Transcription
R EVIEWControversies in vitamin D: deficiency andsupplementation after Roux-en-Y gastricbypass surgeryKerstyn C Zalesin†,Wendy M Miller,Katherine E Nori Janosz,Jose Yanez,Kevin Krause,David L Chengelis &Peter A McCulloughCurrent vitamin D recommendations are insufficient and a higher intake is necessary in thegeneral population. The requirements of bariatric surgery patients can be augmented bylongstanding obesity coupled with, gastro–intestinal malabsorption. Vitamin D deficiencypromotes metabolic bone disease and may increase risks for a multitude of other medicalconditions. This article reviews some controversies surrounding vitamin D and proposes amanagement strategy for bariatric surgery patients.†Authorfor correspondenceWilliam Beaumont Hospital,Division of Nutrition andPreventive Medicine,4949 CoolidgeHighwayRoyal Oak,Michigan 48073, USATel.: 1 248 655 5900Fax: 1 248 655 5901kzalesin@beaumont.eduKeywords: bariatric surgery,cholecalciferol, metabolicbone disease, obesity,vitamin Dpart ofVitamin D deficiency is a worldwide concernthat is becoming increasingly recognized as apublic health threat. Certain populations are atgreater risk for vitamin D deficiency includingthe obese and those with gastro–intestinal malabsorption, which exemplifies bariatric surgerypatients. Bariatric surgery is the most potent toolavailable in the treatment of obesity and itsinherent comorbidities and is becoming increasingly accepted by physicians and patients alike.Roux-en-Y gastric bypass (RYGB) is the goldstandard in the surgical treatment of obesity, succeeding by utilizing restrictive and malabsorptivesurgical techniques, which may promotevitamin D deficiencies [1]. The impact ofvitamin D deficiency is great; although earlystages may be asymptomatic, progression tometabolic bone disease (MBD) can occur withtime [2]. Ironically, middle-aged women, whocomprise a large proportion of bariatric surgerypatients and who benefit greatly from surgicalweight loss, are at the greatest risk from theconsequences of bone loss [3]. There is developingconsensus that current vitamin D recommendations are insufficient and a higher intake ofvitamin D is necessary in the general population,yet the requirements of vitamin D after bariatricsurgery remains elusive. This article reviewsvitamin D controversies and proposes amanagement strategy for bariatric surgery patients.Vitamin D sourceVitamin D is synthesized in the epidermis from7-dehydrocholesterol and catalyzed by ultraviolet-B(UVB)radiation(wavelengths290–315 nm) from sunlight. It is subsequentlyhydroxylated by the liver and then the kidney tobecome 1α, 25-dihydroxyvitamin D3, which isthe active form of vitamin D. Adequate sunlightexposure is capable of providing ample supply of10.2217/14750708.4.5.561 2007 Future Medicine Ltd ISSN 1475-0708vitamin D. It is estimated that 10–15 minutes ofsunlight will produce the equivalent of 3000 IUof vitamin D3. [4]. However, with the increasingutilization of sunscreens and a decrease in outdoor activities, reliance on natural light is aninadequate source of vitamin D for much oftoday’s population [5]. In addition, betweenNovember and February, natural sunlight exposure in the northern latitudes (greater than 35thparallel) is unable to produce adequate levels ofvitamin D [5]. Food sources, including fortifiedmilk, margarines, certain cereals and orangejuice, as well as fatty fish and egg yolks, are likewise insufficient sources of vitamin D, as most ofthe population does not consistently consumelarge enough quantities to suffice [6].Ergocalciferol (vitamin D2) versuscholecalciferol (vitamin D3)There are two forms of commercially availablevitamin D: ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3). Initially