Transcription
CRC Series in Modern Nutrition ScienceHandbook of Minerals asNutritional SupplementsCopyright 2005 by CRC Press, Inc. All Rights Reserved.
CRC Series inModern Nutrition ScienceSeries EditorStacey J. BellIdeasphere, Inc.Grand Rapids, MichiganPhytopharmaceuticals in Cancer ChemopreventionEdited by Debasis Bagchi and Harry PreussHandbook of Minerals as Nutritional SupplementsRobert A. DiSilvestroCopyright 2005 by CRC Press, Inc. All Rights Reserved.
CRC Series in Modern Nutrition ScienceHandbook of Minerals asNutritional SupplementsRobert A. DiSilvestroCRC PR E S SBoca Raton London New York Washington, D.C.Copyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page iv Wednesday, August 18, 2004 10:53 AMLibrary of Congress Cataloging-in-Publication DataDiSilvestro, Robert A.Handbook of minerals as nutritional supplements / Robert DiSilvestro.p. cm.Includes bibliographical references and index.ISBN 0-8493-1652-91. Minerals in human nutrition—Handbooks, manuals, etc. I. Title.QP533.D55 2004613.2′85—dc222004051925This book contains information obtained from authentic and highly regarded sources. Reprinted materialis quoted with permission, and sources are indicated. A wide variety of references are listed. Reasonableefforts have been made to publish reliable data and information, but the author and the publisher cannotassume responsibility for the validity of all materials or for the consequences of their use.Neither this book nor any part may be reproduced or transmitted in any form or by any means, electronicor mechanical, including photocopying, microfilming, and recording, or by any information storage orretrieval system, without prior permission in writing from the publisher.The consent of CRC Press LLC does not extend to copying for general distribution, for promotion, forcreating new works, or for resale. Specific permission must be obtained in writing from CRC Press LLCfor such copying.Direct all inquiries to CRC Press LLC, 2000 N.W. Corporate Blvd., Boca Raton, Florida 33431.Trademark Notice: Product or corporate names may be trademarks or registered trademarks, and areused only for identification and explanation, without intent to infringe.Visit the CRC Press Web site at www.crcpress.com 2005 by CRC Press LLCNo claim to original U.S. Government worksInternational Standard Book Number 0-8493-1652-9Library of Congress Card Number 2004051925Printed in the United States of America 1 2 3 4 5 6 7 8 9 0Printed on acid-free paperCopyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page v Wednesday, August 18, 2004 10:53 AMPrefaceThe Internet, television, and magazines are flooded with nutrition supplement advertisements, with many claims being made for various products. One area with anespecially large recent growth spurt is the mineral supplement area. Moreover, anumber of nutrition business trade journals are projecting that the mineral supplement market should see sustained growth over the next few years. As claims continueto be made for various mineral supplement products, major questions are arising,such as: What research, if any, is behind these claims?Do different forms of mineral supplements have different efficacies?Are these supplements beneficial only for correcting deficiency, or canthere be benefits of eating more than the levels currently recommendedas adequate?What are the safety issues of mineral supplements?These questions are being asked not only by the general public, but also bymany health care professionals, biomedical researchers, and people involved in thenutrition industries themselves. This last group is especially important to publichealth because their marketing can drive the sales of supplements. Therefore, theplayers in nutrition industries, as well as health care professionals and researchers,need a way to evaluate mineral supplement claims. Some information can be obtainedusing a quick search of the Internet, or by using a program like Medline. However,interpretation of the information obtained can be hampered by the lack of a specialized background and time available. For example, if one study says that a calciumsupplement has no effect on blood pressure, and another study says the opposite,how does one reconcile the conflict? Someone with a good biomedical backgroundcan search out the