Transcription
10/29/18And you shall rise and show respect to the agedPatient Driven Payment SystemPDPMOverviewEffective Oct 1, 2019 (FY20)Nov 2018Judy Wilhide Brandt, RN, BA, CPC, QCP, RAC-MT, DNS-CT909-800-9124judy@judywilhide.comTwitter: @WilhideMDSFacebook: /WilhideConsultingJudyWilhide.com1Objectives: Review the six components of the Patient Driven Payment System Discuss role of diagnosis coding and in the PT, OT, SLP, NTA components of aPDPM payment category Explain the variable per diem adjustment schedule Review the PPS MDS schedule Examine additions to the Part A PPS Discharge and limitations on modes oftherapy Explain the Interim Payment Assessment and it’s role in adjusting payment Review the differences between the PT/OT function score and the Nursingfunction score Explain how a function score is calculated Review the ‘interrupted stay policy’ Discuss changes to the nursing component categories Explain how presumption of coverage will work21
10/29/18www.judywilhide.com/resources3Patient Driven Payment System (PDPM)Goals: Remove therapy minutes as a determinant ofpayment and create a new therapy payment model inwhich payment is linked to differences in clinicalcharacteristics Create a separate payment component for nontherapy ancillary (NTA) services, using residentcharacteristics to predict utilization of these services. Will begin Oct 1, 201942
10/29/18PT 50OT 50ST 50NTA 50NursingOverview 300Six components in daily rate, all taken fromPPS 5 day MDS. Each separate componentwill be assigned a daily rate based on thatcomponent’s case mix index (CMI), all addedtogether for that resident’s daily rate. 50NonCaseMix 50NTA non-therapy ancillaries5PTOTNTAFull component rate for days 1 – 20, then bothPT and OT each decrease 2% every 7 daysFull component rate for days 1-3, then 70% decrease for days 4 - 100STNursingNo variable per diem adjustment for ST, Nursing, Non-Case MixNonCaseMixNTA non-therapy ancillaries63
10/29/18PTADL score is “end-split.” Now called “Function score”OTNursingNTA PT and OT use a function score derived from 10 ADL activities assessed in Section GG of aPPS 5 day MDS Nursing uses a function score derived from 7 ADL activities assessed in Section GG of aPPS 5 day MDSSTNonCaseMixNTA non-therapy ancillaries7Section GG Function Score Data Elements:PT and OT componentsNursing componentEatingGG0130A1 EatingEatingGG0130A1 EatingOralHygieneGG0130B1 Oral HygieneToiletingHygieneGG0130C1 Toileting HygieneToiletingHygieneGG0130C1 Toileting HygieneGG0170B1 Sit to LyingAverageBedMobilityGG0170B1 Sit to ngGG0170C1 Lying to Sitting on Side ofBedGG0170D1 Sit to StandGG0170E1 Chair/Bed-to-ChairAverageTransferGG0170C1 Lying to Sitting on Side ofBedGG0170D1 Sit to StandGG0170E1 Chair/Bed-to-ChairGG0170F1 Toilet TransferGG0170F1 Toilet TransferGG0170J1 Walk 50 Feet with TwoTurnsGG0170K1 Walk 150 FeetStart of PPS Stay Section GG on PPS 5 day MDS84
10/29/18For PT and OT Component:Section GG ResponsesFunction ScoreIndependent or Set-up (05,06)Supervision or touching assistance (04)Partial/moderate assistance (03)Substantial/maximal assistance (02)Dependent, refused, N/A, or cannotwalk (01,07,09,10, 88 or “could notwalk 10 feet”(GG0170H any code for “notattempted” 07,07,11,88), missing value43210Function Score Range 0 - 249Six final elements for PT/OT Function ScoreEatingOral HygieneToileting HygieneBed MobilityCategory - ItemsG0130A1 EatingGG0130B1 Oral HygieneGG0130C1 Toileting HygieneGG0170B1 Sit to LyingBed MobilityGG0170C1 Lying/sitTransferTransferTransferGG0170D1 Sit to StandGG0170E1 Chair/Bed-to-ChairGG0170F1 Toilet TransferWalkingGG0170J1 Walk 50 ft w/2 TurnsWalkingGG0170K1 Walk 150 FeetAdmissionPerformance06 set-up06 set-upInterimScore4W/averages (round tonearest whole number)402 max assist03 mod assist4124103 mod assist03 mod assist03 mod assist02 max assist222101 dependent01 dependentFunctionScore:000NA1321.66Round to 2When averaging bed mobility, transfer and walking, round to nearest whole number.105