these formulationswere thought to be equivalent; however, recentstudies identify cholecalciferol as more effective inraising serum levels of 25-hydroxyvitamin D [7].Cholecalciferol’s potency to improve serum25-hydroxyvitamin is estimated to be threefold,but could be as high as tenfold [7]. Differingpotencies result from a greater molecular stabilityof cholecalciferol compared with ergocalciferol, aswell as a more biologically active receptor bindingwith choelcalciferol [8]. Many commercially available vitamins are reformulating their products toincorporate cholecalciferol as the predominantsource of vitamin D, but this has not beenuniversally embraced. Prescription vitamin D utilized by clinicians for severe hypovitaminosis Dtreatment are predominantly formulated withergocalciferol, as there is limited availability ofhigher-dose cholecalciferol.Therapy (2007) 4(5), 561–574561
REVIEW – Zalesin, Miller, Nori Janosz et al.Vitamin D & obesityThe relationship between adiposity andvitamin D deficiency was first recognized over30 years ago [9]. In recent years, a number ofstudies continue to validate this relationship.Arunabh and colleagues found an inverseassociation between percentage body fat andserum 25-hydroxyvitamin D levels in 410 healthywomen [10]. Similarly, Yanoff and colleaguesfound that the prevalence of hypovitaminosis Dincreased in parallel with BMI for both black andwhite subjects in a group of 379 otherwise healthyadults [11]. The majority (60%) of 279 morbidlyobese adults seeking gastric bypass surgery werefound to have a serum 25-hydroxyvitamin D levelof 20 ng/ml or less [12], providing further tamin D and BMI.Various theories regarding the etiology ofvitamin D deficiency in obesity have been postulated. These include avoidance of sun exposure in obese individuals [13], enhancedproduction of 1,25-hydroxyvitamin D with aresultant negative feedback on hepatic synthesisof 25-hydroxyvitamin D [14], as well asincreased uptake of circulating vitamin D intoadipose tissue [15]. As vitamin D is fat-soluble,it is reasonable to speculate that obese individuals have decreased bioavailability of vitamin Ddue to sequestering in adipose tissue.To assess some of the theories regardingvitamin D deficiency in obesity, Wortsman andcolleagues compared the effect of whole-bodyultraviolet radiation and a pharmacologic doseof 1,25-hydroxyvitamin D in 19 healthy, normal weight subjects versus 19 healthy, obesesubjects [16]. Following whole-body irradiation,the content of the vitamin D3 precursor7-dehydrocholesterol in the skin of obese andnonobese subjects did not differ significantly,nor did its conversion to previtamin D3 afterirradiation in vitro. After 24 h, however, theincremental increase of vitamin D3 was 57%lower in obese subjects as compared withnonobese subjects. Therefore, an inverserelationship between BMI and serumvitamin D3 levels following irradiation wasidentified. Similarly, there was an inversecorrelation between BMI and serum1,25-hydroxyvitamin D following a 50,000 IUoral dose of 1,25-hydroxyvitamin D. Theauthors concluded that obesity-associatedhypovitaminosis D is likely due to its deposition in body fat, which leads to decreasedbioavailability of vitamin D.562Therapy (2007) 4(5)Vitamin D & its association with othermedical conditionsVitamin D is proving to be important in the prevention of many chronic disease states, includingsome cancers, autoimmune disorders, andcardiovascular disease. Multiple studies of persons living at higher latitudes, with less naturalexposure to UVB solar radiation, demonstrate anincreased risk for some cancers, multiple sclerosisand hypertension [17–25]. It has been proposedthat sun exposure augments levels of1,25-dihydroxyvitamin D3, which regulates