issue, but this can be very time consuming.This book is intended to provide a concise, yet informative presentation andinterpretation of the current state of research on various mineral supplements. Eachof the above-noted questions are addressed. The information should be technicalenough to satisfy a biomedical audience but will avoid jargon used mainly by mineralspecialists. Even so, it’s hard to write this type of a book without using some wordsfor which the definition may not be known. Therefore, this book includes a glossaryfor some words that appear often.As author of this book, I have tried to present more than one perspective forcontroversial areas, but I have also given my opinions on many of them. When Ihave given my opinion, I have tried to clearly state that this is what I am doing.There is no doubt that more research is needed in almost all the areas I coverin this book. In that regard, I have pointed out some of what I think should comeCopyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page vi Wednesday, August 18, 2004 10:53 AMnext in research. At the same time, I recognize that a lot of people, from the generalpublic to the most dedicated researcher, sometimes get frustrated if a report onnutrition or any other subject is totally noncommittal. So, I state what I feel is safeto conclude right now, and I provide some conjectures.My hope is that this book can spur many of us to further consider how mineralsupplements should and should not be used for health promotion and health care.Copyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page vii Wednesday, August 18, 2004 10:53 AMAcknowledgments andConflicts of InterestI would like to thank Gordon Wardlaw for reading and giving feedback on everychapter, and Elizabeth Joseph for a great deal of assistance with the reference aspectsof the book preparation. I would also like to thank Emily Dy for help with referencesin the chapter on iron. In addition, I appreciate the help of each of the following forcomments on individual subjects: Michael Bergeron, Priscilla Clarkson, SteveAbrams, Connie Weaver, Greg Miller, and Greg Wiet. I also appreciate my wife,Janet, and children, David, Daniel, and Lisa, for allowing me the enormous amountof time it took to complete this writing. Finally, I want to express great appreciationto Stacey Bell for having the original concept for the book and helping me get itoff the ground.I endeavored to present the issues in this book as honestly as I could, withouttrying to make any product supplier look better or worse than reality dictated. Evenso, I do want to note the companies that have supported parts of my own mineralresearch: Albion Laboratories, Nutrition 21, Glanbia, and Purac of America.Copyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page ix Wednesday, August 18, 2004 10:53 AMAuthorDr. Robert DiSilvestro is professor of nutrition at The Ohio State University.He earned his Ph.D. in Biochemistry from Texas A&M University in 1982 afterreceiving his Bachelor of Science from Purdue University, where he majored inBiochemistry.DiSilvestro is the author or co-author of more than 70 peer-reviewed, reseachjournal articles. He has also authored several reviews, including an invited reviewof a trace mineral manual for Free Radical Biology & Medicine, a journal.He’s been a featured speaker for a National Institute of Health workshop on thecurrent state of zinc research as well as speaking on minerals for a functional foodsymposium at an annual meeting of the Institute of Food Technology.This is his first book.Copyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page xi Wednesday, August 18, 2004 10:53 AMTable of ContentsChapter 1CalciumOverview of FunctionOverview of MetabolismNutritional Status AssessmentBioavailability from Foods and SupplementsTypical Intakes versus NeedsCurrent Research on Supplement UseRicketsBone in Children and Adolescents without RicketsOsteoporosis Prevention and Treatment in AdultsHyperparathyroidismBlood PressureBlood Lipid AlterationsColon CancerWeight LossToxicitySummary and ConclusionsChapter 2MagnesiumOverview of FunctionOverview of MetabolismNutritional Status AssessmentBioavailability from Foods and SupplementsTypical Intakes Versus NeedsCurrent Research on Supplement UseParenteral Pharmacological