10/29/18Nursing Function score: 4 final elementsAdmissionInterimPerformance ScoreEatingGG0130A1 Eating06 set-up402 maxToileting Hygiene GG0130C1 Toileting Hygieneassist103 modBed MobilityGG0170B1 Sit to Lyingassist2Bed MobilityGG0170C1 Lying to Sitting 03 modon Side of Bedassist203 modTransferGG0170D1 Sit to Standassist203 modTransferGG0170E1 Chair/Bed-toChairassist202 maxTransferGG0170F1 Toilet Transferassist1FunctionScore:NACategory - ItemsW/averages(round tonearest wholenumber)4121.66Round to 29When averaging bed mobility and transfers, round to nearest whole number.11 Every resident is classified into every component, every time, based onPPS 5 day MDS. Even if no PT or OT or SLP received, each resident’s rate is determinedusing the CMI achieved for each separate component. Each major component is further subdivided into groups, each with aunique CMI. The computation for PT and for OT are identical, but the resident will geta separate CMI for PT and for OT, every time.126
10/29/18Background - Clinical Categories: Based on analysis of primary reason for SNF care ten clinical categories werecreated:1. Acute Infections2. Acute Neurologic3. Cancer4. Cardiovascular and Coagulation5. Major Joint Replacement or Spinal Surgery6. Medical Management7. Non-Surgical Orthopedic/Musculoskeletal8. Pulmonary9. Non-Orthopedic Surgery10. Orthopedic Surgery (Except Major Joint Replacement or Spinal Surgery) Used Medical Severity – Diagnostic Related Group (MS-DRG) from the priorinpatient stay to define the primary reason for SNF care and assign residentsto clinical categories13Maj Joint Repl/SpinalSurgeryNon-ortho surgery andAcute neurologicOther OrthopedicMedical Management 10 Categories collapsed into 4 for PT and OT,because cost of care is commensurate Acute Neurologic is split out and used as afactor to generate the ST component rate Non-surgical orthopedic/musculoskeletal Ortho Surg (not Maj Joint Repl/Spinal Surgery) Acute infections Medical Management Cancer Pulmonary Cardiovascular & Coagulation147
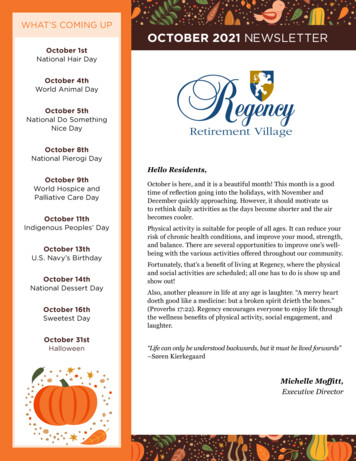
10/29/18Percentage of SNF stays in PDPMResearchMedical Management60%Acute neuro/nonortho surgOther ortho17%14%9%Maj JointRepl/Spinal SurgRounded to nearest whole number15Maj Joint Repl/SpinalSurgeryNon-ortho surgery andAcute neurologicPT and OT componentDetermine “Primary Diagnosis Clinical Category” usingonly the ICD-10 code listed first I8000A. Some primarydiagnosis clinical categories may change if there is asurgical procedure done in hospitalOther OrthopedicMedical ManagementIf there was a surgical procedure during inpt stay thatrelates to primary reason for Part A SNF stay, there will becheckboxes in J2000 to assign appropriate category168
10/29/18Primary Diagnosis Clinical CategoryCMS is developing sub-items for item J2000, which will allow providers to report the patient’sprocedural information in a way that uses a checkbox mechanism, and this procedural information willbe used in concert with the patient’s diagnosis information to classify the patient into a clinicalcategory.Other Ortho non-surgicalortho/musculoskeletal andortho surgery not majorjoint repl or spinal sureryExample:S72002S Fracture of unspecified part of neck of left femur, sequela Other orthopedic categoryS72022S with ORIF Other orthopedic categoryS72022S with hip replacement Major joint replacement categoryOther OrthoMajor Joint ReplacementMore dependent function .1617Clinical Category MappingHuge spreadsheet with all the ICD-10CM codes and assignments on CMS or-ServicePayment/SNFPPS/therapyresearch.html189
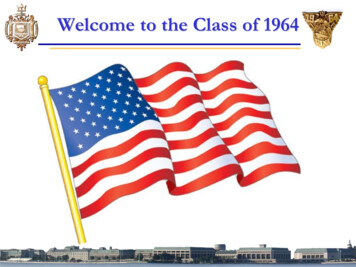
