Transcription
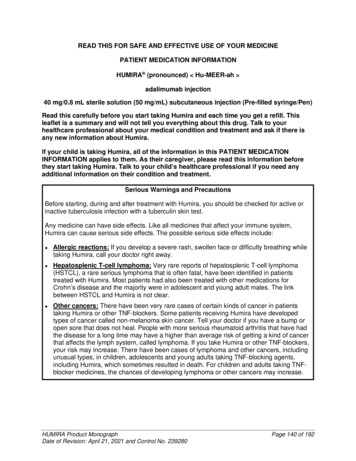
HUMIRA (ADALIMUMAB)PRIOR REVIEW/CERTIFICATION FAXBACK FORMINCOMPLETE FORMS MAY DELAY PROCESSINGALL NC PROVIDERS MUST PROVIDE THEIR 5 DIGIT BCBSNC PROVIDER ID# BELOWPRESCRIBER NAMEPRESCRIBER NPI [REQUIRED]CONTACT PERSONPRESCRIBER PHONEPRESCRIBER ADDRESSCITYPATIENT NAMEBCBSNC PROV ID # / TAX ID [out of state onPRESCRIBER FAXSTATEBCBSNC IDZIPFormulary Drug? Yes NoDATE OF BIRTHGENDERMPLEASE ANSWER THE FOLLOWING QUESTIONS:FDiagnosis Code:1. Is the patient 18 years of age or older?. Yes No2. Will the patient be using Humira in combination with other biologic agents?. Yes NoPlease check the appropriate diagnosis and answer the related questions; if requesting over the quantitylimit please complete bottom of page 2: Active Ankylosing Spondylitis Moderate to Severe Hidradenitis Suppurativaa. Is the patient a new start to therapy with Humira and requires a starting dose?. Yes No Chronic Moderate to Severe Plaque Psoriasisa. Is the patient being managed by a dermatologist?. Yes Nob. Does the patient have Body Surface Area (BSA) involvement of at least 5% or involvement of thepalms, soles, head and neck, or genitalia, causing disruption in normal activities and/oremployment?. Yes Noc. Has the patient tried and failed or is intolerant to systemic therapy (e.g., Methotrexate, Cyclosporine,Acitretin)?. Yes NoIf No, does the patient have a clinical contraindication to systemic therapy? Yes Nod. Has the patient tried and failed or is intolerant to phototherapy?. Yes NoIf No, does the patient have a clinical contraindication to phototherapy?. Yes Noe. Is the patient a new start to therapy with Humira and requires a starting dose?. Yes No Active Rheumatoid Arthritisa. Has the patient tried and failed methotrexate therapy?. Yes NoIf NO, does the patient have a clinical contraindication to methotrexate?. Yes No Active Psoriatic Arthritisa. Has the patient tried and failed or is intolerant to systemic therapy (e.g., Methotrexate, Cyclosporine,Acitretin)?. Yes NoIf NO, is the patient unable to receive or has a clinical contraindication to systemic therapy (e.g.,Methotrexate, Cyclosporine, Acitretin)?. Yes No Active, Moderate to Severe, Polyarticular Juvenile Idiopathic Arthritisa. Is the patient 2 years of age or older?. Yes Nob. Has the patient experienced a therapeutic failure or had an inadequate response tomethotrexate?. Yes NoIf NO, is the patient unable to receive or has a clinical contraindication to methotrexate? Yes No**continued on page 2; sign page 2 for prior authorization**For BCBSNC members, fax form to 1-800-795-9403BLUE CROSS , BLUE SHIELD and the Cross and Shield Symbols are registered marks of the Blue Cross and Blue Shield Association, anassociation of independent Blue Cross and Blue Shield Plans. BCBSNC is an independent licensee of the Blue Cross and Blue ShieldAssociation. All other marks are the property of their respective owners.Last Revision Date: April 2017Page 1
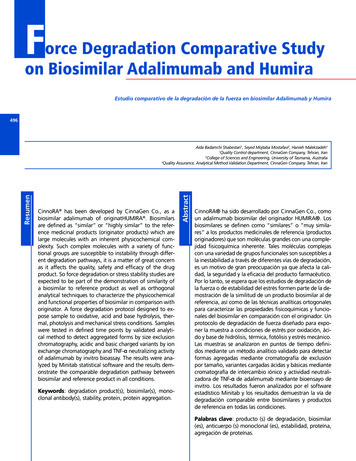