UsesOvert Hypomagnesemia (Low Serum Magnesium)Blood PressureSerum Lipids in Non-Diabetic SubjectsPrevention of Cardiovascular Disease in Non-Diabetic eoporosis Prevention or RestrictionChronic FatigueAsthmaCopyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page xii Wednesday, August 18, 2004 10:53 AMBeta-Thalassemia/Sickle Cell AnemiaKidney StonesPregnancy: Premature/Low Birth Weight OutcomesPremenstrual Syndrome (PMS)Mitral Valve ProlapseOther ApplicationsToxicitySummary and ConclusionsChapter 3PotassiumOverview of FunctionOverview of PhysiologyNutritional Status AssessmentBioavailability from Foods and SupplementsTypical Intakes Versus NeedsCurrent Research on Supplement UseHypertensionKidney StonesCrampsPotassium and Exercise PerformancePotassium and Stroke RiskPotassium and OsteoporosisToxicitySummary and ConclusionsChapter 4IronOverview of FunctionOverview of MetabolismNutritional Status AssessmentBioavailability from Foods and SupplementsTypical Intakes Versus NeedsCurrent Research on Supplement UseGeneral Comments on Doses and UsesTreatment and Prevention of Anemia in Individuals withoutOther Discernable Health ProblemsCommunity Interventions for Anemia Treatment and PreventionPremature/Low Birth Weight InfantsRenal Dialysis PatientsCancer PatientsThe ElderlyIron Deficiency without AnemiaPregnancyCognitive and Behavioral DevelopmentInfectionsCopyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page xiii Wednesday, August 18, 2004 10:53 AMExercise PerformanceMiscellaneous Health ProblemsToxicitySummary and ConclusionsChapter 5ZincOverview of FunctionOverview of MetabolismNutritional Status AssessmentBioavailability from Foods and SupplementsTypical Intakes Versus NeedsCurrent Research on Supplement UseOvert Deficiency Correction in ChildrenCorrection of Marginal Zinc Deficiency in Young ChildrenSelected Breast-Fed InfantsPremature InfantsImmune FunctionDown’s SyndromeMacular DegenerationAcneWound HealingZinc–Carnosine and UlcersRheumatoid Arthritis/Crohn’s DiseaseCancer PreventionExerciseHepatitisOsteoporosis PreventionRenal Dialysis PatientsCardiovascular DiseaseDiabetesPregnancyZinc Lozenges and ColdsToxicityCopper DeficiencyImmunosupressionProstate CancerAlzheimer’s DiseaseSummary and ConclusionsChapter 6CopperOverview of FunctionOverview of MetabolismNutritional Status AssessmentBioavailability from Foods and SupplementsCopyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page xiv Wednesday, August 18, 2004 10:53 AMTypical Intakes Versus NeedsCurrent Research on Supplement UseToxicitySummary and ConclusionsChapter 7SeleniumOverview of FunctionOverview of MetabolismNutritional Status AssessmentBioavailability from Foods and SupplementsTypical Intakes Versus NeedsCurrent Research on Supplement UseGeographical Populations with Severe Selenium DeficiencyCancerCardiovascular DiseaseArthritisPancreatitisHuman Immunodeficiency Virus (HIV)Male InfertilityPregnancy MiscarriagesMoodImmune FunctionAsthmaKetogenic Diet in Epilepsy PatientsMiscellaneous Health ProblemsGeneral Antioxidant EffectsToxicitySummary and ConclusionsChapter 8ManganeseOverview of FunctionOverview of MetabolismNutritional Status AssessmentBioavailability from Foods and SupplementsTypical Intakes Versus NeedsCurrent Research on Supplement UseManganese and EpilepsyToxicitySummary and ConclusionsChapter 9ChromiumOverview of FunctionOverview of MetabolismCopyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C00.fm Page xv Wednesday, August 18, 2004 10:53 AMNutritional Status AssessmentBioavailability from Foods and SupplementsTypical Intakes Versus NeedsCurrent Research on Supplement UseBody Weight and Composition AlterationsImproved Glucose ToleranceBeneficial Alterations in Blood Lipid ProfilesIndirect Antioxidant ActionsToxicitySummary and ConclusionsChapter 10 Other MineralsPhosphorusIodineUltratrace MineralsGlossaryCopyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C01.fm Page 1 Tuesday, August 17, 2004 7:47 AM1CalciumCalcium is currently one of the most used nutritional supplements. Most of thisinterest comes in relation to osteoporosis prevention or treatment, though other usesalso spring up. There are many types of supplements on the market and differentmessages on how they should be taken. One thing seems certain: Calcium supplementation