cellgrowth and inhibits cancer cell proliferation inan autocrine and paracrine fashion [26], or possibly by reducing angiogenesis, increasing cell differentiation and apoptosis of cancer cells andreducing metastases [27,28]. Vitamin D behaves asa hormone rather than a vitamin, by exertingimmunomodulating properties on many cellsreceptors and tissues, including islet cells, heartmuscle, skeletal muscle, active T and B lymphocytes, breast, colon and prostate. In multiplesclerosis, higher vitamin D intake has been associated with disease stabilization and a reducedrisk of developing disease [29,30]. In Type I diabetes, 1,25-dihydroxyvitamin D3 has been shownto reduce risk of disease through the down regulation of cytokines and lymphocyte proliferation,thus reducing overall β-cell destruction [31]. AFinnish study involving 10,366 children demonstrated that a higher intake of vitamin D(2000 IU/day) in the first year of life reduceddevelopment of Type I diabetes by a rate ratio of0.22 (range: 0.05–0.89) [32]. Several epidemiologic and animal studies show vitamin D intakeis inversely associated with autoimmune diseasessuch as rheumatoid arthritis, inflammatorybowel disease, and systemic lupus erythematosus(SLE). An 11-year study of 30,000 women, foundlower daily intake of vitamin D ( 200 IU/day)was associated with a 33% increase in thedevelopment of rheumatoid arthritis [33].Hypertension rates are higher in both the USand Europe for people living at higherlatitudes [8]. Krause et al. found that exposingpatients to UVB radiation for 3 months had amore than 180% increase in 25-hydroxyvitamin D levels, which resulted in a 6 mmHgdecrease in diastolic and systolic blood pressures, similar to the effects of a single bloodpressure medication [34]. The mechanism bywhich vitamin D alters blood pressure is notcompletely understood. However, a study by Liet al., observed mice with higher 1,25-dihydroxyvitamin D3 that effectively downregulated reninfuture science group
Vitamin D deficiency after gastric bypass surgery – REVIEWand angiotensin, which decreases blood pressure, therefore reducing long-term cardiovascular risk [35]. Several observational studiesreport that young adults with vitamin D deficiency are at greater risk of congestive heart failure compared with young adults with adequatevitamin D stores [36,37]. Similarly, two studiesinvolving postmenopausal women found thathigher 25-hydroxyvitamin D levels were associated with decreased myocardial infarctions andischemic heart disease [38].Metabolic bone disease &vascular calcificationLiberation of calcium, phosphorous and othersubstrates from bone may lead to accelerated vascular calcification. Multiple studies indicate thatcalcification occurs at the necrotic core ofatherosclerotic lesions that span the subintimalto vascular medial layers of the arterialwall [39,40]. Vascular calcification thus impliesanatomic presence of atherosclerosis. Greaterdegrees of vascular calcification suggest a greateroverall burden of atherosclerosis in the vasculartree. Several studies have linked osteoporosis andMBD associated with chronic kidney disease toaccelerated vascular calcification [41]. While thereare no data linking calcium, phosphorus,vitamin D and parathyroid hormone (PTH) tochanges in atherosclerosis in bariatric patients,this could be a long-term concern. It may represent somewhat of a paradox, since many of themetabolic changes that occur after bariatric surgery are thought to be favorable to atherosclerosis stabilization and regression, while thedevelopment of bone disease in bariatric patientscould theoretically worsen vascular atherosclerosis and vascular calcification over the longerterm. Clearly, studies of vascular calcification areneeded