HUMIRA (ADALIMUMAB) cont.PRESCRIBER NAMEPRESCRIBER NPI [REQUIRED]CONTACT PERSONPRESCRIBER PHONEPRESCRIBER ADDRESSPATIENT NAMECITYSTATEBCBSNC IDBCBSNC PROV ID # / TAX ID [out of state onPRESCRIBER FAXZIPFormulary Drug? Yes NoDATE OF BIRTHGENDERMF**continued from page 1; sign page 2 for prior authorization** Active, Moderate to Severe, Ulcerative Colitisa. Has the patient experienced a therapeutic failure or inadequate response to conventional therapy(e.g., corticosteroids, 5-aminosalicylate, azathioprine, 6-mercaptopurine, metronidazole,methotrexate)?. Yes NoIf NO, is the patient unable to receive or has a clinical contraindication to conventional therapy (e.g.,corticosteroids, 5-aminosalicylate, azathioprine, 6-mercaptopurine, metronidazole,methotrexate)?. Yes Nob. Is the patient a new start to therapy with Humira and requires a starting dose?. Yes No Active, Moderate to Severe, Crohn’s Diseasea. Is the patient 6 years of age or older?. Yes Nob. Has the patient experienced a therapeutic failure or inadequate response to conventional therapy(e.g., corticosteroids, 5-aminosalicylate, azathioprine, 6-mercaptopurine, metronidazole,methotrexate)?. Yes NoIf NO, is the patient unable to receive or has a clinical contraindication to conventional therapy (e.g.,corticosteroids, 5-aminosalicylate, azathioprine, 6-mercaptopurine, metronidazole,methotrexate)?. Yes Noc. Is the patient a new start to therapy with Humira and requires a starting dose?. Yes No Noninfectious Uveitisa. Is the patient 18 years of age or older?. Yes Nob. Does the patient have a diagnosis of noninfectious intermediate, posterior, or pan uveitis? Yes Noc. Has the patient tried and failed, is intolerant to, or has a clinical contraindication to glucocorticoidtherapy?. Yes Nod. Is the patient a new start to therapy with Humira and requires a starting dose?. Yes No Other (please provide condition and rationale):**PLEASE NOTE : If prescribing greater than 2 syringes/pens per 28 days, please complete page 3 **Please certify the following by signing and dating below: I certify that I have been authorized to request prior review andcertification for the above requested service(s). I further certify that my patient’s medical records accurately reflect the informationprovided. I understand that BCBSNC may request medical records for this patient at any time in order to verify this information. Ifurther understand that if BCBSNC determines this information is not reflected in my patient’s medical records, BCBSNC mayrequest a refund of any payments made and/or pursue any other remedies available.Prescriber’s Signature (Required): Date:For BCBSNC members, fax form to 1-800-795-9403BLUE CROSS , BLUE SHIELD and the Cross and Shield Symbols are registered marks of the Blue Cross and Blue Shield Association, anassociation of independent Blue Cross and Blue Shield Plans. BCBSNC is an independent licensee of the Blue Cross and Blue ShieldAssociation. All other marks are the property of their respective owners.Last Revision Date: April 2017Page 2
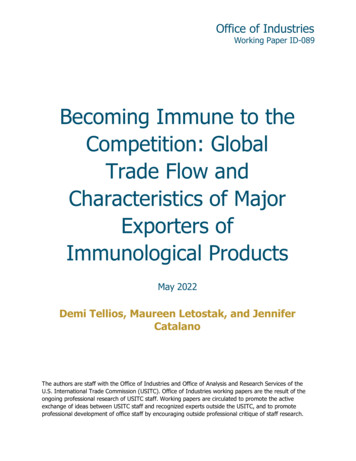
COMPLETE PAGE 3 ONLY IF REQUESTING A QUANTITY LIMIT EXCEPTIONFOR HUMIRA (ADALIMUMAB)PRESCRIBER NAMEPRESCRIBER NPI [REQUIRED]CONTACT PERSONPRESCRIBER PHONEPRESCRIBER ADDRESSCITYPATIENT NAMESTATEBCBSNC IDBCBSNC PROV ID # / TAX ID [out of state onPRESCRIBER FAXZIPFormulary Drug? Yes NoDATE OF BIRTHGENDERMFIf you are requesting a quantity above 2 syringes/pens per 28 days, check the appropriate box andprovide the medical necessity of the increased dosage requested.QUANTITY LIMIT EXCEPTIONPlease note: This medication requires a prior authorization before a quantity limit override can be considered.Before submitting a request for a quantity limit override, please ensure that a prior approval authorization has beensubmitted and/or approved (page 1). Otherwise, this request will deny.Diagnosis Code:Quantity limit of 2 syringes/pens per 28 days1. Is the member currently taking methotrexate?. Yes No2. Please check one dose below: 