Transcription
m a y / ju n e 2 0 0 9 VO L UM E 1 1 3Table of Contents3Everyday stories . . . profiles of your CAOT colleaguesAlison Sisson and Karen Mills4National Blueprint for Injury Prevention in Older DriversJanet Craik and Claudia von Zweck5Occupation-based program development in primary health careMelissa Howey, Tania Angelucci, Dawn Johnston and Elizabeth Townsend8Private Practice InsightsEvidence based practice in private practice occupational therapy: Perceptions, barriers and solutionsDonna Barrett and Margo Paterson11Theory Meets PracticeAccessibility is the law: A review of environmental assessments to improve accessJessica Malpage, Pei-En Shih and Lisa Klinger14What’s online15Update Report on the CAOT Strategic PlanClaudia von Zweck19Theory Meets PracticeThe Person-Environment-Occupation Circle Tool: A simple way to bridge theory into practiceHeidi Cramm22My journey towards “Steps in the Right Direction: Connecting & Collaborating in EarlyIntervention Therapy with Aboriginal Children & Families in British Columbia”Alison Gerlach24Information web portal for internationally educated occupational therapistsKathy Van Benthem25Professional insurance: What you need to knowBrian Gomes26The Canadian Model of Client-Centred Enablement: Reflections from diverse occupationaltherapy practitionersRobin Stadnyk, Jill Phillips, Slavko Sapeta, Alison MacAulay, Margaret Champion, Linna Tam, andJanet Craik29Update from the COTF30CAOT endorsed coursesISSN: 1481-5532Canada Post agreement #40034418read full colour version @ www.caot.ca1
Statements made in contributions toOccupational Therapy Now (OT Now)are made solely on the responsibilityof the author and unless so stated donot reflect the official position of CAOT,and CAOT assumes no responsibility forsuch statements. OT Now encouragesdialogue on issues affecting occupational therapists and welcomes yourparticipation.Editorial rights reservedAcceptance of advertisements does notimply endorsement by OT Now nor bythe CAOT.CAOT patronHer Excellency the Right HonourableMichaëlle Jean C.C., C.M.M., C.O.M., C.D.Governor General of CanadaCAOT PRESIDENTElizabeth Taylor, PhDCAOT Executive DirectorClaudia von Zweck, PhDRETURN UNDELIVERABLECANADIAN ADDRESSES TO:CAOT – CTTC Building3400 – 1125 Colonel By Drive Ottawa,Ontario KIS 5R1 CANE-mail: publications@caot.caINDEXINGOT Now is indexed by: ProQuest andOTDBase.ADVERTISINGLisa Sheehan (613) 523-2268, ext. 232E-mail: advertising@caot.casubscriptionsLinda Charney (613) 523-2268, ext. 242E-mail: subscriptions@caot.caCOPYRIGHTCopyright of OT Now is held by the CAOT.Permission must be obtained in writingfrom CAOT to photocopy, reproduce orreprint any material published in themagazine unless otherwise noted. Thereis a per page, per table or figure chargefor commercial use. Individual membersof CAOT or ACOTUP have permission tophotocopy up to 100 copies of an articleif such copies are distributed withoutcharge for educational or consumerinformation purposes.Copyright requests may be sent to:Lisa SheehanE-mail: copyright@caot.caOccupational Therapy Now is published 6 timesa year (bimonthly beginning with January) by theCanadian Association of Occupational Therapists (CAOT).managing editorBrenda McGibbon Lammi, MSc, BHSc, OT Reg(Ont),Tel. (613) 587-4124, Fax (613) 587-4121, email: otnow@caot.caTRANSLATIONDe Shakespeare à Molière, Services de traductionDESIGN & LAYOUTJAR CreativeON-LINE KEY WORD EDITORKathleen RaumCAOT Editorial boardChair: Anita UnruhMembers: Emily Etcheverry, Mary Forham, April Furlong, TomGrant, Robin Jewers, & Darla KingEx-officio: Marcia Finlayson & Brenda McGibbon Lammicolumn editorsCritically Appraised PapersLori Letts, PhDInternational ConnectionsSandra Bressler, MAIn Touch with Assistive TechnologyRoselle Adler, BScOT & Josée Séguin, MScOT ThenSue Baptiste, MHScPrivate Practice InsightsJonathan Rivero, BScOT, OT(c)Christel Seeberger, BSc OT, OT Reg (NB), OTRSense of DoingHelene J. Polatajko, PhD & Jane A. Davis, MScTele-occupational TherapyLili Liu, PhD & Masako Miyazaki, PhDTheory Meets PracticeHeidi Cramm, MScWatch Your PracticeSandra Hobson, MAEdA Tribute to Ethel Clark1916 - 2009Ethel Clark, born in Chelmsford, N.B., graduated in occupational therapy from the University of Toronto in 1949. She beganher career as a staff therapist at the Kingston Psychiatric Hospital. She later became the Director of Occupational