in this group of patients.Vitamin D deficiency: a link tometabolic bone diseaseThe relationship between vitamin D deficiencyand bone disease is well described. In a study ofcommunity-dwelling patients with hip fractures,half had concomitant vitamin D deficiencywhile a third had secondary hyperparathyroidism [42]. Vitamin D supplementation slowsbone loss in postmenopausal women [43], and hasbeen found to protect against weakness and fallrisk [44], and reduce secondary hyperparathyroidism [45] in the same population. Calciumabsorption and homeostasis is facilitated througha vitamin D mechanism. With a vitamin Dfuture science groupwww.futuremedicine.comdeficiency, gastro–intestinal calcium absorptionis hindered. As a compensatory response to lowercalcium, PTH production stimulates kidneytubule reabsorption, which maintains serum calcium concentrations. The action of PTH stimulates 1,25-dihydroxyvitamin D levels, which inthe early stages, while the process is asymptomatic, leads to an alteration of bony architecturedepleting calcium stores resulting in poor mineralization of bone content, hence promoting boneloss and fracture risks. With advanced deficiency,diffuse arthralgias, myalgias and muscular weakness can mimic various rheumatologic or orthopedic conditions, thus confounding thediagnosis [46]. By definition, MBD encompassesthe spectrum of secondary hyperparathyroidism, osteomalacia and osteoporosis. Thegold standard of differentiating these conditionsis with an iliac crest bone biopsy with doubletetracycline labeling, yet this technique is notclinically utilized in most cases. Bone-specificmarkers can be used as a tool to clinically aid indiscriminating osteomalacia from osteoporosis.Serum predictors of these processes include: alow 25-hydroxyvityamin D, which is the bestassessment of body storages of vitamin D, elevated 1,25-dihydroxyvitamin D and PTH, andbone-specific alkaline phosphatase and osteocalcin, which are markers of osteoblastic boneformation. Urinary N-telepeptides (u-NTX),indicate bone resorption facilitated throughosteoclastic function, as well as inhibited urinarycalcium excretion less than 100mg/day. Antiresorptive treatments used in osteoporosis do notbenefit osteomalacia, which may be partiallyreversible with supplemental vitamin D, makingthis distinction of great importance. To maximizeintestinal calcium and downregulate PTH secretion, serum 25-hydroxyvitamin D levels shouldbe maintained within an optimal normal range.RecommendationsThe Food and Nutrition Board (FNB) of theInstitute of Medicine currently recommendsdaily intake levels of 200 IU from birth to age50 years, 400 IU from the ages of 51–70 years,600 IU for ages over 70 years, and 800 IU forinstitutionalized or homebound individuals [47].These recommendations arose from earlyresearch emphasizing prevention of rickets andare now recognized as insufficient [48]. Higherconcentrations of vitamin D are necessary toprevent bone loss, fractures and other potentially serious medical conditions. Studies indicate that the minimum daily intake for the adult563
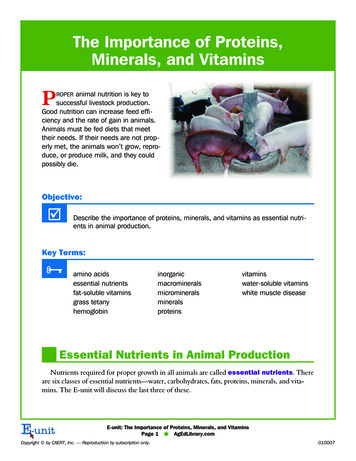
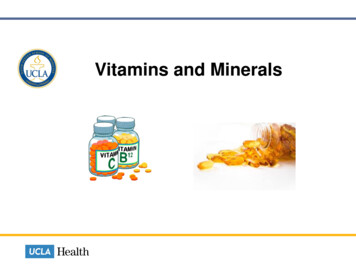
REVIEW – Zalesin, Miller, Nori Janosz et al.population should be closer to 1000 IU daily [49],while the upper limit (UL), which is currentlyacknowledged at 2000 IU/day, may actually be ashigh as 10,000 IU/day [50].Optimal dosing of vitamin D has been foundto be a key factor in differentiating fracture riskreduction. In a placebo-controlled study, using400 IU of cholecalciferol daily was not observedto reduce fracture risk [51]. However, a recentmeta-analysis utilizing 700–800 IU/daily ofcholecalciferol demonstrated a reduced risk forhip fractures of 26% and risk of nonvertebralfracture