Transcription
BPCI-A Update & Trends inValue Based Specialty CareMarch 11, 2021Proprietary and confidential1
Today’s PresentersDave Terry, CEOArchway HealthArchway Health / info@archwayha.com / (617) 209-7985Don Schreiner, CEOOrthoIllinoisKeely Macmillan, SVPPolicy & Solutions ManagementArchway HealthProprietary and confidential2
OutlineBPCI-A Update Model Year 4 Programmatic Changes Recent Market Changes Participation Consideration for Orthopedic GroupsTrends in Value Based Specialty Care Commercial Market Medicare Direct Contracting ProgramQuestions & AnswersArchway Health / info@archwayha.comProprietary and confidential3
BPCI-A prietary4
BPCI-A Update: MY4 Programmatic Changes Shift from bundles to service lines Orthopedic & Spine SLs Updated MY4 pricing model Switch back to “Realized Trend,” No longer prospective trend Advantageous for MJRLE Removal of PGP Offset Prices tied exclusively to hospital, not group More specific Risk Adjusters for MJRLE related proceduresArchway Health / info@archwayha.comProprietary and confidential5
MY4 Orthopedic Service LinesArchway Health / info@archwayha.comProprietary and confidential6
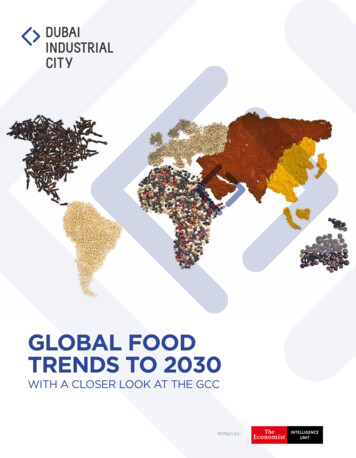
Changes in PGP Prices MY1-MY3 vs MY4ModelYear 4ModelYear 3In MY1-3, the historical efficiency of the PGP impacted the price through the PGP Offset. InMY4 the PGP Offset is no longer applied. As such historical performance for the PGP doesnot affect Baseline or Reconciliation prices.PGP PundlePricePGP BundlePrice HospitalBenchmark Price HospitalBenchmark PricexPGP RelativeCase MixxPGP RelativeCase MixAccounts for the PGP’s case-mixrelative to ACH’s case-mix. Archway Health 2021xPGPOffsetxPeer GroupTrend (PGT)AdjusterMakes Trend Factorretrospective.Proprietary and confidential
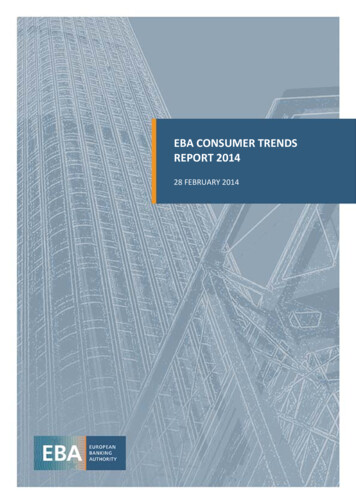
Additional MJRLE Risk Adjusters1.Partial Knee Arthroplasty,2.Total Knee Arthroplasty,3.Partial Hip Arthroplasty,4.Total Hip Arthroplasty and Hip Resurfacing5.Ankle and Reattachments# of EpisodesIn MY3, Major Joint of Lower Extremity Bundles were set too high for knee procedures, and too low for hipprocedures. In MY4, the nuances in the costs of various procedures is introduced to the target price predictions bycreating sub-groups of patients with the following procedures.MJRLE (Combined)MJRLE (Knee)MJRLE (Hip)Episode Expenditures With this change the general differences in costs for treating patients with a Partial/Total Knee Arthroplastyor Partial/Total Hip Arthroplasty vs. those without are also reflected in different target prices. Similar patients who had the same (PCMA/Target Price) in MY3 will now have different PCMA/TargetPrices for each combination of the above risk factors. This corrects the generally high target prices for knees (lower) and low prices for hips (by raising these)Archway Health / info@archwayha.comProprietary and confidential8
BPCI-A Update: Market Changes Large Orthopedic convener stopped offering BPCI-A convener servicesin early December Episode Initiators with that Convener no longer able to participate in the program astraditional EIs Medicare unable to allow EIs to switch conveners or become ownconvener All dropped EIs removed from program effective 1/1/21 Only way for non-participating Ortho Surgeons to move forward in MY4of BPCI-A is to shift Medicare billing to a participating Medicare TINArchway Health / info@archwayha.comProprietary and confidential9
BPCI-A Participation Considerations for Ortho Groups1. Select surgeons to participate High episodic volume Strong historical quality & episodic cost performance2. Select a convener partner able to assignsurgeons to a participating TIN This specific structure needs to be established Specific legal agreements and billing model required3. Work with a convener who will provideaccess to your historical data Absolutely allowed by CMS Assess historical performance vs prices Benchmark opportunities for improvement4. There are no CMS imposed deadlines Surgeon NPIs can re-assign Medicare billing to a new TINat anytime5. Maintain your own Medicare billing Important for managing funds flow and FFS billingreconciliations6. Leverage BPCI-A to prepare for newVBC contracting opportunities Archway Health / info@archwayha.comMedicare Direct ContractingMedicare AdvantageCommercialDirect to EmployerProprietary and confidential10