Therapy, aposition she held until her retirement in 1977. Her special ability to challenge her staff to use all their assets and abilities toorganise workshops, create new treatment approaches, and use evidence based practice was well recognised. Ethel was alsoan active participant in the education of student occupational therapists. She offered fieldwork placements for students andcontributed to the establishment of occupational therapy educational programs in Kingston, initially under the auspices of theCanadian Association of Occupational Therapists (CAOT) and later at Queen’s University.As an active member of CAOT, Ontario Society of Occupational Therapists (OSOT), and the Kingston Branch of OSOT, Ethelheld many committee and leadership responsibilities at all levels including the Board of Directors of CAOT. She was awardedan Honorary Life Membership in OSOT in 1980, this prestigious award recognizes distinguished and long standing contributionto the profession and/or OSOT. Ethel was a passionate professional who contributed enormously to both!Ethel’s many interests included golf, bridge, travelling, reading, quilting and researching her family tree. She was a memberof the RCAF during the Second World War and was the first female in the armed forces to successfully parachute from a planecrash. Thus she became a member of the renowned Caterpillar Club.Ethel passed away on January 4, 2009 in Miramichi, New Brunswick, surrounded by her family. Ethel will be remembered byher many friends, former colleagues, and family.2occupational therapy now volume 11.3
Everyday stories . . .profiles of your CAOT colleaguesAlison Sisson and Karen MillsAlison Sisson and Karen Mills were the co-conveners ofthe CAOT Conference in June, 2008 in Whitehorse, Yukonand became familiar faces to those of us attending theConference. The Yukon Convention Bureau awarded theAssociation of Yukon Occupational Therapists a BravoAward for their role in the 2008 CAOT Conference. TheCAOT Conference was one of the largest conferencesheld in the Yukon last year.Karen MillsFamily life:Married with four children, age 23, 20, 18, 15.Education: Bachelor of Science in Occupational Therapy, University of Western Ontario,1985 Bachelor of Arts, University of Western Ontario, 1985Career path as an occupational therapist: First worked as an occupational therapist at St.Mary’s Hospital in London, Ontario with chronic painclients and amputees. Moved to Vancouver and worked at Holy FamilyHospital in outpatient neurology. Next position was at St. Mary’s Hospital, New Westminster, as the Clinical Supervisor of OccupationalTherapy Services for thirteen years. In 2003, moved my family north to the Yukon andstarted fresh at Whitehorse General Hospital in a100% clinical role covering inpatients and outpatient services. I’ve now added splinting, arthritis,diabetic footcare education, and thermal injuriesto my clinical skills. Moved into the Manager ofTherapy Services position a year after moving to theYukon and continued to carry an outpatient clinicalcaseload. Have recently moved into a non-clinicalrole at the hospital as Director of Special Projects. Member of CAOT and the Association of Yukon Occupational TherapistsHobbies/interests: I enjoy quilting and fabric dying. Am an activemember of a local quilting guild and teach quiltingat Bear’s Paw Quilts. Enjoy kayaking and camping.Karen MillsAlison SissonAlison SissonFamily life:Originally from Haliburton, OntarioSingle, with one lovely, black cat named KawaiiEducation: Honours Bachelor of Science (Biology), Queen’s University, 1994 Bachelor of Science in Occupational Therapy, McGillUniversity, 1999 Masters of Rehabilitation Science, expected graduation in May, 2009, McMaster UniversityCareer path as an occupational therapist: Moved to Toronto in 1999 following graduationfrom McGill and worked for COTA doing communityoccupational therapy with a psychogeriatric andphys-med caseload. Worked at the Toronto Rehabilitation Institute withan outpatient stroke caseload. In January 2003, moved north to Whitehorse to workfor Yukon Continuing Care providing occupationaltherapy to Copper Ridge Place, a long term care facility in Whitehorse, and for the Regional Therapiesprogram, providing home care occupational therapyto communities throughout the Yukon. In 2007, went to India on a Rotary exchange to meetother occupational therapists and observe rehabilitation services throughout central India. Currently working for Yukon Continuing Care asa Policy & Standards Analyst which includes bothpolicy development for the branch and the lead rolefor branch-wide accreditation. Very interested in the effective provision of rehabilitation services to rural and northern communities. Board member of Yukon Learn Society Member of CAOT and Association of YukonOccupational TherapistsHobbies/interests: Love hiking, cross-country skiing, canoeing, traveling, knitting, yogaread full colour version @ www.caot.ca3