by 23% compared with placebo. Theauthors concluded that fracture risk reductioncorrelates with optimal serum 25-hydroxyvitamin D and requires dosing at levels greaterthan currently recommended [52]. Evolvingrecommendations in the general populationidentify 25-hydroxyvitamin D at 32 ng/ml orgreater as an optimal range capable of maximallysuppressing PTH levels, thus, limiting boneloss [53]. This concentration is higher than theestablished norm on most laboratories referenceranges, which guides current treatment.Bariatric surgery & vitamin DMBD is a known consequence of prolongedvitamin D deficiency in other malabsorptiveconditions [54], and is well documented after gastrectomy procedures [55]. However, many physicians are unaware of this potential complicationand, thus, do not adequately screen or promptlydiagnose MBD with RYGB surgery [56]. Theduodenum and jejunum are sites of calciumabsorption, which is processed through avitamin D-related transport mechanism. AfterRYBG, the remaining distal small bowel compensates and absorbs calcium, albeit less efficiently. Calcium carbonate is inefficientlyabsorbed owing to the lack of stomach acidity,therefore calcium citrate is the preferred form ofcalcium supplementation after RYGB, yet thisform of calcium is less desirable owing to itsbulky composition. Risks of vitamin D deficiency become amplified by poor intake ofvitamin D and calcium-rich foods in thepostoperative setting, owing to the commondevelopment of lactose intolerance and dietarypreference after surgery [57]. In addition, malabsorption of fat-soluble vitamins may occurowing to ineffective mixing of bile salts with fat,exacerbating the deficiency [58]. As a result ofthese physiologic changes, this population willrequire a greater daily intake of vitamin D tomaintain serum levels and will continue to564Therapy (2007) 4(5)exhibit lifetime risks for these problems. Wereviewed the literature for studies of vitamin Ddeficiency and secondary MBD outcomes afterbariatric surgery.Review of the RYGB literatureThere is great variation in the literature withrespect to the relationship of vitamin D andMBD after RYGB surgery (Table 1). Coates andcolleagues evaluated 25 postoperative RYGBpatients and compared bone turnover markerswith 30 obese controls [59]. Patients in the control group had a greater BMI than those in thepostoperative group measured at 48 7 and32 5 kg/m2, respectively. A significantincrease of u-NTX measured at 93 38 versus24 11 nM/mmolCr, (p 0.001), as well as ahigher osteocalcin, measured at 11.6 3.4 versus 7.6 3.6 ng/ml (p 0.001), among surgery compared with control cases. A subgroupanalysis evaluated 15 patients (12 women andthree men) prospectively for 9 months fromsurgery and likewise noted an increase inu-NTX scores with time, 174 168% at3 months (p 0.01) and 319 187% at9 months (p 0.01). All postoperative patientswere instructed to take a vitamin supplementwith calcium (1200 mg daily) and vitamin D400–800 IU daily. The subgroup lost37 9 kg and had a 29 8% decrease in BMI(p 0.001). Bone mineral density (BMD)scores among this group were significantlydecreased at the hip (7.8 4.8%; p 0.001),trocanter (9.3 5.7%; p 0.001) and totalbody (1.6 2.0%; p 0.05) after surgery.Other markers of bone metabolism, such asPTH serum calcium and 24-h urinary calcium,were unchanged between control and postoperative groups. 25-hydroxyvitamin D levelswere low in both groups, yet unchanged withsurgery. These results indicate that bone turnover may be noted as early as 3 months afterRYGB surgery, with the hip being the mostaffected site, and suggests that vitamin D is notthe only mediator of increase bone turnoverafter bariatric surgery. The authors recommendsupplementation of calcium and vitamin D aswell as screening for MBD in this population.Youssef et al. recently published the effects ofRYGB on calcium, alkaline phosphatase, PTH,and 25-hydroxyvitamin D [60]. The studyenrolled 193 female patients and prospectivelyfollowed them for 2 years. Daily calcium citrate1200 mg with vitamin D 400 IU were recommended daily for all subjects. They noted 53.3%future science group