will remain popular for the foreseeable future.OVERVIEW OF FUNCTIONCalcium, as part of calcium phosphate, is the main structural component of bonesand teeth.1 In addition, calcium is involved in a long list of reversible activating andregulatory actions.1 In fact, calcium movements in and out of cells or cell organellesare essential to many basic physiological functions, including neurological actionsand cardiac muscle contraction.2 Part of calcium’s functions inside cells is to act aswhat is called a “second messenger.”2 This name arises because the shifting ofcalcium between pools is often a way that a hormone or other signaling moleculestarts a process within a cell. In addition to intracellular second messenger functions,calcium also seems to serve as an extracellular messenger outside cells.3 Calciumis well suited to the activator/regulator roles, because this metal is a strong enoughchelate former to complex with a signaling molecule, such as a receptor, but a weakenough chelate former to also fall back off the molecule.The bone function of calcium seems to be better preserved than the activator/regulator functions, since bone releases some calcium if the body’s supply falls off.1However, not all activating/regulatory functions are necessarily preserved perfectlyin times of low calcium supply.OVERVIEW OF METABOLISMThe activator/regulator functions are so essential to life, and are so sensitive tochanges in calcium concentrations, that the body needs powerful mechanisms tomaintain calcium homeostasis. These mechanisms exist especially for plasma calcium levels, and for the transport of calcium in and out of cells and in and out ofcell organelles.4 This movement maintains the cytoplasmic concentration of ionizedcalcium (calcium ion in a relatively unbound state) in the micromolar range (overa thousand-fold less than plasma calcium concentrations). This low cytoplasmiccalcium ion concentration is essential to calcium’s second messenger functioning.Copyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C01.fm Page 2 Tuesday, August 17, 2004 7:47 AMOtherwise, small calcium ion fluxes would not impact the cellular environmentenough to send signals.About 1% of bone calcium exchanges freely with extracellular fluid and, therefore, is available for resisting changes in plasma calcium concentrations.5 Normally,about 40% of blood calcium is bound to plasma proteins, primarily albumin. Theremaining 60% includes ionized calcium plus calcium complexed with phosphateand citrate.Calcium absorption from the intestine, as well as movement between bone andblood, revolves around vitamin D-derived hormones, parathyroid hormone, and, toa lesser extent, calcitonin.4,5 Parathyroid hormone is released into the blood inresponse to decreases in plasma calcium. This action rapidly increases plasmacalcium due to actions such as increased intestinal absorption of calcium, increasedcalcium retention by the kidney, and release of calcium from bone (bone resorption).Vitamin D hormones, especially 1′25-dihydroxycholecalciferol, also increase intestinal calcium absorption and bone resorption. The intestinal effect works in part byincreasing calcium binding proteins, which increase calcium absorption. This typeof absorption regulation is the opposite of what is seen for iron or zinc. With thesemetals, intestinal binding proteins decrease absorption. Thus, calcium absorption isincreased by active regulation, but iron and zinc absorption is increased passivelyby diminishing barriers to absorption.Calcitonin tends to lower plasma calcium concentration by increasing celluptake, renal excretion, and bone formation.4,5 The effects of calcitonin on bone aremuch weaker than those of either PTH or vitamin D.Vitamin D hormones, in addition to regulating calcium absorption and boneresorption, are involved in promoting some of calcium’s regulatory functions.5NUTRITIONAL STATUS ASSESSMENTPlasma or serum total or ionized calcium is sometimes used to assess calciumnutritional status and for short-term assessments of calcium absorption. When thereare large changes in calcium status, such as with the correction of severe calciumdeficiency rickets, serum calcium can show small changes.6 However, usually serumcalcium measurement is not useful for assessing calcium status