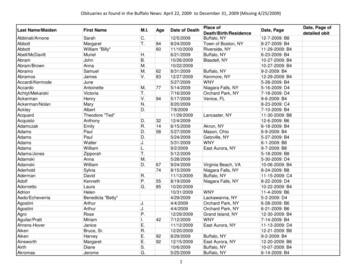
National Blueprint for Injury Preventionin Older DriversJanet Craik, Director of Professional Practice and Claudia von Zweck, Executive Director, CAOTThe Canadian Association of Occupational Therapists(CAOT) has recently collaborated with McGill University,and Dr. Nicol Korner-Bitensky in particular, to developthe National Blueprint for Injury Prevention in OlderDrivers. The Blueprint was successfully launched onFebruary 26th, 2009, in Ottawa, Ontario, gaining national media attention.What is the Older Driver Blueprint?The Older Driver Blueprint is funded by the PublicHealth Agency of Canada. It is an important and innovative initiative that aims to enhance the capacityof older adults to maintain their ability to drive safelyfor as long as possible. The ultimate goal is to maintainolder adults’ engagement in the occupations that givemeaning and purpose to their lives such as social andleisure activities, work and volunteerism. The OlderDriver Blueprint document itself comprises severalmajor topics and includes a vision, guiding principles,priority goals, and directions for action.Why is the Older Driver Blueprint important?Older adults are the fastest growing segment of thedriving population. While it has long been believedthat the older driver is actually the safest and mostcautious driver on the road, statistical analysis revealsotherwise. The leading cause of accidental deaths forpersons 65 to 75 years old in Canada today is drivingrelated accidents with those over the age of 75 having a3.5 times higher crash rate per miles driven comparedto 35 to 44 year olds. Given that there will be almostdouble the number of older drivers in Canada by 2040,this issue is likely to increase in the coming years ifstrategic actions are not put in place.How was the Older Driver Blueprintdeveloped?A National Advisory Committee of individuals representing stakeholders in older driver safety cametogether to create the Blueprint. Stakeholders includeolder adults in Canada and those concerned with olderdriver safety such as national and local seniors agencies, health care professionals, insurance and automobile industries, traffic safety professionals, law enforcement representatives, provincial, territorial and federal4occupational therapy now volume 11.3health agencies and ministries. The intent is that theOlder Driver Blueprint will be used by many stakeholders and will inform future policy, practice, educationand research regarding older driver safety.Occupational therapy’s role in injury prevention in older driversOccupational therapists have education and training to evaluate physical, cognitive, visual-perceptual,and behavioral aspects of driving using standardizedpre-road and on-road assessments. These assessmentshelp to alert the driver to areas that require driving refresher or retraining. Occupational therapists can alsoprovide recommendations on vehicle modification andadaptive equipment to enable safer driving practices.For more information about the Blueprint visitwww.caot.ca/driving and www.mcgill.ca/spot/ot/drivingThe CAOT has recently updated their Position Statement: Occupational Therapy and Driver Rehabilitation.Visit www.caot.ca for the full document.Launch of the National Blueprint for Injury Prevention inOlder Drivers. (L) to (R) spokespeople: Patricia Clark, NationalExecutive Director, Active Living Coalition for Older Adults; Dr.Nicol Korner-Bitensky, Ph.D., OT(C), erg., Principal Investigator for the Blueprint, McGill University; Dr. Colin Carrie, B.Sc.(Hons.), D.C., M.P., Parliamentary Secretary and representingthe Minister of Health - The Honourable Leona Aglukkaq, P.C.,M.P.; Dr. Claudia von Zweck, Ph.D., OT Reg. (Ont.), OT(C) Executive Director, CAOT; Dr. Elizabeth Taylor, Ph.D., President, CAOT.