future science groupwww.futuremedicine.comProspective41 LL-GBP202 SLGBP3.1 3.6 years26 RYGB7 CNT5.7 2.5 years10 years232 RYGB15 RYGB25 RYGB30 CNTn1200 mg Ca2 800 IU vitamin DMVI & Ca2 vitamin D1200 mg Ca2 800 IU vitamin D1200 mg Ca2 400–800 IUvitamin DSupplementuse Vitamin D, PTH in theLL-GBP comparedwith SL-GBPN/A FN‡ LS Ca2 , 25(OH)D Alk Phos* TH, trocanter,total body* uNTX*BMD at TH andLS at 1 year*,similar at year 2N/A uNTX, OC*Similar 25(OH)DSimilar 25(OH)D,PTH Ca2 Outcomes:BMDOutcomes:25(OH)D/bonemarkersKeep 25-OH vitamin D 30 ng/mlAggressively screen & treatdeficient vitamin DFurther studies to defineextent and prevalence ofproblemMBD annual screeningSupplement Ca2 &vitamin D;reasonable to screen BMD inat-risk patientsStudy recommendationsNo baseline dataWt loss betweenstudy and CNT groupsdifferent;small nPoor follow-up, RYGBBPD analyzedtogetherSmall n, shortdurationSmall nStudy weakness[63][64][61][59][59]Ref.*Statistical significance; ‡Not statistically significant.Alk phos: Alkaline phosphatase; BMC: Bone mineral content; BMD: Bone mineral density; BPD: Biliopancreatic diversion; CNT: Control; def: Deficiency; FN: Femoral neck; LL-GBP: Long limb gastric bypass;LS: Lumbar spine; MBD: Metabolic bone disease; MVA: Multivitamin; n: Sample size; N/A: Not available; OC: Osteocalcin; PTH: Parathyroid hormone; RYGB: Roux–en-Y gastric bypass; SL-GBP: Short limbgastric bypass; TH: Total hip; uNTX: Urinary N- telopeptide; Wt: Weight.Johnsonet al.RetrospectivecontrolOtt et al.3 yearsProspectiveProspective,casecontrolled9 monthsRetrospectivecontrolCoateset al.Johnsonet al.2 yearsDesignStudyDurationTable 1. Studies assessing vitamin D and markers for metabolic bone disease with Roux-en-Y gastric bypass surgery.Vitamin D deficiency after gastric bypass surgery – REVIEW565
566Therapy (2007) 4(5)ProspectiveobservationalProspectivecontrolCase zet al.Ybarraet al.de Priscoet al.10–12 years3 years3 years2 years3 RYGB1BPD64 RYGB,80 obeseCNT64 RYGB193femaleRYGB13 RYGBwith BMD13 CNT44 RYGB65 CNTnVariedNo routinesupplementsNo routinesupplements1200 mg Ca2 400 IU vitamin D1200 mg Ca2 8 µg vitamin DNot definedSupplementuseN/AN/A 25(OH)D Alk phos, PTHafter RYGB* PTH, 1,25vitamin D, alkphos Ca2 , 25vitamin DN/A PTH *N/ASimilar LS BMDand BMC PTH, uNTX6 months* 25(OH) D*Similar OCSimilar Ca2 , alkphos, PTH,25(OH)DSimilar BMD inpremenopausal,Postmenopausal FN, ease awareness,supplement and screen MBDVitamin D supplementationis needed in obeseFurther studiesAggressive and earlysupplementation afterRYGB, screen Ca2 metabolism pre-opFurther studies to examineif vitamin D canprevent MBDStudy recommendationsCase seriesNo baseline dataSmall nDefined vitamin Ddef. 20 ng/ml, nobaseline dataShort duration offollow-upSmall nStudy weakness[67][66][65][60][62][62]Ref.*Statistical significance; ‡Not statistically significant.Alk phos: Alkaline phosphatase; BMC: Bone mineral content; BMD: Bone mineral density; BPD: Biliopancreatic diversion; CNT: Control; def: Deficiency; FN: Femoral neck; LL-GBP: Long limb gastric bypass;LS: Lumbar spine; MBD: Metabolic bone disease; MVA: Multivitamin; n: Sample size; N/A: Not available; OC: Osteocalcin; PTH: Parathyroid hormone; RYGB: Roux–en-Y gastric bypass; SL-GBP: Short limbgastric bypass; TH: Total hip; uNTX: Urinary N- telopeptide; Wt: Weight.Prospectiveobservational6 monthsProspectiveYoussefet al.3 yearsRetrospectiveobservational,controlledGoodeet al.DurationDesignStudyTable 1. Studies assessing vitamin D and markers for metabolic bone disease with Roux-en-Y gastric bypass surgery. (cont.)REVIEW – Zalesin, Miller, Nori Janosz et al.future science group