BPCI-A Data AccessBPCI Advanced Participation Agreement12.2.G (page 58) The Participant (convener) may reuse original or derivative data without prior written authorizationfrom CMS for clinical treatment, care management and coordination, quality improvement activities, and healthcareprovider incentive design and implementation, but shall not disseminate individually identifiable original or derivedinformation from the files specified in the Data Request and Attestation to anyone who is not a HIPAA CEDownstream Episode Initiator or Participating Practitioner (or is) the Participant’s sub-BA, which is hired bythe Participant to carry out work on behalf of the CE Downstream Episode Initiators or ParticipatingPractitioners.Email Confirmation from CMMI“Downstream Episode Initiators and Participating Practitioners are not precluded from gaining access to theBPCI Advanced Data Portal or receiving beneficiary-identifiable claims data.”Beth Chalick-Kaplan, DNP, CRNP, FNP-BC, RN, CCM Analyst BPCI Advanced Division of Payment Models Patient Care Models Group CMS Innovation Center Centers for Medicare & Medicaid Services Archway Health / info@archwayha.comProprietary and confidential11
Importance of Accessing Your BPCI-A DataOne of the main reasons for participating in BPCI-A is accessing theunprecedented data provided to program participants.Benefits include: Assessing historical group and surgeon performance vs BPCI-A prices Benchmarking performance vs other groups Utilizing data to improve quality and cost performance - overall and by MD Gaining advantages in negotiating VBC contracts with other payers andpurchasers Underwriting risk with stop-loss carriersArchway Health / info@archwayha.comProprietary and confidential12
Trends in Value Based Specialty ietary13
Progress in specialty risk contracting in the Commercial andmarket has been slow A recent study cited 5 live commercial specialty risk arrangements, Several programs have been terminated due to contract complexity & low volumePurchaserConditionsGeisinger Health PlanCoronary Bypass SurgeryPacific Business Groupon Health Total Joint Replacement & SpineExpanding to Cancer and MaternityNotes Integrated provider & plan Most successful employer driven programTravel and COE focusedStill relatively low volumeMultiple large nationalpayersSolid Organ Transplants Longest specialty risk programsEssentially discounted FFSHorizon BCBSMultiple Upside onlyCentral Health PlanOsteoArthritis Episode starts at diagnosisUnitedMultiple Many programs terminated due to low volumeSource: AJMC: Successes and Failures With Bundled Payments in the Commercial Market, October 2, 2020Proprietary and confidential14
Medicare Direct Contracting Program: StructureMedicareContract between CMS and DCE Prospective PMPM payment PMPM based on ParticipantProvider partnerships Annual Full Cap BenchmarkRequiredDirectContractingEntity Full Up/Down Risk Quality Withholds Annual ReconciliationsoptionalSpecialist PartnershipsPrimary CareParticipantProvidersPrimary CareParticipantProvidersPrimary e ProvidersSkeletalCancerCareDiabetesChronicNeuro No effect on alignment Option to be paid by DCE Required Contracts Determine alignment Drives Primary Care cappayments Responsible for quality Paid by DCE Need to get to 5,000 lives to startArchway Health / info@archwayha.comParticipant Providers Determines alignment Drives Specialty Cappayments Paid by DCEPreferred Providers Doesn’t drive alignment Can drive specialty Cappayments Can be paid by DCEProprietary and confidential15