Occupation-based program development inprimary health careMelissa Howey, Tania Angelucci, Dawn Johnston and Elizabeth TownsendInclusion of occupation-based programs in primaryhealth care increases the availability of services thatcontribute to comprehensive, quality primary healthcare and to occupational community development(Lauckner, Pentland, & Patterson, 2008). In this articlewe illustrate how a theoretical understanding of occupation and enablement may be applied to developprimary health care occupational therapy.Occupation-based primary health carePrimary health care places attention on health promotion, disease prevention, and identifies needs toincrease access to services for all individuals (HealthCanada, 2006). The goal of primary heath care is toprovide preventative services as opposed to reactiveservices that focus on the diagnosis and treatment ofillness and injury. Primary health care encompassesservices beyond traditional health care to includeeducation, income, housing, and environment (HealthCanada, 2006).Client-centred, occupation-based health care hasbeen the implicit if not explicit theoretical foundation for remedial occupational therapy for many years(Townsend & Polatajko, 2007). Occupational therapistshave a role in primary health care by focusing on theoccupational needs of populations, and on enabling occupational performance and engagement as a meansof preventing injury and promoting health (CAOT,2003). This involves responding to the occupationalneeds of clients. Practitioners use a combination ofenablement skills in adapting communities and programs, and advocating for health promotion programsthat emphasize occupational engagement (Townsend& Polatajko, 2007). The aim is to provide more population health, illness prevention, chronic disease management, and health promotion by all professions (Heuchemer & Josephsson, 2006). It is within the primaryhealth care context that occupational therapists haveincreasingly had the opportunity to develop and delivercommunity-based services at a primary level of care.Community-based and primary health careoccupational therapyBoth community-based and primary health care occupational therapists work with clients in their envi-ronment with a focus on clientAbout the authors –centred occupations (Wittman &Melissa Howey, MSc(OT),is an occupational theraVelde, 2001).pist at the VancouverThe difference between theGeneral Hospitaltwo approaches is the focus onVancouver, British Codisability and illness prevention inlumbia.primary health care and the remeTania Angelucci, MSc(OT),diation or rehabilitation of existis an occupationaling disability or illness throughtherapist in the Living Skycommunity-based occupationalSchool Division in NorthBattleford, Saskatchewan.therapy. In the past twenty yearsthere has been a shift from institu- Dawn Johnston, MSc(OT),is an occupational theration-based, remedial occupationalpist for Harbourstonetherapy to community-basedEnhanced Care Sydney inremedial occupational therapy.Cape Breton, Nova Scotia.Now the shift is extendingElizabeth Townsend, PhD.,occupational therapy into primaryOT (C), Reg. NS, is a Profeshealth care within the community,sor and the Director ofredefining health as physical,the School of Occupationmental, and social well-beingal Therapy at DalhousieUniversity in Halifax, Novarather than simply the absence ofScotia.disease (Perrin & Wittman, 2001).Community-based occupationaltherapy aims to remediate the impact of everyday lifechanges in a client’s community, including changeswithin the multiple systems of clients: psychological,emotional, physical and social, by using occupationsthat clients define as meaningful (Ward et al., 2007).Primary health care occupational therapy aims to enable clients to live and interact within their community,preventing disability and illness (Ward et al., 2007).Primary health care’s focus on building healthy andsupportive communities goes beyond individualized disability and illness prevention to improve the physical, social,and institutional environment (Baum, 1998). Improving theenvironment for occupational engagement assists in creating healthy surroundings that contribute to future health,well-being and justice (Townsend & Polatajko, 2007).The lack of a healthy environment has a negative impacton physical and mental health (Wilcock, 2005). With anincreasing shift to primary health care and increasing attention on prevention and (inter)dependence, there is anincreased need and opportunity for occupational therapyservices to enrich the services available through primaryhealth care (Baum, 1998).read full colour version @ www.caot.ca5
Occupation-based primary health care:An exampleIn collaboration with a community primary health carecentre, occupational therapy students generated a business proposal aimed at enhancing primary health careservices for community members. The program goal wasto enable target populations within the community toincrease their occupational engagement and communityparticipation in the areas of: Safety and independence Re-engagement into the community and daily occupations Capturing their potential Social inclusionBased on a community needs assessment conductedby talking with the staff of the community health centreand members of target populations, options for specificoccupation-based programs were discussed. Two clientsituations are presented in which the primary health careneeds were for transportation, communication, community support and safety. These examples of occupationbased primary health care implemented by one of theauthors are presented here; the aim in both situations wasto increase participation