Vitamin D deficiency after gastric bypass surgery – REVIEWof patients had an elevated PTH level with meantime to development after surgery at9.1 months. There was a 2.5-fold elevated risk inthe African–American population comparedwith the Caucasian population (p 0.05), and a1.8-times higher risk in subjects aged over45 years compared with younger counterparts(p 0.05), to develop secondary hyperparathyroidism. Vitamin D deficiency, which wasdefined as less than 20 ng/ml, was described in18.2% of the patients, while 30% of patientswith secondary hyperparathyroidism had concomitant vitamin D deficiency. This study likewise identified factors other than vitamin Ddeficiency as predictive of MBD, namely age andrace. The authors cautioned that aggressive supplementation with calcium and vitamin D isnecessary due to cumulative effects of malabsorption with hypovitaminosis D magnifyingrisks of MBD.Johnson et al. prospectively monitored BMD,calcium, PTH and vitamin D and comparedbaseline results to annual postoperative findingsfor 2 years subsequently [61]. Calcium intake recommendations were 600–1000 mg with400–800 IU of vitamin D per day. A total of226 patients, who had undergone RYGB, andseven who underwent biliopancreatic diversion(BPD), were included in a combined analysis,with each patient serving as their own control.They found that 15 patients were osteopenic preoperatively, and three subjects developed osteopenia within the first year. None of the studypatients had or developed osteoporosis. At the1 year evaluation (n 116), total forearm BMDhad decreased 0.55 2.43% (p 0.03), radiusBMD increased 1.85 4.06% (p 0.008), whiletotal hip and lumbar spine BMD decreased by9.27 3.42% (p 0.001), and 4.53 3.83 %(p 0.001), respectively. At the second year(n 37), BMD at the total forearm decreased anadditional 3.62 3.56 % (p 0.001), while nosignificant further losses at the total hip or lumbar spine were appreciated. At the third year follow-up (n 12), there were no statisticallysignificant losses noted at total forearm, radiusbone, total hip or lumbar spine. In fact, BMDs atthe spine and hip areas were not significantly different from baseline after the first year, indicatingthat there may be regain in BMD in somepatients over time at the hip, spine and total forearm locations among the remaining small sample.Calcium trended in a declining pattern, whilePTH and 25-hydroxyvitamin D levels bothincreased after surgery; however, none of thesefuture science groupwww.futuremedicine.comparameters were significantly changed. Thisstudy demonstrates that the rate of bone loss isgreatest after the first year, and plateaus or evenslightly improves in subsequent years. This boneloss appeared partially independent from avitamin D mechanism, as there was no association between vitamin D or PTH levels to BMDresults in this study. The authors indicate thatbone loss is not an ongoing process after the firstyear; however, they do advocate annual screeningto detect MBD and BMD changes in individualsat increased risk.Goode et al. assessed 44 females (23 werepremenopausal and 21 postmenopausal), 3 ormore years following RYGB [62]. There was anaverage weight loss of 31% and a current BMIaverage of 34 kg/m2. A comparison of bone mineral content (BMC), bone turnover markers,PTH levels and 25-hydroxyvitamin D levels withan age- and weight-matched historical controlgroup who had previously been assessed for bonemass (n 65). This study achieved a 72% followup rate and found