because, as justmentioned, serum calcium levels are regulated heavily.5 Sometimes, parathyroidhormone readings are done since they respond to fluxes in plasma calcium, thoughthis is not the only influence.5 Other alternatives are reviewed by Cashman andFlynn.7 One is a calcium retention test, which utilizes urinary calcium. Anotherapproach is the use of functional indices such as blood and urine markers of bonemetabolism. Since these markers are affected by multiple factors, their prime use isfor monitoring calcium intervention studies (i.e., to compare values before and afterincreased calcium intake). For population, long-term calcium status assessment,sometimes diet analysis is used, with the results compared to bone density or markersof bone metabolism.6Copyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C01.fm Page 3 Tuesday, August 17, 2004 7:47 AMBIOAVAILABILITY FROM FOODS AND SUPPLEMENTSCalcium absorption from different foods is known to vary. The classic “high bioavailability” food group is diary products, while the classic “low bioavailability”food is spinach, where most calcium is in the water-insoluble oxalate form.1 Somefood components, such as the compound phytate, are known to inhibit calciumabsorption.1High dietary protein has been said to both increase and decrease calcium balance,and consequently bone strength.8 One attempt to reconcile this conflict has beenmade by Dawson-Hughes.9 She notes that on the one hand, dietary protein stimulatesthe production of insulin-like growth factor-1 (IGF-1), which promotes osteoblastmediated bone formation. On the other hand, dietary protein also increases urinarycalcium losses by several proposed mechanisms. According to the Dawson-Hugheshypothesis, the influence that predominates depends on dietary calcium intake (athigh intake, the positive effect is more prominent). By that author’s own admission,some but not all studies support the hypothesis. Possibly, the hypothesis is generallytrue, but some other factors may come into play.In this author’s opinion, the key to the protein–calcium issue is to eat adequatecalcium. If that is done, then even if high protein intake does have negative effects,they may not be enough to seriously affect calcium functional status.Many different calcium complexes have been marketed for pill or capsuleconsumption or to fortify foods. A number of these have been used in studieswhere the supplement produces some effect associated with improved bone health(Table 1.1).TABLE 1.1Examples of CalciumComplexes That GivePositive Results in BoneStudiesCarbonate*CitrateCitrate malateAcetatePhosphateGluconateLactate* Calcium carbonate can be in a relatively isolated form or part of a naturalpreparation such as eggshell or coralcalcium.Copyright 2005 by CRC Press, Inc. All Rights Reserved.
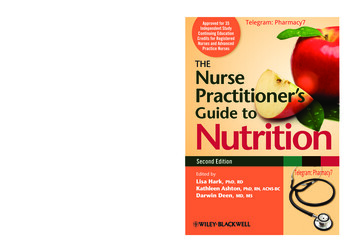
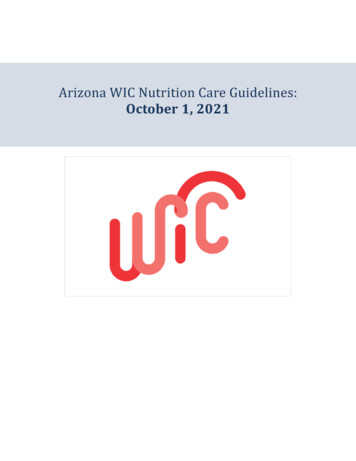
1652 C01.fm Page 4 Tuesday, August 17, 2004 7:47 AMThe fact that all forms of calcium named in Table 1.1 have been able to producepositive effects on bone health suggests that all can be used effectively by people.There are also a few studies that show similarities in absorption rates betweendifferent calcium supplements. For example, in rats, the apparent calcium absorptionis reported to be the same from carbonate, gluconate, oyster shell, and bovine bone.10On the other hand, calcium citrate has been reported to have better absorption thancalcium carbonate, though this finding is not completely uniform.11,12,13 One reasonfor the diverse results could be that a number of different evaluation criteria havebeen used. It has also been suggested that the vitamin D and estrogen status of thesubjects may affect comparisons between different types of calcium supplements.13Whatever the reason for the differing results, some health care professionals andsome researchers emphasize the better absorption potential of calcium citrates, whileothers point out that carbonate, at worst, still works nearly as well, is cheaper, andrequires smaller delivery vehicle mass (due to more calcium per total complexweight). Another consideration can be GI tract tolerability. Some people have somedistress with carbonate, though this may be lessened by splitting the daily dose intotwo ingestion times. Also, the GI tract