10/29/18Return to Provider: Not deemed appropriate to enter as the primary reason for SNF care. Such codes eitherlack certainty and specificity required to properly categorize a resident under PDPM or the underlying conditioncannot be the main reason of care in SNFs. When a code is returned to a provider, the provider is to select anappropriate ICD-10-CM diagnosis code from the SNF PDPM Clinical Category Mapping available at CMS’website.19Note: categoriesare identical forPT and OT butthey are separatecomponents withseparate CMIsTA0-5Function Score: Lower number is more dependentTBMajor JointReplacement orSpinal SurgeryTE6-9TCTFTI6-9TJNon-ortho surgeryand Acuteneurologic24TGTH2410-230-56-9Medical MgtTMTD0-5Other OrthoPT andOT10-23TK10-23TL0-5TN6-9TO2410-23TP2424 possible PT groups2010
10/29/18Example diagnosesMaj. Joint Repl or Spinal SurgeryM97-periprothetic fracture around internalprosthetic hip & knee joint (other joints under“other ortho”)S12- fracture of neck bonesS22- fracture of ribs, sternum or thoracic spineS32- fracture of lumbar spine and pelvisS34.0-concussion and edema of lumbar and sacral spinal cordS34.101D or S Unspec injury to L1T84-Broken hip & knee prosthesisZ47.1 Aftercare following joint replacement surgery21Exam ple diagnosesOrtho Surgery Not Major Joint Repl/SpinalM96.6- bone fx after insertion of implant, prothesis or plateOrtho Surg that is not MajJoint Repl or Spinal SurgeryOther OrthoM97-Periprothetic fracture around internal prosthetic joint:all others not hip and kneeNon-surgortho/M usculoskeletalFracture, crushing, traumatic amputation of any bones not mentioned so farMechanical complications of implanted devices (fixation devices,plates, etc) for anything other than hip and knee)Complications of reattachment of body partsStump issues: Neuromas, dehiscenceEncounter to remove any device the MD put in and it didn’t go wellEncounter for other orthopedic aftercare2211
10/29/18Clinical CategoryOrtho Surg that is notMaj Joint Repl orSpinal SurgeryOther OrthoPT and OTNon-surgortho/MusculoskeletalMixed bag of other ortho conditions such as: subluxation, avulsion,dislocation, stenosis, some other fractures that often don’t requiresurgery, compression fractures, benign bone/cartilage/etc tumorsSome non-surg ortho will bump to a surgery category if the surgical procedure checkbox applies in J200023Medical MgtPT and OTAcute InfectionsCV and CoagulationsPulmonaryCancerMedical ManagementTITJTKTLCh 1: Certain infectious & parasitic diseases, and someinfections coded in other chapters: ex: Cellulitis, flu,appendicitis, staph arthritis, etc.Ch 3: diseases of blood and blood formingorgans & certain disorders involving immunemechanismCh 9: Diseases of the circulatory systemCh 10: Diseases of the respirator system, and some lungissues from other chapters, ex: traumatic pneumothoraxCh 2: Neoplasms(see next slide)1.131.421.521.092412
10/29/18Sub-category “medical management” under “Medical Management” CategoryMedical ManagementOther: examples - thyroiditis, benign tumors, diabetes,protein-calorie malnutrition, psych, eye, ear, unspecifiedand other CV disease, postthrombotic syndrome,bronchitis, Chrohn’s disease, liver failure, unspecified,pressure ulcers, chronic ulcers, non-pressure,Stress/pathologic fractures (may bump up to surgicalcategory with surgical procedure in J2000), kidney disease,puncture wounds, lacerationsPT and OTNon Ortho surgery & AcuteNeurologicMost any surgery for anything not ortho: GI, GU, trauma, burn, graft, flap,Acute neuro examples. Encephalitis, meningitis, hemiplegia,quadriplegia, brain hemorrhage, effects of stroke and other cerebralevents, some skull fractures, nerve injuries, head injuries, spinal cordinjuries(without surgery), nervous system issues2613
10/29/18RecapClinical CategoryFunction ScorePT & OT CaseM ix Gro upM ajor Joint Replacem ent or Spinal Surgery0-5TAM ajor Joint Replacem ent or Spinal SurgeryM ajor Joint Replacem ent or Spinal SurgeryM ajor Joint Replacem ent or Spinal SurgeryOther OrthopedicOther Orthopedic6-910-23240-56-9TBTCTDTETFOther OrthopedicOther OrthopedicM edical M anagem entM edical M anagem entM edical M anagem entM edical M anagem TNTOTPNon-Orthopedic SurgeryNon-Orthopedic SurgeryNon-Orthopedic SurgeryNon-Orthopedic eurologicNeurologicNeurologicPT CM IOT CM 71.441.541.111.301.491.551.0927SLP ComponentSLP Component: Building BlocksStep 1: Services Count (Tier 1 Category)One point for each:Step 2: (Tier 2)Neither, either,or both?Acute NeurologicComorbidityCognitive ImpairmentMechanicallyAltered dietSSwallowing disorder:Any in K01002814