Medicare Direct Contracting - Global Risk ModelGame Changing Attributes1. Prospective Payment ACO Model2. Not a Shared Savings program3. Significant Incentives forSpecialty Risk Arrangements Monthly PMPMs paid to DCE Moves Medicare FFS patients into risk model Most attribution will be Primary Care driven DCE keeps all savings and responsible for alllosses 2% initial discount 25% Up & Down Risk Corridor Specialty PMPMs flow to DCE if they havedownstream specialty partnerships DCE success will require partnerships withhigh performing specialistsArchway Health / info@archwayha.com / (617) 209-7985Proprietary and confidential16
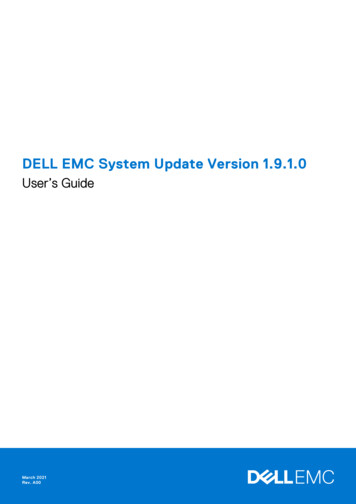
Medicare Direct Contracting Entity - Global Risk ModelBudget by Specialty Area 878 Per Member Per Month 52.7 Million Annual Budget5,000 Medicare BeneficiariesSource: Institute for Health Evaluation & Metrics, University of WashingtonArchway Health / info@archwayha.comProprietary and confidential17
Key features to fulfill program goalsCapitated paymentsBased on performance yearbenchmarks, option between:Benefit EnhancementsEnhancements and waivers canbe provided to beneficiaries, this:Outcomes MetricsDC has a small set of qualitymanageable quality measureTotal Cost of Care CapitationIncreases complianceAll-cause readmissionsPrimary Care CapitationDisburdens providersUnplanned admissionsHelps fulfill goals by:Improving cash flowSupporting reinvestmentCreates flexibility for downstreamVBC arrangementsBenefit enhancements willinclude such mechanisms as:Days at home (High Needs)The quality measures set is:SNF waiverTelehealthOutcomes focusedHome visitsCost-sharingCentered on preventable admitsRewardsPBPM Archway Health / info@archwayha.comProprietary and confidential18
Medicare Direct Contracting - Global Risk ModelKeys to SuccessPrimary Care Ability to transition from FFS to CapitationExpanded PCP panel sizeSpecialty Care Greater use of Care Extenders Patient engagement & TelemedicinePreferred referral partnerships with DCE’sAbility to use data to demonstrate great outcomesat value based pricesAbility to take and manage risk Patient risk segmentationChronic care managementPreferred partnerships with High QualityValue Based SpecialistsRisk financing & Stop-LossArchway Health / info@archwayha.com Pay for PerformanceBundlesCarve-OutsEasy accessCollaborative, high quality hospital and post-acutepartnersIntegrated patient engagement toolsProprietary and confidential19
Key TakeawaysArchway Health / info@archwayha.com / (617) roprietary20
Additional Opportunities in Value Based Specialty Contracting The Commercial market is still moving slowly The Medicare Direct Contracting program is poised to dramatically change the wayspecialty care is delivered and paid for Capitalize on BPCIA data to Assess your performance vs competitors Identify opportunities vs benchmark performers Engage in contract negotiation Prepare to enter risk arrangements Understand local market - what DCEs are in your market? Evaluate Participant / Preferred Provider opportunities in Cohort 2 and beyond Specialists who are prepared to enter into risk based arrangements will win big relativeto competitorsArchway Health / info@archwayha.comProprietary and confidential21
Closing Remarks on BPCIA There are still opportunities for Orthopedic groups and surgeons to participate inthe final three years of the program Surgeons can start in the program at anytime, there are no CMS imposed deadlines Choose your partner wisely Make sure you get can access to your data Fully understand your Pricing, Performance, Opportunities and Risks Maintain control over your billing process Prepare for participation in Direct Contracting & other emerging specialty riskarrangementsArchway Health / info@archwayha.comProprietary and confidential22
Questions & AnswersContact us at info@archwayha.comArchway Health / fidentialProprietary23
Episode Initiators with that Convener no longer able to participate in the program as traditional EIs. Medicare unable to allow EIs to switch conveners or become own convener. All dropped EIs removed from program effective 1/1/21. Only way for non-participating Ortho Surgeons to move forward in MY4