through facilitating occupationalre-engagement.Situation #1Joe- worked with the occupational therapy studentwho was initially asked to see what could be done toenhance his writing skills. Additionally Joe expressedconcern about going out in the community with hiswheelchair because he was concerned about goingover curbs and downhill; he would go outside moreoften if he had greater confidence in his abilities. Areferral was sent to the local Wheelchair Skills Training Program, two dates for Joe to participate werereceived. Due to inaccessible and unreliable transportation Joe cancelled his appointment.In Situation #1, the aim was to facilitate Joe’s occupational engagement within his environment.Due to gaps in existing services regarding transportation, enablement to acquire wheelchair skills washindered. Joe, according to the Canadian Model ofClient-Centered Enablement (CMCE), experienced whathas been called “missed enablement” (Townsend &Polatajko, 2007). Joe was unable to engage in educationin terms of wheelchair safety due to a lack of coordination of services that hindered his overall engagement(Townsend & Poatajko, 2007).6occupational therapy now volume 11.3Situation #2Linda- worked with the occupational therapystudent on enhancing Linda’s exercise routine andsetting daily goals. Linda was provided with routineplanning agenda sheets to write down daily goalsthe night before; when waking up in the morningthere was a concrete list of things to accomplish. Theoccupational therapy student accompanied Linda toYMCA on a day pass to try exercise equipment andsee what Linda could do; Linda enjoyed the gym andis now thinking about joining a community networkthat offers a YMCA membership for individuals livingin the community with mental stresses.Situation #2 is a second example of an occupationbased program implemented to assist in Linda’s senseof accomplishment and to facilitate change for thefuture. The approach began by capitalizing on Linda’sstrengths to ensure successful completion of goals(Schultz-Krohn, Drnek, & Powell, 2006). Linda seemedto accomplish her objectives by setting goals that wereimportant to her. The sense of accomplishment wastaken forward to facilitate community engagementboth within the mental health community and thecommunity at large. By collaborating with Linda, coaching her to achieve her goals, working to coordinateservices between the health care centre, mental healthcommunity resources and local community services,Linda and others in the population living with a chronic mental health disorder would more likely experience“effective enablement” (Townsend& Polatajko, 2007).ReflectionsThese two situations highlight the opportunities foroccupation-based program development in primaryhealth care. In Joe’s situation there is a continued needto promote primary health care and a coordination ofservices. Although services began with community-
based rehabilitation, a primary health care approachevolved by gathering resource information and advocating with members of the community to improve accessible transportation. The primary health care aspect“Occupational therapists have a role in primary health careby focusing on the occupational needs of populations, andon enabling occupational performance and engagementas a means of preventing injury and promoting health(CAOT, 2006). “was the shift to a population approach with a focus onprevention of community dis-engagement by thoseusing mobility devices that are not easily transportedin regular buses or taxis, particularly for those on lowincomes. In Linda’s situation, a psychosocial rehabilitation occupational therapy approach was extended intoprimary health care occupational therapy. Occupational therapy took a population perspective on accessto community resources, and began to improve serviceaccess for prevention and community development.The project took the initiatives on primary healthcare from both the CAOT and Health Canada from theory to practice. Occupational therapy in primary healthcare can facilitate occupational engagement throughthe use of occupation-based programs. By using theenablement skills of an occupational therapist, focusing on the strengths of clients and the communities inwhich they live, and taking a population and prevention approach, occupational therapists are poised toadvance health, well being and justice through occupation.The marginalization of communities affects thehealth of community members and the availabilityof services. The impact of this project has been thesuccessful development of a collaborative relationship between the community health centre and anoccupational therapy education program at DalhousieUniversity in Halifax, Nova Scotia. The collaboration hascontinued and a budget request for full time primaryhealth care occupational therapy services is pending.The application of theory to practice, as seen in Joe andLinda’s situations, helped to build the business pro-posal by highlighting the need for a preventive, population-based approach for underserviced clients.In the next phase of program development, stakeholders will be interviewed to further understand theiroccupational needs and the potential for occupationbased programming to enrich an existing primaryhealth care service.References:Baum, C. (1998). Client-centred practice in a changing healthcare system. In M. Law (Ed.), Client-centered occupationaltherapy (pp. 29- 45). Thorofare, NJ: SLACK Inc.Canadian Association of Occupational Therapists (2003).Position statement on primary health care. RetrievedOctober 10, 2007, from http://www.caot.ca/index.cfm?ChangeID 2&pageID 188Health Canada (2006). About primary