10mg/0.2 mL syringe 20 mg/0.4 mL syringe 40 mg/0.8 mL syringe 40 mg/0.8 mL pen - injector# of syringes / pens per 28 days:Please enter quantity as a numeric value with one decimal place (ex. 1.0, 1.5)In the space provided, please document support for the requested Quantity Limit Exception (this mayinclude documented clinical rationale and/or medical records). If none, write N/A.Please certify the following by signing and dating below: I certify that I have been authorized to request priorreview and certification for the above requested service(s). I further certify that my patient’s medical recordsaccurately reflect the information provided. I understand that BCBSNC may request medical records for thispatient at any time in order to verify this information. I further understand that if BCBSNC determines thisinformation is not reflected in my patient’s medical records, BCBSNC may request a refund of any paymentsmade and/or pursue any other remedies available.Prescriber’s Signature (Required): Date:For BCBSNC members, fax form to 1-800-795-9403BLUE CROSS , BLUE SHIELD and the Cross and Shield Symbols are registered marks of the Blue Cross and Blue Shield Association, anassociation of independent Blue Cross and Blue Shield Plans. BCBSNC is an independent licensee of the Blue Cross and Blue ShieldAssociation. All other marks are the property of their respective owners.Last Revision Date: April 2017Page 3
Non-Discrimination and Accessibility NoticeDiscrimination is Against the Law Blue Cross and Blue Shield of North Carolina (“BCBSNC”) complies withapplicable Federal civil rights laws and does not discriminate on the basis ofrace, color, national origin, age, disability, or sex. BCBSNC does not exclude people or treat them differently because of race,color, national origin, age, disability, or sex.BCBSNC: Provides free aids and services to people with disabilities to communicateeffectively with us, such as:- Qualified interpreters- Written information in other formats (large print, audio, accessibleelectronic formats, other formats) Provides free language services to people whose primary language is notEnglish, such as:- Qualified interpreters- Information written in other languages If you need these services, contact Customer Service 1-888-206-4697, TTYand TDD, call1-800-442-7028. If you believe that BCBSNC has failed to provide these services ordiscriminated in another way on the basis of race, color, national origin, age,disability, or sex, you can file a grievance with: BCBSNC, PO Box 2291, Durham, NC 27702, Attention: Civil RightsCoordinator- Privacy, Ethics & Corporate Policy Office, Telephone 919765-1663, Fax 919-287-5613, TTY 1-888-291-1783civilrightscoordinator@bcbsnc.com You can file a grievance in person or by mail, fax, or email. If you need helpfiling a grievance, Civil Rights Coordinator - Privacy, Ethics & Corporate PolicyOffice is available to help you. You can also file a civil rights complaint with the U.S. Department of Healthand Human Services, Office for Civil Rights, electronically through the Officefor Civil Rights Complaint Portal, available athttps://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at: U.S.Department of Health and Human Services 200 Independence Avenue, SWRoom 509F, HHH Building Washington, D.C. 20201 1-800-368-1019, 800BLUE CROSS , BLUE SHIELD and the Cross and Shield Symbols are registered marks of the Blue Cross and Blue Shield Association, anassociation of independent Blue Cross and Blue Shield Plans. BCBSNC is an independent licensee of the Blue Cross and Blue ShieldAssociation. All other marks are the property of their respective owners.Last Revision Date: April 2017Page 4