distress may be temporary in many people.However, for people with health problems, the antacid effect of calcium carbonatemay be undesirable in the long term.Another kind of calcium supplement is milk extract calcium, such as that soldby Glanbia Ingredients Inc. This author’s laboratory has completed a small pilotstudy with this product. In a short intervention (six weeks), the milk calcium productproduced a small decrease in a marker of bone degradation, which was not seen forcalcium carbonate (Figure 1.1).Calcium phosphate, due to its high water solubility, is used to fortify drinks likesoy milk and is part of the calcium fortification in some orange juices. This formof calcium is also used in some pills because it is well tolerated by people who mayhave GI tract issues with calcium carbonate.Calcium lactate finds its way into some food and pharmaceutical applications,sometimes mixed with calcium gluconate. For food applications, calcium lactate hasdesirable properties in terms of neutral flavor and stability. Calcium lactate is wellabsorbed14 and, in a rat study,15 shows better bone-stimulating activity than calciumcarbonate or citrate. Calcium lactate is also sold as pills and as powder that aconsumer can mix into drinks at home. This can be an economical alternative tosome other forms of calcium supplementation.Coral calcium, which is a type of calcium carbonate supplement, has been thesubject of many extravagant claims. Along these lines, some Internet sites state thatthe many merits of coral calcium have been extensively researched. However, thepapers cited on these websites generally do not actually involve studies of coralcalcium. Instead, the research deals with calcium function in general, including manyregulatory functions that are not even known to be affected by typical variations incalcium intake. In reality, only one original research paper relevant to coral calciumsupplements appears in a Medline search of “coral calcium human.”16 This paperreports that in an acute test of calcium uptake, in a small number of people, onetype of coral calcium preparation fares better than another type of calcium carbonate.Copyright 2005 by CRC Press, Inc. All Rights Reserved.
20*181614121086420PREPOSTCaCarbonatePREPOSTMilk CaFIGURE 1.1 Bone specific alkaline phosphatase response to calcium supplementation as calcium carbonate or a milk calcium extract. Young adultfemales were given about 700 mg calcium/day for six weeks. Values are Units/L SEM. *Significantly different from pretreatment (p 0.05, paired t-test).Copyright 2005 by CRC Press, Inc. All Rights Reserved.1652 C01.fm Page 5 Tuesday, August 17, 2004 7:47 AM22
1652 C01.fm Page 6 Tuesday, August 17, 2004 7:47 AMHowever, this study does not compare coral calcium with calcium citrate, whichmay be better absorbed than calcium carbonate.Some coral calcium advertisements claim superiority to other calcium supplements based partly on the inclusion of magnesium. However, the amount of magnesium varies. Moreover, there is no data presented to demonstrate how well thismagnesium is absorbed in the presence of the calcium. Another highly advertisedclaim of coral calcium is that it can affect various aspects of health by manipulatingbody pH. This claim has no research backing. In regard to another issue, coralcalcium is often presented as the reason for the longevity of certain Okinawans.However, there is no actual research data to indicate that coral calcium intake iswhat is responsible for any of the longevity. Therefore, considering all these issuesrelated to coral calcium, there is no clear research justification for the extra expensecompared to other calcium supplements.Some calcium complexes have found a niche for specialized applications. Inthese applications, attention must often be given to the effects of calcium complexon pH as well as other chemical actions. For example, calcium gluconate is usedfor some infant formulas and TPN solutions. On the other hand, this form of calciumhas not had tremendous popularity in pill or capsule form because of the relativelylow percentage of calcium. This means a person has to take more or bigger calciumgluconate pills per dose compared to calcium carbonate. Even so, based on a ratstudy,10 calcium gluconate may have one selling point: Rats fed a