health care. RetrievedJune17, 2008 from eng.phpHeuchemer, B., & Josephsson, S. (2006). Leaving homelessnessand addiction: Narratives of an occupational transition.Scandinavian Journal of Occupational Therapy, 13(3), 160-169.Lauckner, H., Pentland, W., & Patterson, M. (2008). ExploringCanadian occupational therapists’ understanding of andexperiences in community development. Canadian Journalof Occupational Therapy, 74(4), 314-325.Perrin, K. & Wittman, P. P. (2001). Educating for community-basedoccupational therapy practice: a demonstration project. Occupational Therapy in Health Care, 13, 11-21.Schultz-Krohn, W., Drnek, S., Powell, K. (2006). Occupationaltherapy intervention to foster goal setting skills for homeless mothers. Occupational Therapy in Health Care, 20(3-4),149-166.Townsend, E. A. & Polatajko H. J. (2007). Enabling occupationII: Advancing an occupational therapy vision for health,well-being, & justice through occupation. Ottawa, ON: CAOTPublications ACE.Ward, K., Mitchell, J., & Price, P. (2007). Occupation-based practiceand its relationship to social and occupational participationin adults with spinal cord injury. OTJR; Occupation, Participation & Health, 27(4), 149-156.Wilcock, A. A. (2005). Occupational science: Bridging occupationand health. Canadian Journal of Occupational Therapy, 72(1),5-12.Wittman, P. P., & Velde, B. P. (2001). Occupational therapy in thecommunity: What, why and how. Occupational Therapy inHealth care, 13(3/4), 1-5.read full colour version @ www.caot.ca7
Private Practice InsightsColumn Editor: Christel Seeberger and Jon RiveroEvidence based practice in privatepractice occupational therapy:Perceptions, barriers and solutionsDonna Barrett and Margo PatersonEvidence based practice (EBP) requires therapists toaccess, appraise and integrate research literaturewith clinical expertise and clients’ values (Bennett &Townsend, 2003). Although research indicates thattherapists support the principles and importance ofEBP (McClusky 2004), challenges such as time, appraisal skills, workloads, and a perception that there is a lackof evidence to support occupational therapy intervention have resulted in therapists using experience andinformation gleaned from practice related courses toinform their clinical decision making (McCluskey, 2003).The findings of a qualitative study using a focusgroup with five private practice occupational therapists are presented here. The aim of the study wasto understand the unique experiences, perceptions,barriers, and feasible solutions to implementing EBPin private sector occupational therapy.PerceptionsOne participant identified the analogy of EBP as afilter which clinicians can put their clinical experience, knowledge, and client perceptions throughbefore making treatment plans and solving clinicalproblems:“It [EBP] is the filter. My intuition is the foundationand I’m going to put the research through that sortof filter and if it still hangs tight at the end, then Iam going to make that choice. even if the evidencesays this is the sort of treatment for this person withcognitive issues if there are other diagnoses and family issues that is the primary filter that’s what Ineed to add more purposefully to the tree of decisionmaking that happens in my brain when I’m choosingan intervention.”.“It’s probably a combination of that pool of clinicalexperience and what you read and know and learnthrough the research in terms of the interventionsyou choose. Pull all those pieces together and helpit direct your way of thinking. To me, even thoughyou do your research and are reading the articles,you’re still reviewing and critically appraising them.The bottom line still comes down to clinical experience and expertise and that filter.”8occupational therapy now volume 11.3BarriersParticipants were asked to reflect on the barriers toadopting EBP that are unique to the private sector.Common themes that emerged included isolation,heightened accountability, administrative demands,time and money. Working in the community and inprivate practice presents an inherent isolation whichone participant described as: “we’re all islands.”Participants indicated that although, as sole practitioners, efforts are made to meet and connect with otherpractitioners, taking that initiative to make it happenat a frequency that allows for discussion about spe“Participants discussed how the very nature of privatepractice work demands a higher level of accountability andyet is designed in such a way that EBP strategies are viewedas hurdles “cific EBP issues is challenging. It was acknowledgedthat when working in a group setting (i.e. hospital,clinic etc.) information gets shared spontaneouslyand motivates the practitioner to inquire more deeplyabout EBP issues.Participants discussed how the very nature ofprivate practice work demands a higher level of accountability and yet is designed in such a way thatEBP strategies are viewed as hurdles because of otherdemands placed on them. They reflected that lackof time to adopt EBP may be more of a factor whenoperating in a fee for service type of environment.Practitioners perceive that a large amount of timeis required to research evidence and appraise theliterature. Frustration with their skill level in efficiently finding applicable information was also noted,as were financial implications of completing tasksthat are not part of the
Masters of Rehabilitation Science, expected gradua-tion in May, 2009, McMaster University Career path as an occupational therapist: Moved to Toronto in 1999 following graduation from McGill and worked for COTA doing community occupational therapy with a psychogeriatric and phys-med caseload.