537-7697 (TDD). Complaint forms are available athttp://www.hhs.gov/ocr/office/file/index.html. This Notice and/or attachments may have important information about yourapplication or coverage through BCBSNC. Look for key dates. You may needto take action by certain deadlines to keep your health coverage or help withcosts. You have the right to get this information and help in your language atno cost. Call Customer Service 1-888-206-4697.ATTENTION: If you speak another language, language assistance services, free ofcharge, are available to you. Call 1-888-206-4697 (TTY: 1-800-442-7028).ATENCIÓN: Si habla español, tiene a su disposición servicios gratuitos de asistencialingüística. Llame al 1-888-206-4697 (TTY: ��通話, � 1-888-2064697(TTY:1-800-442-7028)。CHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ miễn phí dành cho bạn.Gọi số1-888-206-4697 (TTY: 1-800-442-7028).주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수있습니다.1-888-206-4697 (TTY: 1- 800-442-7028)번으로 전화해 주십시오.ATTENTION : Si vous parlez français, des services d'aide linguistique vous sontproposés gratuitement. Appelez le 1-888-206-4697 (ATS : 1-800-442-7028). اتصل برقم . فإن خدمات المساعدة اللغوية تتوافر لك بالمجان ، إذا كنت تتحدث اللغة العربية : ملحوظة .1-800-442-7028 : المبرقة الكاتبة .1-888-206-4697LUS CEEV: Yog tias koj hais lus Hmoob, cov kev pab txog lus, muaj kev pab dawb raukoj. Hu rau1-888-206-4697 (TTY: 1-800-442-7028).ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатныеуслуги перевода. Звоните 1-888-206-4697 (телетайп: 1-800-442-7028).PAUNAWA: Kung nagsasalita ka ng Tagalog, maaari kang gumamit ng mga serbisyo ngtulong sa wika nang walang bayad. Tumawag sa 1-888-206-4697 (TTY: 1-800-4427028).સુચના: જો તમે ગુજરાતી બોલતા હો, તો નન:સુલ્કુ ભાષા સહાય સેવાઓ તમારા માટે ઉપલબ્ધ છે . ફોન કરો1-888-206-4697 (TTY: 1-800-442-7028).ចំណំ៖ �ិយាយជាភាសាខ្មែរ �កភាសាមាននតលជ់ ��្ទំនាក់ទនំ ងតាម្រយៈបលម៖ 1-888-206-4697 (TTY: 1-800-442-7028)។BLUE CROSS , BLUE SHIELD and the Cross and Shield Symbols are registered marks of the Blue Cross and Blue Shield Association, anassociation of independent Blue Cross and Blue Shield Plans. BCBSNC is an independent licensee of the Blue Cross and Blue ShieldAssociation. All other marks are the property of their respective owners.Last Revision Date: April 2017Page 5
ACHTUNG: Wenn Sie Deutsch sprechen, stehen Ihnen kostenlos sprachlicheHilfsdienstleistungen zur Verfügung. Rufnummer: 1-888-206-4697 (TTY: 1-800-4427028).ध्यान दें: यदद आप दिन्दी बोलते िैं तो आपके दलए मफ्ु त में भाषा सिायता सेवाएं उपलब्ध िैं। 1-888206-4697 (TTY: 1-800-442-7028) पर कॉल करें ।້ າພາສາ ລາວ, ການບໂປດຊາບ: ຖ້ າວ່ າທ່ ານເວໍ ິ ລການຊ່ ວຍເຫ້ ານພາສາ, ໂດຍບໍ່ ເສ່ າ,ຼື ອດັ ຽຄແມ່ ນມ້ ອມໃຫ້ ທ່ ານ. ໂທຣ 1-888-206-4697 (TTY: 1-800-442-7028).ີ ��。1888-206-4697(TTY: ください。BLUE CROSS , BLUE SHIELD and the Cross and Shield Symbols are registered marks of the Blue Cross and Blue Shield Association, anassociation of independent Blue Cross and Blue Shield Plans. BCBSNC is an independent licensee of the Blue Cross and Blue ShieldAssociation. All other marks are the property of their respective owners.Last Revision Date: April 2017Page 6
patient at any time in order to verify this information. I further understand that if BCBSNC determines this information is not reflected in my patient's medical records, BCBSNC may request a refund of any payments