calcium gluconatediet had a higher apparent absorption of magnesium than the rats fed the othercalcium supplements, possibly because the gluconate stimulates magnesiumabsorption.This observation for gluconate contrasts a concern that calcium supplements canantagonize magnesium absorption. For this reason, some people avoid taking amixture of the two minerals, since each mineral may impair the absorption of theother. In contrast, some people take supplements that mix calcium and magnesium.The feeling is that the possible loss in absorption of each mineral is compensatedby the increased intake of each. There is also another reason why some people feelthat if one takes calcium, then one should also take magnesium. This reason is thathigh body calcium-to-magnesium ratios have been stated to be problematic. Theconcerns about this ratio, as well as possible impairment of magnesium absorptionby calcium, are covered below in the Toxicity section. The opposite issue, magnesiumimpairing calcium absorption, is covered in the Magnesium chapter under Toxicity.Calcium supplement bioavailability may be affected by the ability of the pillitself to dissolve. A website put out by Kansas State University (http://www.oznet.ksu.edu/ext f&n/ timely/calcium.htm) suggests buying brand-name calcium supplements because the solubility may be better. The site also suggests testing the abilityof a calcium pill to dissolve in 6 ounces of vinegar in 30 minutes.Two other factors have been considered in regard to calcium supplement bioavailability. These are the timing around meals and the splitting of the daily doseinto different ingestion times. The latter seems to help with calcium absorption,8with 500 mg or less per single ingestion time as a common recommendation. Thetiming with meals is a less-settled issue. Calcium carbonate may be better takenCopyright 2005 by CRC Press, Inc. All Rights Reserved.
1652 C01.fm Page 7 Tuesday, August 17, 2004 7:47 AMwith meals, since the acid involved in food digestion can help dissolve calciumcarbonate. Some groups, including an NIH panel, have recommended between mealsas the time to take other calcium supplements. For these other forms of calcium, anempty stomach may work fine, but is it an advantage to taking between meals? Oneadvantage may be avoiding food components that may interfere with calcium absorption. However, it should be noted that some calcium supplements have shown goodabsorption properties even when taken with a meal.17 Thus, this author feels that atpresent, as far as calcium supplement absorption goes, there is no compelling reasonto favor either with meals or between meals. On the other hand, for people proneto kidney stones, taking calcium with meals may present a distinct advantage (seebelow).TYPICAL INTAKES VERSUS NEEDSThere has been considerable debate as to what constitutes “needs” for calcium. Itis safe to say that many people of different ages and circumstances do not eat RDAlevels of calcium consistently.8 Possible consequences of such eating behavior arebeing elucidated by supplement studies (considered in the next section).Calcium is rather unique among nutrient minerals in that when discussing thismineral, the phrase “deficiency” is not mentioned very often. This is a little strangesince, in essence, most proposed calcium supplement uses are primarily intended ascorrection of marginal calcium deficiency. Even so, this term is not brought up much.Severe calcium deficiency is not reported to any large degree in the biomedicalliterature. The one exception pertains to childhood rickets. Although vitamin Ddeficiency is the typical diagnosed cause of this,1 calcium deficiency can also playa role.6 The use of calcium supplements in this situation is discussed in the nextsection.CURRENT RESEARCH ON SUPPLEMENT USERICKETSRickets is a name for a pattern of bone development impairment generally ascribedto a vitamin D deficiency.1 Since vitamin D promotes calcium absorpt
The consent of CRC Press LLC does not extend to copying for general distribution, for promotion, for creating new works, or for resale. Specific permission must be obtained in writing from CRC Press LLC . Handbook of minerals as nutritional supplements / Robert DiSilvestro. p. cm. Includes bibliographical references and index. ISBN 0-8493 .