Transcription
Regional Continuing Education ProgramTuesday, April 19, 2011Baxter Regional Medical Center – Mtn. Home, AR6:30pm to 9:10pmOld Bugs, New Tricks: Multi-Drug Resistant InfectionsACPE # 0004-0000-11-016-L01-P1.0 hr*This CE activity will be Knowledge based.Presented by:Maggie Miller, PharmDMedication Assistance Services to Area ResidentsACPE # 0004-0000-11-017-L04-P1.0 hr*This CE activity will be Knowledge based.Presented by:Dennis Moore, PharmDBrought to you by:
ObjectivesOld Bugs, New Tricks:Multi-Drug Resistant InfectionsMaggie Miller, Pharm.D.White River Medical CenterBatesville, AR Discuss resistance patterns for multi-drugresistant organismsg g multi-drugg resistant Discuss how emerginginfections are affecting healthcare. Review the steps needed to prevent thespread of multi-drug resistant organisms.In the U.S.most antibiotic usage takes place ina.b.cc.d.The Hospital settingOutpatient treatmentAgricultural usageWater treatmentCauses of AbRNatural Causes – the bacteria change– Selective pressure– Mutation– Gene transferCauses of AbRSocietal Pressures – we force thebacteria to change– Inappropriate usage– Inadequate diagnostics/broad spectrum usage– Hospital usage in the critically ill– Agricultural usage (this one is decreasingrapidly)A Quick AbR Timeline 1947 – PCN resistance appears. Four years after initial massproduction 1961 – Methicillin resistant S. aureus (MRSA) . One yearafter methicillin was introduced. 1968 – U.S.U S soldiers in Asia ‘acquired’acquired PCN resistantSTD’s. 1983 – Hospital-acquired PCN-resistant intestinal infectionsof E. faecium make a debut 1993- 13,300 hospital patients died from AbR infections 1999 – Community-acquired MRSA was identified in theUS1
A Quick AbR Timeline 1997-2007 – no real ‘blockbuster’ antibiotics developed(Zyvox was the biggest drug to hit the market but s till didnot meet its pre-release expectations) 2007- present – a few ‘new’ antibiotics are beingdeveloped These drugs include ‘new’ classes of antibiotics and newderivatives of older antibiotics. Some of these drugs willbe approved by the FDA in the next few years but the juryis still out on their true effectiveness.Definitions Colonization – organism is present on aperson but doesn’t cause a specific immuneresponse or infection Pathogen – organism that can cause aninfection Contaminant – organism that grew in thesample but is not the pathogenOrganisms Methicillin-resistant Staphylococcus aureus(MRSA)y resistant Enterococcus ((VRE)) Vancomycin Clostridium difficile (Cdif)Staphylococcus aureus Hardiest non-spore forming bacteria Major human pathogen– Pneumonia– Skin infections– Sepsis Most humans are colonized Can contaminate clothes and linens– transfer by colonized hands or inanimateenvironmentMRSA Hospital-acquired MRSA (HA-MRSA)– Pneumonia– Bloodstream– UTI’s– Surgical – site infections Community-acquired MRSA (CA-MRSA)– SkinTreatment MRSA in/dalfopristinCeftaroline2
Treatment CA-MRSA nPlus RifampinEnterococcus Infections– UTI’s– Bloodstream– Endocarditis– Intra-abdominalC. diff. Spore forming and toxic producing bacteria Normal gut floraEnterococcus Not as virulent as S. aureusSurvive under harsh conditionsMajor habitat is GI tract of humansAbility to cause infection – superinfectionsUsually people with infections arecolonized with the organism VRETreatment (VRE) Linezolid Quinupristin/dalfopristinTreatment Metronidazole oral or IV Vancomycin oral only– 20% hospitalized patients Causes antibiotic associated diarrhea Main transmission is person-to-person– Wash Hands!- no alcohol-based handantiseptics3
Big PictureStrategies to prevent AbRA Bad Moon RisingMicrobes that are becoming increasingly resistant todrugs Food borne bacteria such as E.coli, Salmonella,and Campylobacter.Campylobacter PCN – resistant Streptococci PCN – resistant Staphylococci STD’s TB HIV1. Prevent infection – wash your hands2. Seek treatment of infections early andyeffectively3. Use antibiotics wisely4. Prevent transmission – stay home whenyou are febrile.Clinical Measures9Practice antibiotic control/stewardship9Use local data9Treat infection not contamination9Treat infection not colonization9Stop antibiotic treatment as soon asclinically possibleConclusion Personally - be wise in the usage of antibiotics Clinically - be selective and specific in the usageof antibiotics Use common sense– Wash your hands!!