10/29/18SLP related co-morbiditiesMDS 8000O0100E2O0100F2Acute Neurologic: Same as PT and OT,based on diagnosis code in I8000ADescriptionAphasiaCVA, TIA, or StrokeHemiplegia or HemiparesisTraumatic Brain InjuryLaryngeal CancerApraxiaDysphagiaALSOral CancersSpeech and Language DeficitsTracheostomy Care While a ResidentVentilator or Respirator While a ResidentCognitive Impairment:BIMS 12ORAt least mild impairment: Cognitive skills for daily decisionmaking: modified independence orworse Makes self understood: usually orworse Memory Problem29SLP Categories1. Mechanically altered diet2. Swallowing bothSJSKSL00. None of the 3 conditions1. Acute Neurologic2. Comorbidity3. Cognitive 93015
10/29/18NTA ComponentNon-case-mix component addresses consistent coststhat are incurred for all residents, such as room andboard and various capital related expenses.31Non-therapy ancillaries50 separate items on the MDS assigned a points value,many diagnosis codes in I8000Condition/Extensive ServiceHIV/AIDSParenteral IV Feeding: Level High (51% calories) (not peg tube)Special Treatments/Programs: Intravenous Medication Post-admitCodeSpecial Treatments/Programs: Ventilator Post-admit CodeParenteral IV feeding: Level Low (26% calories/501cc fluid) (not pegtube)Lung Transplant StatusSpecial Treatments/Programs: Transfusion Post-admit CodeMajor Organ Transplant Status, Except LungActive Diagnoses: Multiple Sclerosis CodeOpportunistic InfectionsActive Diagnoses: Asthma COPD Chronic Lung Disease CodeBone/Joint/Muscle Infections/Necrosis - Except: Aseptic Necrosis ofBoneChronic Myeloid LeukemiaWound Infection CodeActive Diagnoses: Diabetes Mellitus (DM) CodeEndocarditisImmune DisordersEnd-Stage Liver DiseaseOther Foot Skin Problems: Diabetic Foot Ulcer CodeMDS ItemSNF Claim ICD-10B20K0510A2 K0710A2Points87O0100H25O0100F2K0510A2 1133216
10/29/18Condition/Extensive ServiceNarcolepsy and CataplexyCystic FibrosisSpecial Treatments/Programs: Tracheostomy Post-admit CodeActive Diagnoses: Multi-Drug Resistant Organism (MDRO) CodeSpecial Treatments/Programs: Isolation Post-admit CodeSpecified Hereditary Metabolic/Immune DisordersMorbid ObesitySpecial Treatments/Programs: Radiation Post-admit CodeHighest Stage of Unhealed Pressure Ulcer - Stage 4Psoriatic Arthropathy and Systemic SclerosisChronic PancreatitisProliferative Diabetic Retinopathy and Vitreous HemorrhageOther Foot Skin Problems: Foot Infection Code, Other Open Lesion onFoot Code, Except Diabetic Foot Ulcer CodeComplications of Specified Implanted Device or GraftBladder and Bowel Appliances: Intermittent catheterizationInflammatory Bowel DiseaseAseptic Necrosis of BoneSpecial Treatments/Programs: Suctioning Post-admit CodeMDS M0300X1I8000I8000I8000M1040A 1111111111111133Condition/Extensive ServiceCardio-Respiratory Failure and ShockMyelodysplastic Syndromes and MyelofibrosisSystemic Lupus Erythematosus, Other Connective Tissue Disorders,and Inflammatory SpondylopathiesDiabetic Retinopathy - Except : Proliferative Diabetic Retinopathy andVitreous HemorrhageNutritional Approaches While a Resident: Feeding Tube (peg tube)Severe Skin Burn or ConditionIntractable EpilepsyActive Diagnoses: Malnutrition CodeDisorders of Immunity - Except : RxCC97: Immune DisordersCirrhosis of LiverBladder and Bowel Appliances: OstomyRespiratory ArrestPulmonary Fibrosis and Other Chronic Lung DisordersMDS 0I5600I8000I8000H0100CI8000I80001111111113417
10/29/18NTA CMINTA ComorbidityScore12 9-116-83-51-20NTA Case ursing ComponentSame major categories as RUG IV 66Extensive Services18% increase in payment fornursing component forresidents with HIV/AIDS (B20on SNF claim)Special Care HighSpecial Care LowClinically ComplexBehavior Symptoms and Cognitive ImpairmentReduced Physical FunctionFunction ScoreInstead of ADL Score0 – 16Lower score more dependentUses hierarchy, not CMIEatingGG0130A1 EatingToiletingHygieneGG0130C1 Toileting HygieneAverageBedMobilityGG0170B1 Sit to LyingAverageTransferGG0170C1 Lying to Sitting on Side ofBedGG0170D1 Sit to StandGG0170E1 Chair/Bed-to-ChairGG0170F1 Toilet Transfer3618