no difference in BMC in premenopausal groups (42 5 years); however, inpostmenopausal women (55 7 years), BMCwas higher in the lumbar spine (p 0.05) andlower in the femoral hip (p 0.001). A subgroupof 13 postoperative RYGB patients with a meanBMI of 34 kg/m2, seven premenopausal and sixpostmenopausal, with low BMCs, were providedsupplements of 1200 mg of calcium and 8 µg ofvitamin D per day for 6 months, while BMC andserum bone markers were monitored. This groupwas compared with a 13-member weightmatched control group, seven premenopausaland six postmenopausal, who had previouslycompleted a 6-month unsupplemented weightmaintenance study. No difference in BMC wasnoted in the subgroup analysis (100% follow-uprate) with supplementation. PTH and serummarkers of bone turnover were higher in theRYGB group (p 0.001), yet were notsignificantly altered with supplementation.While there was a significant increase in25-hydroxyvitamin D in RYGB patients withsupplementation (p 0.0001), no differences in25-hydroxyvitamin D or osteocalcin were demonstrated between control and postoperativegroups. This study found MBD risks to be moreprominent with postmenopausal status at corticalbone sites, namely the femoral neck and radius,and raised the concern that standard vitamin Dand calcium supplementation may be insufficient to suppress PTH and prevent bone lossafter bariatric surgery.567
REVIEW – Zalesin, Miller, Nori Janosz et al.Direct correlation of vitamin D levels andmarkers of MBD after surgery have been noted.In another 243-subject study led by the Johnsongroup [63], a prospective evaluation of the effectsof RYGB, both long limb (n 41) (LL-GBP),defined as a Roux limb greater than 100cm, andshort limb, defined as 100cm or more (n 202)(SL-GBP), on calcium, vitamin D and PTH wascompiled. BMI levels were greater in the LLGBP measuring 60.6 8.3 kg/m2, as opposed tothe SL-GBP group, which was 49.1 8.8 kg/m2.All study subjects were supplemented with 1200mg of calcium and 800 IU of vitamin D.Patients in the SL-GBP were followed for amean of 3.1 3.6 years, while the LLGBP group was followed for 5.7 2.5 years(p 0.0001). They found that the average25-hydroxyvitamin D level was lower in the LLGBP group, 16.8 10.8 ng/ml, while the SLGBP group levels were 22.7 11.1 ng/ml (p 0.0022). The average PTH levels were higher inthe LL-GBP group 113.5 88.0 compared withSL-GBP 74.5 52.7 pg/ml (p 0.0002). Studypatients had normal calcium levels without differences between SL and LL-GBP groups. Inpatients with low vitamin D levels, (defined as 8.9 ng/ml), 89% had an elevated PTH,(defined as 65 pg/ml). In patients with avitamin D level up to 8.9 ng/ml, 58% had anelevated PTH. When evaluating 25-hydroxyvitamin D at less than 30 ng/ml, 55.1% hadsecondary hyperparathyroidism while those withvitamin D level up to 30 ng/ml, 28.5% had secondary hyperparathyroidism (p 0.0007). Alinear correlation revealed that as vitamin D levels decrease (p 0.005) PTH levels linearlyincrease (p 0.001), which highlighted a directrelationship of bone turnover and vitamin Ddeficiency in this postoperative setting. Thistrend appeared more prominent the longerpatients were followed after RYGB. TheLL-GBP population had a greater risk for hypovitaminosis D and secondary hyperparathyroidism, indicating that a greater surgicallyimposed malabsorption produces greater risksfor MBD. The authors recommended maintaining 25 hydroxyvitamin D levels greater than30 ng/ml.Ott et al. retrospective
William Beaumont Hospital, Division of Nutrition and Preventive Medicine, 4949 Coolidge HighwayRoyal Oak, Michigan 48073, USA Tel.: 1 248 655 5900 Fax: 1 248 655 5901 kzalesin@beaumont.edu Keywords: bariatric surgery, cholecalciferol, metabolic bone disease, obesity, vitamin D