– Follow protocols– Learn to hate long term usage of broad spectrumantibiotics– Ask questions about diagnostics and usageReferences Cohen SH, Gerding DN, et al. Clinical Practice Guidelines for Clostridium difficileInfection in Adults: 2010 Update by the Society for Healthcare Epidemiology ofAmerica (SHEA) and the Infectious Diseases Society of America (IDSA). InfectControl Hosp Epidemiol 2010; 31(5):431-455. Liu C, Bayer A, et al. Clinical Practice Guidelines by the Infectious Diseases society ofAAmericai forf theth treatmentt tt off Methicillin-ResistantM thi illi R i t t StaphlococcusSt hlAureusAInfectionsI f tiiniAdults and Children. Clinical Infectious Diseases 2011;1-38 Mandell GL, Bennett JE, et al. Mandell, Douglas, and Bennett’s Principles and Practiceof Infectious Diseases 5th ed. Philadelphia, PA: Churchill Livingstone; 2000. Shlaes DM, Gerding DN, et al. Society for Healthcare Epidemiology of America andInfectious Diseases Society of America Joint committee on the Prevention ofAntimicrobial Resistance: Guidelines for the Prevention of Antimicrobial Resistance inHospitals. Clinical Infectious Diseases 1997;25:584-99.Thank you4
Questions5
4/18/2011Educational ObjectivesMEDICATIONASSISTANCE PROGRAM Discuss Availability of MAP Services throughNC‐AHEC Provide Contact information to participants Discussimethodsh d off iimprovement iin servicesiNORTH CENTRAL AREA HEALTHEDUCATION CENTERDennis F. Moore, Pharm.D.AHEC‐NC Health Rankings Established newAHEC in North CentralArkansas in 20072011 AR County Health RankingsHealth Needs of Population Baxter County has 26% over 65, Independenceis youngest with approx 18% over 65 Higher than state averages in obesity,smoking cancersmoking,cancer, cardiovascular illness The 15 cents of the health care dollar thatgoes to medications determines—manytimes—how the other 85 cents is used.1
4/18/2011AHEC Mission To improve the supply and distribution of careprofessionals in Arkansas, with an emphasison primary care, throughcommunity/academicit / d i educationald tilpartnerships, to increase quality care for allArkansansMedication Assistance Programs Miscellaneous programs—usually industrysponsored—that provide prescriptionmedications/supplies for those unable to affordpsuch products Developed by companies based on philanthropy,political or public relations purposes. Variable as to guidelines and requirements Nearly impossible to navigate unless staff time isdevoted to processGeneral Criteria for ProgramParticipation Not eligible for benefits through otherpublic/private program Based on total household income—most at200% of FPL Some for Medicare Part‐D, based on % ofannual income, some for “donut hole” Some “case‐by‐case” due to financial/medicalhardshipsPatients Generally Excluded Those with prescription drug insurancecoverage Those with household incomes over 200% ofFPL Those with other assets(stocks/bonds/cd’s) Those unwilling to cooperate with writtendocumentation requirementsDrugs We Try to Avoid Opioid agonist Some psychotherapeutic agents—howeverMD’s are sometimes unwilling to write for 90day supplies that some companies demandMechanism of DistributionProvider’s officePatient’s homeSome will allow eitherSome provide the card to deliver to you—thepharmacist—to obtain medication We never accept medications in our facility 2
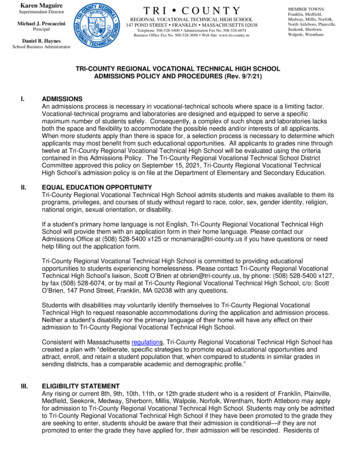
4/18/2011# of Patients ServedNorth Central AHECAWPNorth Central AHEC700 600,000.00600 500,000.00500 400,000.00400200930020102002011*2009 300,000.00 ,2010 200,000.00100 100,000.000 0.002011** 2011 – January through March* 2011 – January through MarchWho to Contact?Discussion Marion, Baxter, Fulton, Izard, and Sharp—Mary Worthern, 870‐251‐6478—office inSalem, Ash Flat and Mountain Home. Searcy,Searcy Van Buren,Buren CleburneCleburne, StoneStone, andIndependence—Tina Venteicher, 870‐251‐7126—office in Mountain View and Batesville How could we help you and your patients?3
ACPE # 0004-0000-11-016-L01-P 1.0 hr *This CE activity will be Knowledge based. Presented by: Maggie Miller, PharmD Medication Assistance Services to Area Residents ACPE # 0004-0000-11-017-L04-P 1.0 hr *This CE activity will be Knowledge based. Presented by: Dennis Moore, PharmD Brought to you by: