persistent depressive disordercurrent episode depressed & moderateHCC 58HCC 58F31.4 Disruptive mood dysregulation disorderdepressed but WITHOUT psychotic featuresHCC 58HCC 58F31.5 Other specified persistent mood disorderdepressed and WITH psychotic featuresHCC 58HCC 58F31.61 Mood disorder, unspec. (Active psychosis NOS)avoidBipolar, current episode mixed (manic & dep.) mildHCC 58F31.62Personality Disorders F60Bipolar; current episode mixed & moderateHCC 58F31.63 Antisocialmixed & severe, WITHOUT psychotic featuresHCC 58F31.64 Avoidantmixed & severe, and WITH psychotic featuresHCC 58F31.0 BorderlineBipolar, current episode hypomanicDependentBipolar Disorders IN REMISSION (Partial or Full Remission)Bipolar PARTIAL remissionHistrionicBipolar FULL remissionHCC 58HCC 58F31.71F31.72 NarcissistichypomanichypomanicHCC 58HCC 58F31.73F31.74 Obsessive-compulsivemanicmanicHCC 58HCC 58F31.75F31.76 ParanoiddepresseddepressedHCC 58HCC 58F31.77F31.78 SchizoidmixedmixedHCC 58avoidF31.9Schizophrenia/SchizoaffectiveBipolar disorder, unspecifiedHCC 58HCC 57F31.81 ParanoidBipolar II disorderHCC 57Manic Episode F30DisorganizedHCC58HCC 57F30.11 CatatonicManic episode w/o psychotic symptoms mildHCC58HCC 57F30.12 UndifferentiatedManic episode w/o psychotic symptoms moderateHCC 58HCC 57F30.13 ResidualManic episode w/o psychotic symptoms severeHCC 58HCC 57F30.2 Schizophreniform disorderManic episode with psychotic symptoms severeHCC 58HCC 57F30.8 Schizophrenia (a documented but no code exists)Other manic episodes (like hypomania)HCC 58HCC 57F30.3 Schizoaffective disorder, bipolar typeManic episode in PARTIAL remissionHCC 58HCC 57F30.4Manic episode in FULL remissiondepressive typeHCC 57avoid HCC 58 F30.9Manic episode, unspecifiedother specified (documented type, not bipolar or depressive)avoid HCC 57Schizoaffective disorder, unspecifiedScreening for Mental Health and Behavioral DisordersFactitious DisordersZ13.30 Δ Factitious disorder imposed on self; unspecified Screening; mental health & behavioral disorders, unspecZ13.31 depressionΔ with predominantly psychological sgns and symptomsZ13.32 maternal depressionΔ with predominantly physical sgns and symptomsZ13.39 other mental health and behavioral disordersΔ with combined psychological physical sgns and symptomsZ13.41 Factitious disorder imposed on another autismBrown Consulting Associates, Inc. ICD-10-CM Common Codes - WIP - October 29, 1F25.8F25.9F68.10F68.11F68.12F68.13F68.A1
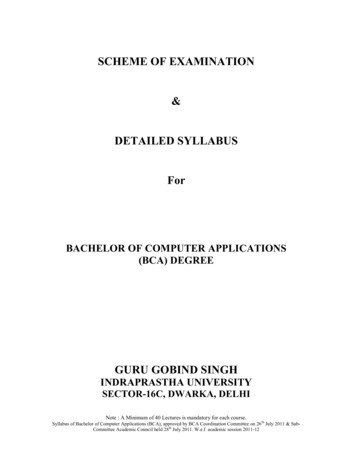
PSYCHIATRIC DX CODE SHEETCHILD MALTREATMENTReplace dash with A -initial, D -FU or S -sequelaADULT MALTREATMENTCodeT74.12X T74.32X T74.22X T74.02X T74.4XX T74.52XT76.52XT74.62XT76.62X-Child physical abuse, confirmedΔ Psychological abuse, confirmedSexual abuse, confirmedChild neglectShaken infant syndrome Sexual exploitation, confirmed Sexual exploitation, suspected Labor exploitation, confirmed Labor exploitation, suspectedOther Child DxsAutistic disorderHeller's syndromeChild psychosis NOSSchizophrenia, childhood typeChild Conduct DisordersOppositional defiant disorderAdolescent onset typeChildhood onset typeOther conduct disordersUnspecifiedDisorder - Social Functioning Child/AdolescenceSelective mutismReactive attachment disorderDisinhibited attachment disorderOther childhood disorderChild - Additional Social Status DxsParent child problems, unspecified.Parent-biological child problemCounseling-parent-adopted child problemCounseling-parent-foster child problemOther parent-child problemsOther specific problem related to upbringingAlcoholism in familySubstance abuse in familyOther psychosocial circumstancesSocial maladjustmentLegal circumstancesRefusal of tx for religious reasonsRelational problem, NOSBereavement, uncomplicatedCounseling perpetrator of physical/sexual abuseReligious or spiritual problemLife circumstance problemPersonal History of Mental Disorders (Any age)Affective disordersNeurosisHCC 55AlcoholismCombat and operational stressOther mental disordersavoidUnspecified mental disorderFamily hx of psychiatric conditionOther/Miscellaneous Dxs (Any Age)InsomniaHypersomnia Several codes available Check F51.0 - F51.9Self mutilation (personal hx)NoncomplianceAnorexia nervosaBulimia nervosaIntellectual Disabilities; 19F50.00F50.2F70F71F72F73Replace dash with A -initial, D -FU or S -sequelaAdult physical abuse, confirmedΔ Psychological abuse, confirmedsexualother abuse and neglectAdult neglect (nutritional) Sexual exploitation, confirmed Sexual exploitation, suspected Labor exploitation, confirmed Labor exploitation, suspectedAdult Related Info Dx CodesPerpetrator of spousal/partner abuseParent child problems, unspecified.Perpetrator of parental child abuseParent-biological child problemCounseling: parent-adopted child problemCounseling: parent-foster child problemParental overprotectionProblems with aged parents or in-lawsAlcoholism in familySubstance abuse in familyPersonal current military deploymentPersonal Hx return from military deployOccupational concerns, loss of jobChange of jobThreat of loss of jobStressful work scheduleDiscord with boss and workmatesDifficult conditions at workOther physical and mental strainSocial maladjustmentLegal circumstancesRefusal of tx for religious reasonsBereavement (disappearance/death)Religious or spiritual problemLife circumstance problemPerson awaiting admission to facilityExploitation Dx Codes (Any age) Exam and observation; following forced sexual exploitation following forced labor exploitation Forced labor or sexual exploitation in childhood Forced labor or sexual exploitationEmotional State Dx Codes (Any age)NervousnessIrritability & AngerImpulsivenessEmotional LiabilityDemoralization/ApathyOther emotional stateCognitive Defects (Any age)Attention/concentrationCognitive communicationVisuospatialPsychomotorFrontal lobe/executive functionOther cognitive deficitsDementia in disease classified elsewhereCode first, underlying conditionwith behavioral disturbances(OB) Puerperium Mental & Behavioral Disorders Postpartum depression Peurperal psychosisBrown Consulting Associates, Inc. ICD-10-CM Common Codes - WIP - October 29, 2018CodeT74.11X T74.31X T74.21X T74.01X T74.01X .843R41.844R41.89F02.80code firstF02.81F53.0F53.12
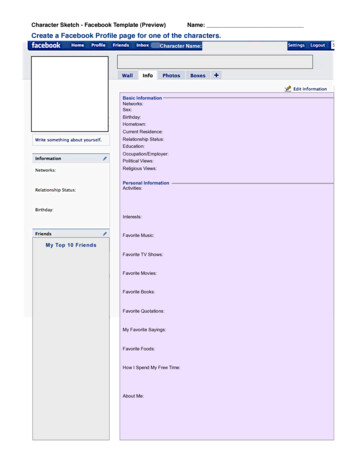
PSYCHIATRIC DX CODE SHEETCodeSigns and Symptoms (Any age)R41.3Memory lossR45.83Excessive cryingR41.82Altered mental statusR68.89Other general symptomsR27.9Lack of coordinationR63.5Abnormal weight gainR63.4Abnormal weight lossR47.89Other speech disturbanceR41.81Senility w/o mention psychosisR51HeadacheG47.9Sleep ssR68.82Decreased libidoR53.83FatigueR52Generalized painF51.4Night terrors (child)Nicotine Dependence vs Tobacco Use and ExposureF17.210Cigarette, uncomplicated (no related illness)in remissionF17.211in withdrawalF17.213F17.290Vapor or "Other" uncomplicatedin remissionF17.291in withdrawalF17.293CodeDx - Medication Management Code also clinical condition(s)Code:Therapeutic drug level monitoringZ51.81Z79.899Code Long term (current) drug therapyZ79.891Code Long term (current) use of opiate analgesicSee codeCode also the medical/psych diagnosis(es)Underdosing of Prescribed Medication by Patient (requires 2 codes)Refer these cases to coder for code assignmentCode first, underdosing of medication (T36-T50) with fifth or sixth character of "6", thencode intent and reason (below)1. Look up med or med class in ICD"A" Initial eval of this med management, "D" FU or "S" SequalaPatient Medication Noncompliance by Self Underdosing of;Replace dash (-) w/ A initial (active tx); D FU (healing); or