10/29/18Nursing ComponentSame Nursing categories as RUGIV 66,except Function score,resulting in 24 nursing categories.Uses hierarchy, not CMIPDPM PA1Function 130.6637Illustrative Base Rates:3819
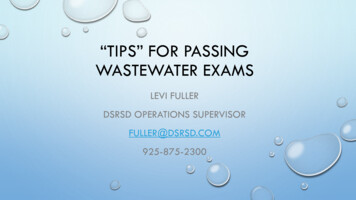
10/29/18Example:Com ponentGroupCMIAmountCommentsPTTC1.88111.54Maj Joint Replacement, PT/OT Function Score: 10OTTC1.6892.79Maj Joint Replacement, PT/OT Function Score: 10SLPSA0.6815.06Nothing to score higherNursingHBC22.23230.72Septicemia, depression, nursing function score 7NTA10.9674.93Chronic pancreatitisNon-CaseMixNANA92.63(Urban rate)Total perdiem617.67Subject to variable per diem adjustment for PT, OTand NTA39Interim Payment Assessment (IPA): NP item set Optional assessment: Facilities will be able to determine whenIPAs will be completed for their patients to address potentialchanges is clinical status and what criteria should be used to decidewhen an IPA would be necessary. “We will seek additional stakeholder input on this issue of criteriafor completion.” An IPA will not stop or change the variable per diem adjustment. The ARD for the IPA will be the date the facility chooses to completethe assessment relative to the triggering event that causes a facilityto choose to complete the IPA. Payment based on the IPA will beginthe same day as the ARD. The IPA will not be susceptible to assessment penalties, given theoptional nature of the assessment.4020
10/29/18Therapy Delivery There will be a combined 25 percent limit onconcurrent therapy and group therapy for eachdiscipline of therapy provided. For example, if a resident received 800 minutes ofphysical therapy, no more than 200 minutes of thistherapy could be provided on a concurrent or groupbasis. Group and concurrent therapy should not be utilized tosatisfy therapist or resident schedules, and all groupand concurrent therapy should be well documented ina specific way to demonstrate why they are the mostappropriate mode for the resident and reasonable andnecessary for his or her individual condition.41Therapy Delivery Therapy delivery items will be added to PartA PPS Discharge Assessment for eachdiscipline: Start and End dates Total individual, concurrent, group minutes Total days If concurrent/group limits exceeded, nonfatal warning on validation report Could be used to deny payment for those staysupon medical review4221
10/29/18Interrupted Stay Policy If resident is discharged from a SNF and returns to the same SNFby midnight at the end of the third day of the interruptionwindow, the resident’s stay will be a continuation of theprevious stay for purposes of both resident classification andthe variable per diem adjustment schedule. If absence exceeds 3-day interruption window, readmission willbe treated as a new stay, in which the resident would receive anew 5-day assessment upon admission and the variable perdiem adjustment schedule would reset to Day 1. If resident readmits to a different SNF, it’s a new stay with new5-day and variable per diem adjustment schedule43Interrupted stay policy changes nothing about OBRA and PPS Discharges(or OBRA MDS schedule) You can be required to do an OBRA/PPS Discharge forwhat may be classified as an “interrupted stay” uponreturn. CMS will revise codes for SNF-QRP so that a hospitaladmission and return to SNF in “interrupted stay” doesnot trigger a new stay for SNF-QRP4422
10/29/18Questions/Discussion4523
T84-Broken hip & knee prosthesis Z47.1 Aftercare following joint replacement surgery Example diagnoses 21 Other Ortho Ortho Surg that is not Maj Joint Repl or Spinal Surgery Non-surg ortho/Musculoskeletal Ortho Surgery Not Major Joint Repl/Spinal M96.6-bone fx after insertion of implant, prothesis or plate