S sequelatetracyclic antidepressantstricyclic antidepressantsother antidepressantantipsychotics (phenothiazine)amphetaminesother psychostimulantantipsychotics and ne/thiothixene narcolepticsT43.026 T43.016 T43.296 T43.3x6 T43.626 T43.696 T43.596 T42.3x6 T42.4x6 T43.4x6 -cannabisT40.7x6 -MAOIsmethadonemethyphenidate (ADD)narcotics (synthetic)opiumother opioidpsychotropic (other)SSRIsICD-10 Guidelines prohibit assignment of a diagnosis when that Dx. is only being 2. Code also intent and reason from self underdosing"considered" at this time. One might consider assignment of R69 in cases where INTENTIONAL underdosing of med(s) by patient;a definitive diagnosis cannot yet be assigned. R69 May or may not representdue to financial hardshipreimbursement problems, Coder/biller should monitor.for any other reasonMental illness, NOSF99UNINTENTIONAL underdosing by patient;Illness, unspecifiedR69due to age-related debilityfor any other reasonOther Patient Noncompliance DiagnosesOther med. noncompliance (e.g., self overdosing)Noncompliance involving other than medicationNoncompliance with dietSocial DeterminatesZ55.0 Foster care (status)Illiteracy and low-level literacyUnderachievement in schoolZ55.3 Family disrupt; due to military deploymentEdu. maladjustment, discord w/teachers & classmatesEdu.Z55.4maladjustment,due to otherdiscordabsencew/teachersof family&memberclassmatesUnemployment, unspecifiedZ56.0due to divorce/legal separationChange of jobZ56.1due to return from military deploymentThreat of job lossZ56.2 Problem related to primary support group, unspecifiedDiscord with boss and workmatesZ56.4 Conviction civil/criminal proceedings w/o imprisonmentOther physical and mental strain related to workZ56.6 Imprisonment and other incarcerationZ59.0 Lack of physical exerciseHomelessnessZ59.1 Inappropriate diet and eating habitsInadequate housingZ59.3 Burn-outPerson living in residential institutionZ56.4 Type A behavoir patternLack of adequate food and safe drinking waterExtreme povertyZ59.5 Stress, not elsewhere classifiedInsufficient social insurance and welfare supportZ59.7 Inadequate social skills, not elsewhere classifiedOther housing/economic circumstanceZ59.8 Social role conflict, not elsewhere classifiedProblems related to living aloneZ60.2 Limitation of activites due to disabilityAcculturation difficultyZ60.3 No household member to render careSocial exclusion and rejectionZ60.4 Holiday relief careOther problems related to social environmentZ60.8 Personal history of adult physical and sexual abuseChewing tobacco, uncomplicatedin remissionin withdrawal2nd hand tobacco smoke exposureOccupational tobacco smoke exposureHistory of tobacco dependenceavoidTobacco use, [no dependence]"PROVISIONAL DX" / "RULE OUT DX" TODAY?TXX.XXX -When assigning the "T" code, the 7th character will own Consulting Associates, Inc. ICD-10-CM Common Codes - WIP - October 29, 2018T43.1x6 T40.3x6 T43.636 T40.4x6 T40.0x6 T40.2x6 T43.8x6 T43.226 4Z73.0Z73.1Z73.3Z73.4Z73.5Z73.6Z74.2Z75.5Z91.4103
CHRONIC PAIN AND SUBSTANCE ABUSE DX CODE SHEETChronic Pain & Medication ManagementCodeCoding chronic pain management: List 1st the chronic pain Dx, then the clinical reason Dx,followed by "Therapeutic monitoring" Dx, and finally High-risk medication Dx, if appropriate.See 1-4 below.1. Chronic Pain SyndromeChronic Pain, unspecifieddue to; traumaneoplasm related2. Common conditions causing chronic painArthropathyFibromyalgiaLumbagoHCC 40R
C. Accurate reporting of ICD-10-CM diagnosis codes For accurate reporting of ICD-10-CM diagnosis codes, the documentation should describe the patient's condition, using terminology which includes specific diagnoses as well as symptoms, problems, or reasons for the encounter. There are ICD-10-CM codes to describe all of these.